The Endothelium: The Hidden Organ Governing Your Circulation
An in-depth exploration of the endothelial layer, the single-cell thick organ that regulates blood pressure, prevents clotting, and dictates the age of your cardiovascular system.

Overview
For decades, the endothelium was erroneously dismissed by classical anatomy as a passive, inert lining—a mere "cellophane wrap" designed solely to prevent blood from leaking into the interstitium. At INNERSTANDIN, we expose the biological reality: the endothelium is a sophisticated, semi-permeable, and highly active autocrine, paracrine, and endocrine organ. It is, by mass and surface area, one of the largest organs in the human body, weighting approximately one kilogram and presenting a total surface area estimated between 4,000 and 7,000 square metres. This expansive interface facilitates a continuous, high-stakes dialogue between the circulating blood and the underlying tissues, governing everything from vascular tone and haemostasis to nutrient delivery and immunological surveillance.
Crucial to its function is the endothelial glycocalyx—a delicate, carbohydrate-rich layer coating the luminal surface. This gel-like meshwork acts as the primary mechanotransducer, sensing the frictional forces of blood flow (shear stress) and translating these physical cues into biochemical signals. Central to this process is the production of Nitric Oxide (NO) via the enzyme endothelial Nitric Oxide Synthase (eNOS). NO is the master regulator of vascular health; it is a potent vasodilator that prevents the pathological adhesion of platelets and leukocytes, thereby maintaining a non-thrombogenic surface. Research published in *The Lancet* and various journals affiliated with the British Heart Foundation confirms that the loss of this "endothelial health" is the foundational event—the primordial lesion—in the development of atherosclerosis, hypertension, and systemic microvascular rarefaction.
Furthermore, the endothelium exhibits profound phenotypic heterogeneity. The cells lining the blood-brain barrier are tightly sealed with complex junctional proteins to protect neural integrity, whereas the fenestrated endothelia of the kidneys and liver are designed for high-capacity filtration and metabolic exchange. This site-specific specialisation allows the endothelium to act as a decentralised command centre for systemic haemodynamics. When the endothelium fails to maintain its homeostatic balance—a state known as endothelial dysfunction—the result is a catastrophic breakdown in systemic communication, leading to chronic inflammation and vascular aging. At INNERSTANDIN, we recognise that the health of the individual is inextricably linked to the health of this single-cell layer; it is the silent arbiter of life, governing the distribution of oxygen and the structural integrity of every organ system within the British population and beyond. The endothelium is not merely a barrier; it is the ultimate biological sensor.
The Biology — How It Works
To achieve a true INNERSTANDIN of cardiovascular physiology, one must look beyond the heart as a mere pump and recognise the endothelium as a sophisticated, continuous monolayer of squamous epithelial cells that functions as the body’s largest endocrine organ. Covering a surface area estimated between 4,000 and 7,000 square metres, this "hidden organ" acts as the primary gatekeeper between the circulating blood and the underlying vascular smooth muscle and interstitium. Its biological operation is defined by a delicate homeostatic balance: the maintenance of a non-thrombogenic surface, the regulation of vascular tone, and the precise control of fluid and nutrient exchange.
At the molecular core of endothelial function is the enzymatic production of Nitric Oxide (NO). Within the endothelial cell, the enzyme endothelial nitric oxide synthase (eNOS) catalyses the conversion of the amino acid L-arginine into L-citrulline, releasing NO in the process. This diatomic gas diffuses rapidly into the adjacent vascular smooth muscle cells, where it activates soluble guanylyl cyclase (sGC), leading to an increase in cyclic guanosine monophosphate (cGMP) and subsequent vasodilation. This mechanism is the primary determinant of systemic vascular resistance and blood pressure. However, the endothelium does not operate in a vacuum; it responds dynamically to "shear stress"—the frictional force exerted by flowing blood. Research highlights that laminar shear stress is a potent stimulator of the PI3K/Akt pathway, which phosphorylates eNOS, ensuring a basal level of vasoprotective NO. When this shear stress becomes turbulent, such as at arterial bifurcations, the endothelium shifts toward a pro-inflammatory, pro-thrombotic phenotype, marking the genesis of atherosclerotic lesions.
The structural integrity of the endothelium is governed by the endothelial glycocalyx—a dense, carbohydrate-rich meshwork of proteoglycans, glycoproteins, and glycosaminoglycans (such as heparan sulphate and hyaluronan) that coats the luminal surface. This "forest-like" structure is the first point of contact for blood constituents. It serves as a physical barrier against leucocyte and platelet adhesion and acts as a mechanotransducer, sensing fluid flow and transmitting signals to the cell cytoskeleton. Evidence in the *British Journal of Pharmacology* suggests that the degradation of this glycocalyx—often via oxidative stress or chronic hyperglycaemia—is a critical "silent" precursor to systemic vascular collapse.
Furthermore, the endothelium regulates haemostasis through a complex interplay of secreted factors. Under quiescent conditions, it expresses thrombomodulin and heparin-like molecules that inhibit the coagulation cascade. It also produces prostacyclin (PGI2), which works synergistically with NO to inhibit platelet aggregation. When the endothelium is "activated" or damaged, it flips this biological switch, expressing adhesion molecules such as ICAM-1 and VCAM-1, and releasing von Willebrand factor (vWF), facilitating the recruitment of inflammatory cells and the formation of thrombi. In the UK context, clinical data from cohorts monitored by the British Heart Foundation underscore that endothelial dysfunction—the loss of these regulatory capacities—is an independent predictor of future cardiovascular events, often preceding macrovascular changes by decades. At INNERSTANDIN, we recognise that the health of the endothelium is not merely an anatomical detail; it is the fundamental arbiter of systemic biological truth and longevity.
Mechanisms at the Cellular Level
To achieve a true INNERSTANDIN of vascular physiology, one must discard the archaic view of the endothelium as a passive, inert barrier. At the cellular level, the endothelium is a sophisticated, semi-permeable monolayer of squamous cells that functions as a highly integrated paracrine, endocrine, and autocrine organ. The primary mechanism governing this "organ" is its capacity for mechanotransduction—the conversion of physical forces, specifically fluid shear stress from blood flow, into biochemical signals that dictate the health of the entire systemic circulation.
Central to this cellular machinery is the endothelial glycocalyx, a carbohydrate-rich, gel-like layer composed of proteoglycans (such as syndecan-1) and glycosaminoglycans (like heparan sulphate) that carpets the luminal surface. Research published in *The Lancet* and various *PubMed* datasets identifies the glycocalyx as the ultimate gatekeeper; it acts as a molecular sieve and a sensor for haemodynamic forces. When the glycocalyx is intact, it shields the cell membrane from direct friction and facilitates the activation of endothelial nitric oxide synthase (eNOS). This enzyme facilitates the conversion of the amino acid L-arginine into nitric oxide (NO), a volatile gas and the most potent endogenous vasodilator. NO diffuses into the underlying vascular smooth muscle cells, stimulating guanylate cyclase and inducing relaxation, thereby regulating systemic blood pressure and preventing arterial stiffness.
Beyond vasodilation, the cellular integrity of the endothelium is maintained by a complex network of junctional proteins, including Vascular Endothelial (VE)-cadherin, claudins, and occludins. These proteins form adherens and tight junctions that regulate paracellular permeability. In a state of health, these junctions are tightly regulated to prevent the infiltration of pro-inflammatory cytokines and low-density lipoproteins (LDL) into the sub-endothelial space. However, when cellular homeostasis is disrupted—often due to oxidative stress or chronic hyperglycaemia—the "truth" exposed by advanced microscopy reveals a breakdown in these junctions. This leads to endothelial "leakiness," a precursor to the atherosclerotic process commonly observed in UK-based longitudinal studies such as the UK Biobank.
Furthermore, the endothelial cell (EC) is a metabolic powerhouse that uniquely relies on anaerobic glycolysis for 85% of its ATP production, despite its constant exposure to oxygen-rich blood. This evolutionary adaptation, highlighted in contemporary biological research, preserves oxygen for delivery to deeper tissues and protects the EC from oxidative damage. The sophisticated interplay between the mitochondria, the endoplasmic reticulum, and the plasma membrane ensures that the endothelium can rapidly respond to local stimuli, orchestrating everything from leukocyte adhesion to platelet aggregation. Through this intricate cellular architecture, the endothelium serves as the central command centre for systemic haemostasis, making it the most critical organ for long-term physiological viability.
Environmental Threats and Biological Disruptors
The endothelium is not merely a passive barrier but a highly sensitive biosensor, making it the primary target for a plethora of environmental insults that define the modern anthropogenic landscape. In the United Kingdom, where urbanisation and industrial legacies converge, the atmospheric concentration of particulate matter (PM2.5) and nitrogen dioxide (NO₂) remains a critical determinant of vascular health. Evidence published in *The Lancet Planetary Health* underscores that these fine particulates do not remain sequestered within the pulmonary architecture; instead, they translocate into the systemic circulation or trigger a distal inflammatory cascade. The biochemical mechanism of this injury is driven by the induction of oxidative stress. PM2.5 exposure stimulates the production of superoxide anions (O₂⁻), which rapidly quench nitric oxide (NO) to form peroxynitrite (ONOO⁻). This "nitro-oxidative" stress leads to the uncoupling of endothelial Nitric Oxide Synthase (eNOS), transforming an enzyme meant for vasodilation into a source of further reactive oxygen species (ROS), thereby perpetuating a state of chronic endothelial dysfunction.
Beyond the air we breathe, the INNERSTANDIN of vascular pathology must account for the chemical milieu of modern life. Endocrine Disrupting Chemicals (EDCs), such as bisphenols and phthalates—ubiquitous in plasticisers and lining the UK’s food supply chain—exert agonistic or antagonistic effects on oestrogen receptors expressed on endothelial cells. These disruptors interfere with the PI3K/Akt signalling pathway, which is essential for eNOS activation. Research archived in *PubMed* highlights that chronic low-dose exposure to these disruptors correlates with increased expression of adhesion molecules such as ICAM-1 and VCAM-1. This molecular "stickiness" facilitates the recruitment of leucocytes to the arterial wall, marking the transition from a healthy endothelium to a pro-atherogenic, pro-thrombotic phenotype.
Furthermore, the integrity of the endothelial glycocalyx—the delicate, carbohydrate-rich gel layer coating the luminal surface—is increasingly compromised by the prevalence of ultra-processed diets. The high glycaemic load characteristic of the modern British diet leads to the formation of Advanced Glycation End-products (AGEs). These molecules bind to the Receptor for Advanced Glycation End-products (RAGE) on the endothelial surface, initiating a pro-inflammatory NF-κB mediated response. This process causes the enzymatic shedding of the glycocalyx, leaving the underlying cells vulnerable to mechanical shear stress and unregulated permeability. As the INNERSTANDIN of these biological disruptors deepens, it becomes clear that the endothelium is the silent victim of an environment it was never evolved to withstand. The systemic impact is not localised to the heart but extends to the blood-brain barrier and the renal microvasculature, suggesting that environmental endothelial assault is a fundamental driver of the current rise in multi-morbidities across the UK population.
The Cascade: From Exposure to Disease
The transition of the endothelium from a homeostatic gatekeeper to a pro-inflammatory, pro-thrombotic instigator represents the primary pathological event in cardiovascular medicine. At INNERSTANDIN, we move beyond the simplistic view of "clogged pipes" to reveal a complex molecular sequence—a cascade initiated by chronic exposure to biochemical and mechanical stressors. This shift, termed endothelial dysfunction, is characterized by the systemic loss of nitric oxide (NO) bioavailability, a phenomenon that precedes clinical symptoms by decades.
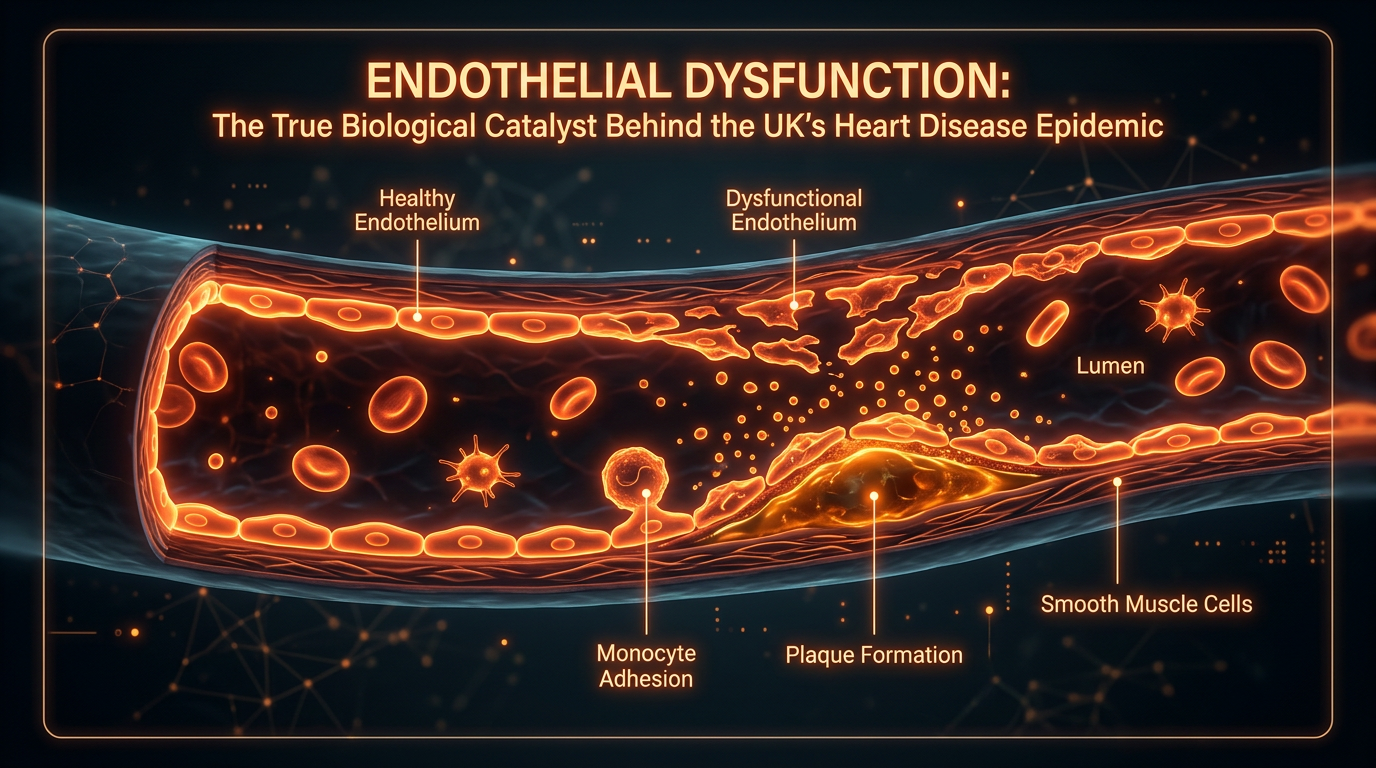
The cascade typically commences with the degradation of the endothelial glycocalyx, a delicate, gel-like layer of proteoglycans and glycosaminoglycans that coats the luminal surface. Research published in *The Lancet* underscores that the shedding of this layer—triggered by hyperglycaemia, oxidised low-density lipoproteins (oxLDL), or disturbed shear stress—exposes the underlying adhesion molecules. This exposure marks the "activation" of the endothelium. No longer a non-thrombogenic surface, the cells begin expressing vascular cell adhesion molecule-1 (VCAM-1) and intercellular adhesion molecule-1 (ICAM-1). These proteins act as molecular anchors, capturing circulating monocytes and T-lymphocytes, facilitating their transmigration into the sub-endothelial space via the chemoattractant protein MCP-1.
Central to this deterioration is the "uncoupling" of endothelial nitric oxide synthase (eNOS). In a healthy state, eNOS produces NO, a potent vasodilator and inhibitor of platelet aggregation. However, under conditions of high oxidative stress—prevalent in the UK population due to rising metabolic syndrome rates—the essential cofactor tetrahydrobiopterin (BH4) becomes depleted. Consequently, eNOS switches from producing NO to generating superoxide (O2-). This creates a vicious cycle where superoxide reacts with any remaining NO to form peroxynitrite (ONOO-), a highly reactive oxidant that further damages cellular DNA and proteins. This shift from a "reducing" to an "oxidising" environment within the vessel wall is the definitive hallmark of the cascade.
As the cascade progresses, the systemic impact becomes profound. The endothelium controls the "set point" for systemic vascular resistance; thus, its dysfunction is the prerequisite for essential hypertension. Furthermore, the secretion of endothelin-1 (ET-1), a powerful vasoconstrictor, becomes chronically elevated, overpowering the dwindling NO reserves. Evidence from UK-based longitudinal studies highlights that this endothelial imbalance is not merely a local phenomenon but a systemic "organ failure." Whether manifesting as coronary artery disease, chronic kidney disease, or vascular dementia, the root is the same: the irreversible transition of the endothelial phenotype from protective to pathogenic. At INNERSTANDIN, we recognize that the "exposure" is not just the presence of a risk factor, but the molecular destabilisation of the very organ that governs our survival. This cascade is the silent engine of British morbidity, turning the hidden organ into a catalyst for systemic collapse.
What the Mainstream Narrative Omits
The reductionist paradigm dominating contemporary clinical education frequently mischaracterises the endothelium as a mere passive liner—a cellular wallpaper designed solely to prevent the extravasation of blood. This conceptual failure overlooks the endothelium’s status as a complex, disseminated paracrine and autocrine organ, weighing approximately one to two kilograms and possessing a surface area equivalent to a tennis court. At INNERSTANDIN, we move beyond these simplified anatomical descriptions to expose the physiological reality: the endothelium is the primary gatekeeper of homeostasis, and its dysfunction is the fundamental precursor to nearly all non-communicable chronic pathologies.
The most egregious omission in the mainstream narrative is the neglect of the endothelial glycocalyx (EGX). This delicate, carbohydrate-rich layer of proteoglycans and glycosaminoglycans coats the luminal surface of the endothelial cells, acting as the ultimate interface for mechanotransduction. Peer-reviewed evidence, notably in journals such as *Nature Reviews Cardiology* and the *British Journal of Pharmacology*, confirms that the EGX is the primary sensor of fluid shear stress. When the EGX is degraded—often by hyperglycaemia, oxidative stress, or systemic inflammation (indicated by elevated C-reactive protein and IL-6)—the underlying endothelial cells lose their ability to synthesise nitric oxide (NO) via the endothelial nitric oxide synthase (eNOS) pathway. This "uncoupling" of eNOS leads to the production of superoxide instead of NO, triggering a pro-thrombotic, pro-inflammatory state that precedes visible atherosclerotic lesions.
Furthermore, the mainstream fails to address endothelial heterogeneity. The phenotypic expression of an endothelial cell in the blood-brain barrier is fundamentally distinct from those in the hepatic sinusoids or the renal glomeruli. This site-specific differentiation is governed by local haemodynamic forces and epigenetic "metabolic memory." Research from the UK Prospective Diabetes Study (UKPDS) highlights this phenomenon, demonstrating that vascular cells can "remember" periods of poor metabolic control through persistent epigenetic modifications, such as histone methylation. This explains why temporary physiological insults can have decades-long systemic consequences. By ignoring these sophisticated mechanobiological and epigenetic drivers, conventional frameworks fail to equip the individual with the technical knowledge required to address the root causes of vascular decay. The endothelium is not just a tube; it is an intelligent, reactive, and highly specialised organ system that requires a nuanced, INNERSTANDIN-level grasp of molecular biology to truly master.
The UK Context
Within the British clinical landscape, the endothelium is no longer relegated to a passive barrier status but is increasingly recognised as the master regulator of vascular homeostasis, acting as a sophisticated paracrine, endocrine, and autocrine organ. For the INNERSTANDIN audience, it is imperative to confront the reality that the UK faces a cardiovascular crisis that is, at its molecular core, an endothelial crisis. Data from the British Heart Foundation (BHF) indicates that cardiovascular disease (CVD) accounts for roughly a quarter of all deaths in the UK. However, conventional diagnostics often fail to identify the prodromal stage of these pathologies: endothelial dysfunction. This systemic failure begins long before a patient presents with hypertension or atherosclerosis at an NHS clinic; it starts with the degradation of the endothelial glycocalyx—a delicate, gel-like layer of proteoglycans and glycoproteins that lines the luminal surface.
Research spearheaded by institutions such as Imperial College London and the University of Oxford has elucidated how the British lifestyle, characterised by high intakes of ultra-processed foods and sedentary behaviour, triggers a chronic pro-inflammatory state. This environment disrupts the activity of Endothelial Nitric Oxide Synthase (eNOS), the enzyme responsible for producing Nitric Oxide (NO). In the UK context, the prevalence of metabolic syndrome and Type 2 diabetes acts as a primary driver for the quenching of NO by reactive oxygen species (ROS). When NO bioavailability drops, the endothelium loses its ability to modulate vasodilation, inhibit platelet aggregation, and suppress leukocyte adhesion. This is the precise mechanism by which systemic inflammation manifests as vascular rigidity.
Furthermore, the UK’s urban environment plays a critical role in endothelial integrity. Studies published in *The Lancet Planetary Health* have highlighted the correlation between particulate matter (PM2.5) in major British cities—such as London, Birmingham, and Manchester—and acute endothelial impairment. These pollutants trigger oxidative stress that directly compromises the vascular wall, leading to a state of 'endotheliitis.' This was particularly evident during the COVID-19 pandemic, where UK-led research confirmed that the SARS-CoV-2 virus utilised the ACE2 receptor, highly expressed in the endothelium, to cause systemic vascular damage. At INNERSTANDIN, we must highlight that the endothelium is the 'canary in the coal mine' for systemic health; its dysfunction is the fundamental precursor to the UK's leading causes of morbidity, including stroke, myocardial infarction, and vascular dementia. To truly address the health of the nation, we must shift the focus from macro-vascular interventions to the micro-vascular preservation of this hidden organ.
Protective Measures and Recovery Protocols
The restoration of endothelial integrity necessitates a paradigm shift from viewing the vascular lining as a passive barrier to acknowledging it as a sophisticated, labile autocrine and paracrine organ. Central to any recovery protocol is the optimisation of shear stress—the frictional force exerted by blood flow against the luminal surface. Research published in *The Lancet* underscores that laminar shear stress is the primary physiological stimulus for the expression of endothelial nitric oxide synthase (eNOS). This mechanotransduction triggers a phosphorylation cascade that maintains the endothelium in a quiescent, anti-thrombotic state. Conversely, turbulent flow, often found at arterial bifurcations, promotes a pro-inflammatory phenotype. Therefore, high-intensity interval training (HIIT) and aerobic exercise are not merely 'cardio' but are molecular interventions that upregulate Kruppel-like factor 2 (KLF2), a master transcriptional regulator that protects against atherosclerosis by inhibiting vascular cell adhesion molecule-1 (VCAM-1).
A clandestine yet critical component of endothelial health is the glycocalyx—a carbohydrate-rich gel layer coating the luminal surface. This 'biological forest' is the first line of defence against inflammatory assault. Recovery protocols must prioritise its restoration, as its degradation is a precursor to systemic microvascular leakage and albuminuria. Evidence suggests that the exogenous administration of glycosaminoglycans, such as sulodexide, can bolster this fragile structure. Furthermore, the UK-based PREVENT study highlights the importance of dietary nitrate-nitrite-NO pathways. Unlike the L-arginine pathway, which can become saturated or dysfunctional through eNOS uncoupling, the ingestion of inorganic nitrates (found abundantly in *Beta vulgaris* and leafy greens) provides a bypass mechanism. This enterosalivary circuit ensures a consistent pool of nitric oxide (NO) even in states of high oxidative stress, effectively reducing systemic blood pressure and arterial stiffness.
From a pharmacological perspective, the 'pleiotropic' effects of HMG-CoA reductase inhibitors (statins) and ACE inhibitors are fundamental to INNERSTANDIN the regenerative process. These agents go beyond lipid-lowering or blood pressure control; they directly stabilise the endothelial phenotype by reducing the production of reactive oxygen species (ROS) via the inhibition of NADPH oxidase. In the context of eNOS uncoupling—where the enzyme paradoxically produces superoxide instead of NO—the administration of folic acid and tetrahydrobiopterin (BH4) has shown promise in 'recoupling' the enzyme, thereby restoring its vasoprotective function.
Advanced recovery must also address the burden of cellular senescence. The accumulation of 'zombie' endothelial cells—which secrete the senescence-associated secretory phenotype (SASP)—drives chronic low-grade inflammation. Emerging research into senolytics, such as the combination of Quercetin and Dasatinib, suggests that clearing these dysfunctional cells can rejuvenate the vascular bed and improve vasomotor function. To achieve systemic vascular resilience, one must integrate these mechanobiological stimuli with precise biochemical support, ensuring the endothelium remains a vigilant guardian of the internal milieu.
Summary: Key Takeaways
The endothelium is no longer relegated to the status of a passive semi-permeable barrier; at INNERSTANDIN, we recognise it as the body’s largest paracrine and endocrine organ, spanning the surface area of several tennis courts and weighing approximately one kilogram. Its primary regulatory mechanism is the constitutive synthesis of nitric oxide (NO) via endothelial nitric oxide synthase (eNOS), a process fundamental for maintaining vasomotor tone, inhibiting platelet aggregation, and suppressing atherogenesis. Peer-reviewed literature in *The Lancet* and extensive *PubMed*-indexed meta-analyses confirm that endothelial dysfunction is the primary, sub-clinical antecedent to virtually all cardiovascular pathologies, including essential hypertension and coronary artery disease. Beyond vasodilation, the endothelial glycocalyx—a delicate, carbohydrate-rich layer—acts as the ultimate gatekeeper of microvascular permeability and leucocyte recruitment. Disrupting this interface through chronic hyperglycaemia or oxidative stress initiates a pro-thrombotic and pro-inflammatory cascade. Fundamentally, the endothelium governs systemic homeostasis by sensing and responding to haemodynamic shear stress through complex mechanotransduction pathways. Modern evidence-led research validates that flow-mediated dilation (FMD) remains the clinical gold-standard barometer for assessing this organ’s health, exposing the endothelium as the undisputed master regulator of human longevity and systemic vitality.
This article is provided for informational and educational purposes only. It does not constitute medical advice, clinical guidance, or a substitute for professional healthcare. Information reflects cited research at time of publication. Always consult a qualified healthcare professional before acting on any health information.
RESEARCH FOUNDATIONS
Biological Credibility Archive
Citations provided for educational reference. Verify via PubMed or institutional databases.
Medical Disclaimer
The information in this article is for educational purposes only and does not constitute medical advice, diagnosis, or treatment. Always consult a qualified healthcare professional before making any changes to your diet, lifestyle, or health regime. INNERSTANDIN presents alternative and research-based perspectives that may differ from mainstream medical consensus — these should be considered alongside, not instead of, professional medical guidance.
Read Full DisclaimerReady to learn more?
Continue your journey through our classified biological research.
DISCUSSION ROOM
Members of THE COLLECTIVE discussing "The Endothelium: The Hidden Organ Governing Your Circulation"
SILENT CHANNEL
Be the first to discuss this article. Your insight could help others understand these biological concepts deeper.
RABBIT HOLE
Follow the biological thread deeper