Thiamine Depletion via Modern UK Stimulants
High consumption of alcohol, coffee, and refined sugar in the UK accelerates the depletion of Vitamin B1. This piece details the resulting disruption of the citric acid cycle and neurological energy failure.
Overview
In the hierarchy of human biochemistry, few molecules hold as much sovereign power over our vitality as Vitamin B1, or Thiamine. Often relegated to the footnotes of nutritional science as a "preventative for Beriberi," thiamine is, in reality, the fundamental spark plug of the human engine. It is the gatekeeper of mitochondrial energy production, the essential cofactor for the conversion of fuel into life-sustaining ATP. Yet, across the United Kingdom, a silent catastrophe of metabolic failure is unfolding.
The modern British lifestyle, characterised by a relentless reliance on stimulants—specifically alcohol, caffeine, and refined carbohydrates—has created a "high-calorie malnutrition" epidemic. We are a nation that is overfed but metabolically starving. This article aims to expose the mechanisms by which common social habits in the UK systematically strip the body of thiamine, leading to a state of neurological energy failure that mimics many of the "mystery" chronic illnesses of the 21st century.
From the high-street coffee chains to the pervasive pub culture and the ubiquity of ultra-processed "convenience" foods, the environmental pressure on our thiamine stores is unprecedented. When thiamine levels drop, the Citric Acid Cycle—the core of our cellular respiration—stalls. The result is a cascade of systemic dysfunction: brain fog, autonomic instability, cardiovascular strain, and psychiatric distress. It is time to move beyond the antiquated notion that B1 deficiency is a relic of the Victorian era and recognise it as a primary driver of modern British morbidity.
The Biology — How It Works

Magnesium Blend – The Most Important Mineral
A high-bioavailability mineral blend designed to support over 300 essential biochemical reactions, from energy production to muscle relaxation. This formula helps combat daily fatigue while providing the foundational support your nervous system and bones require.
Vetting Notes
Pending
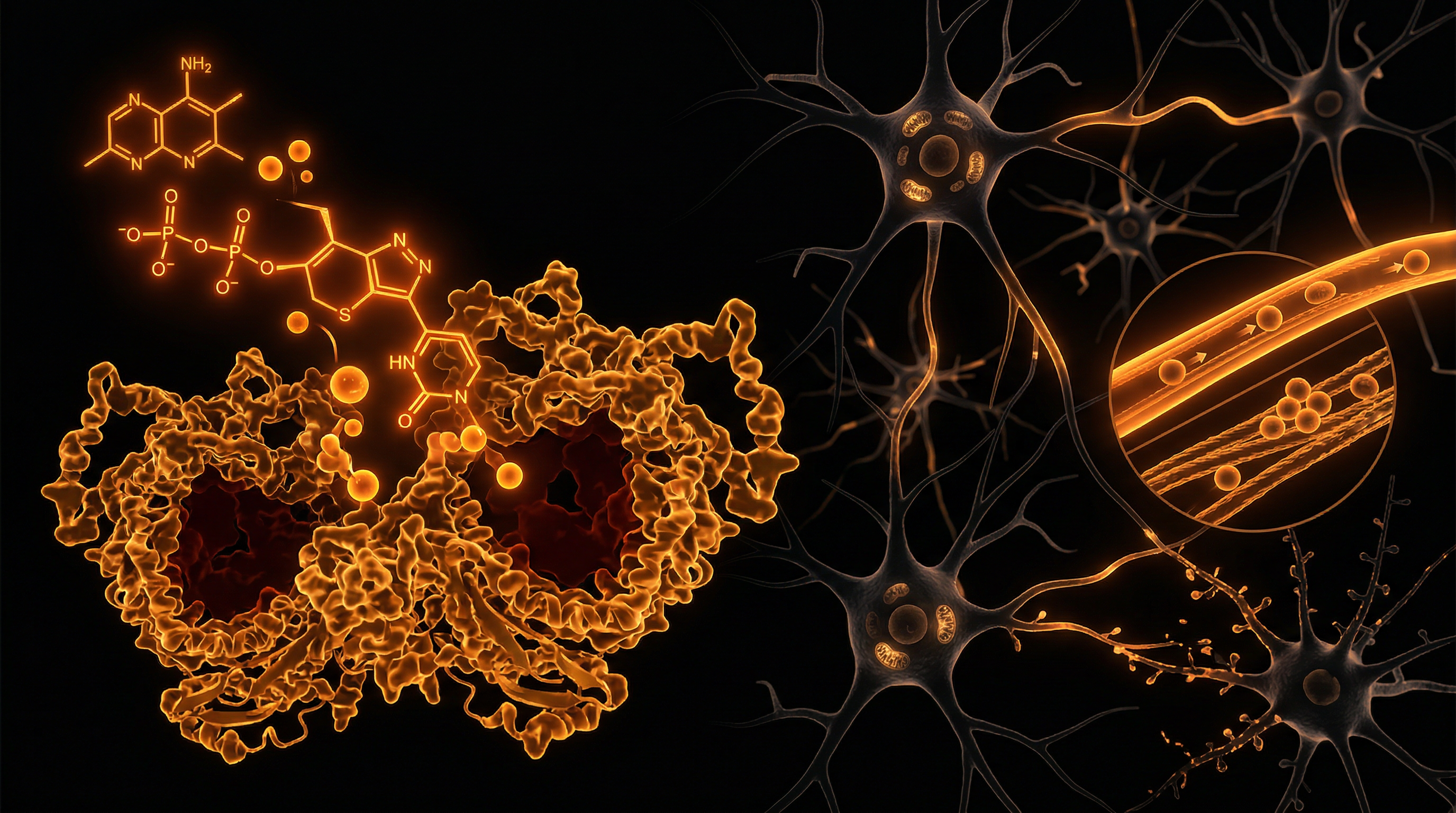
To understand the gravity of thiamine depletion, one must first grasp its role as the primary mediator of energy metabolism. Thiamine does not act on its own; it must be converted into its active form, Thiamine Pyrophosphate (TPP), also known as Thiamine Diphosphate (ThDP).
The Master Cofactor
TPP serves as a mandatory cofactor for several critical enzyme complexes that sit at the intersection of macronutrient metabolism. Without sufficient TPP, the body cannot effectively process glucose or certain amino acids. The most notable of these is the Pyruvate Dehydrogenase Complex (PDHC).
- —The Gateway: PDHC is the enzyme that converts pyruvate (the end product of glycolysis) into Acetyl-CoA. Acetyl-CoA is the "ticket" required to enter the Krebs Cycle (Citric Acid Cycle).
- —The Bottleneck: When thiamine is deficient, this conversion cannot occur. Pyruvate begins to back up in the system.
- —The Divergence: Instead of entering the aerobic pathway to produce 36-38 ATP, the body is forced into anaerobic metabolism, converting pyruvate into Lactic Acid.
Fact: The brain represents only 2% of body weight but consumes roughly 20% of the body’s total glucose. Because the brain is almost entirely dependent on aerobic glucose metabolism, it is the first organ to suffer when thiamine-dependent pathways fail.
The Pentose Phosphate Pathway
Thiamine is also a cofactor for transketolase, a key enzyme in the Pentose Phosphate Pathway. This pathway is responsible for generating NADPH, which is essential for fatty acid synthesis and the maintenance of the body’s master antioxidant, Glutathione. Furthermore, this pathway produces ribose-5-phosphate, a precursor for DNA and RNA synthesis. Consequently, thiamine depletion doesn't just stop energy production; it halts cellular repair and leaves the body vulnerable to oxidative stress.
Mechanisms at the Cellular Level
At the microscopic level, thiamine deficiency initiates a process known as mitochondrial transition. When the mitochondria can no longer produce energy via oxidative phosphorylation, the cell enters a state of crisis.
The Citric Acid Cycle Disruption
Within the Citric Acid Cycle, thiamine is required for the Alpha-Ketoglutarate Dehydrogenase complex. This step is a rate-limiting part of the cycle. When this enzyme fails:
- —ATP Production Plummets: The cell cannot maintain its electrochemical gradients.
- —Glutamate Excitotoxicity: Alpha-ketoglutarate is a precursor to glutamate. When the cycle stalls, glutamate (an excitatory neurotransmitter) can accumulate to toxic levels in the synaptic cleft, leading to neuronal death.
- —GABA Depletion: Since glutamate is the precursor to GABA (the primary inhibitory, "calming" neurotransmitter), thiamine deficiency often manifests as acute anxiety, restlessness, and insomnia.
The Blood-Brain Barrier and Oxidative Stress
The brain possesses specific transporters for thiamine (THTR-1 and THTR-2). However, these transporters are highly sensitive to environmental toxins and pH changes. When energy failure occurs, the Blood-Brain Barrier (BBB) begins to leak. This allow substances that are normally excluded from the brain to enter, further exacerbating neuroinflammation.
Statistical Insight: Studies have shown that even a 20% reduction in thiamine activity can lead to a measurable increase in reactive oxygen species (ROS) within hippocampal neurons, the area of the brain responsible for memory and spatial navigation.
Environmental Threats and Biological Disruptors
The United Kingdom presents a unique "perfect storm" for thiamine depletion. The confluence of cultural habits and industrial food production has created a landscape where thiamine is consistently "stolen" from the population.
Alcohol: The Great Depleter
In the UK, alcohol consumption is a cornerstone of social interaction. Alcohol is perhaps the most well-known "thiamine antagonist."
- —Absorption Inhibition: Alcohol directly inhibits the expression of THTR-1 and THTR-2 in the intestinal tract, meaning even if you eat thiamine-rich foods, you cannot absorb them.
- —Storage Failure: Alcohol interferes with the liver's ability to store thiamine and convert it into its active TPP form.
- —Increased Excretion: Alcohol acts as a diuretic, flushing water-soluble B-vitamins out through the kidneys at an accelerated rate.
Coffee and Tea: The Tannin Trap
The British obsession with tea and the burgeoning coffee shop culture add another layer of risk. Both coffee and tea contain antithiamine factors (ATFs), such as tannins and chlorogenic acids.
- —These compounds react with thiamine in the digestive tract, converting it into a biologically inactive form.
- —Thiaminases: Certain plants and raw fish contain enzymes called thiaminases that physically break the thiamine molecule apart. While less common in the UK diet than tannins, the sheer volume of coffee consumed (often 3-5 cups a day for the average professional) creates a continuous neutralizing effect on dietary B1.
Refined Sugar and Flour: The Metabolic Debt
The UK diet is heavily reliant on "white" carbohydrates—bread, pasta, biscuits, and sugary snacks. These are known as empty calories, but a more accurate term would be debt calories.
- —To metabolize one molecule of glucose, the body *requires* thiamine.
- —Refined sugar contains zero thiamine. Therefore, every time a person consumes a sugary soft drink or a pastry, they must "borrow" thiamine from their internal stores (liver, heart, and brain) to process that sugar.
- —Over time, this leads to High-Calorie Malnutrition, where the individual is overweight but functionally starving at a cellular level.
The Cascade: From Exposure to Disease
The progression of thiamine deficiency is often subtle, masquerading as other conditions until it reaches a critical threshold. In the medical literature, this is often described as a continuum.
Stage 1: The Subclinical "Malaise"
The initial signs are often dismissed by GP surgeries as "stress" or "general fatigue."
- —Irritability and "Air Hunger": A feeling of not being able to take a deep enough breath (dyspnea), caused by early disruption of the brainstem's respiratory centres.
- —Gastrointestinal Issues: Gastroparesis (slow stomach emptying) and low stomach acid. Thiamine is required for the vagus nerve to signal the digestive system.
- —Postural Orthostatic Tachycardia Syndrome (POTS): Dizziness upon standing, as the autonomic nervous system loses the energy required to regulate blood pressure.
Stage 2: Autonomic Dysfunction (Dysautonomia)
As depletion worsens, the Autonomic Nervous System (ANS) begins to fail. The ANS controls everything that happens automatically: heart rate, digestion, temperature regulation, and pupil dilation.
- —British "Stiff Upper Lip" Syndrome: Many people push through Stage 2 using more coffee and sugar, which further accelerates the depletion, leading to a "crash and burn" cycle.
- —Lactic Acidosis: Muscle pain, unexplained soreness, and a "heavy" feeling in the limbs as the body shifts to anaerobic metabolism.
Stage 3: Wernicke’s Encephalopathy and Beyond
While the mainstream view suggests this only happens to "hardcore alcoholics," subclinical Wernicke’s is increasingly found in the general population.
- —Symptoms: Ataxia (unsteady gait), ophthalmoplegia (eye movement issues), and mental confusion.
- —Korsakoff Psychosis: Permanent brain damage characterized by an inability to form new memories and "confabulation" (making up stories to fill memory gaps).
Important Fact: Many cases of "Fibromyalgia" and "Chronic Fatigue Syndrome" (ME/CFS) have been shown in clinical trials to respond dramatically to high-dose thiamine therapy, suggesting that thiamine depletion is a primary driver of these labels.
What the Mainstream Narrative Omits
The current medical consensus regarding thiamine in the UK is dangerously outdated. There are three primary "blind spots" in the mainstream narrative:
1. The Failure of the RDA
The Recommended Dietary Allowance (RDA) for thiamine (approx. 1.1mg to 1.2mg) was established to prevent the total collapse of the system (Beriberi). It was *not* designed for optimal neurological health in an environment saturated with thiamine-depleting stimulants. The RDA assumes a "clean" metabolism, not one burdened by alcohol, caffeine, and environmental toxins.
2. The Myth of the "Balanced Diet"
Doctors often tell patients that "you get all the B-vitamins you need from a balanced diet." This ignores the fact that bioavailability is not 100%. Furthermore, it ignores the existence of thiamine antagonists. You can eat a "balanced diet," but if you wash it down with a double espresso and a glass of wine, the net thiamine absorption may be near zero.
3. Inaccurate Testing
The standard blood test for thiamine is the Serum Thiamine test. This is almost useless. Less than 1% of the body’s thiamine is found in the serum; the rest is inside the cells. A person can have "normal" serum levels while their intracellular stores are dangerously depleted.
- —The Gold Standard: The Erythrocyte Transketolase Activation Coefficient (ETKA) test is the only way to accurately measure functional thiamine status, yet it is rarely, if ever, performed in an NHS setting.
The UK Context
The UK presents a specific sociological landscape that exacerbates this issue.
The "High Street" Coffee Culture
Over the last two decades, the UK has seen an explosion of coffee culture. High streets that once held diverse shops are now dominated by chains. This constant availability of caffeine, often consumed in large "venti" sizes, means the average Briton is subjected to a constant stream of chlorogenic acids that neutralise thiamine.
The Ultra-Processed Food (UPF) Crisis
According to recent data, the UK consumes more ultra-processed food than any other country in Europe (over 50% of the average diet). These foods are stripped of natural B-vitamins during processing. While some flour is "fortified," the form of thiamine used (Thiamine Mononitrate) is synthetic and often poorly absorbed compared to the natural forms found in whole foods like pork, legumes, and seeds.
The NHS Burden
The "mystery illness" epidemic—comprising Fibromyalgia, POTS, Long-Covid, and Type 2 Diabetes—is crippling the NHS. There is a profound refusal to look at the bioenergetic root of these conditions. Instead, the system focuses on "managing symptoms" with pharmaceutical drugs (like SSRIs or beta-blockers), many of which (such as certain antibiotics and diuretics) *further* deplete thiamine.
Protective Measures and Recovery Protocols
Recovering from thiamine depletion requires more than just "eating better." When the transporters are downregulated and the enzymes are dormant, a high-dose intervention is often necessary to "force" the enzymes back into action.
1. High-Bioavailability Derivatives
Standard Thiamine Hydrochloride (the kind found in cheap supplements) has very poor absorption in high doses. For neurological recovery, specialised forms are required:
- —Benfotiamine: A fat-soluble derivative that reaches much higher levels in the blood and is excellent for treating peripheral neuropathy and diabetic complications.
- —TTFD (Thiamine Tetrahydrofurfuryl Disulfide): A disulfide form that can cross the Blood-Brain Barrier without relying on the compromised thiamine transporters. This is the "gold standard" for neurological energy failure.
2. The Magnesium Connection
Important: Thiamine cannot be converted into its active TPP form without Magnesium.
- —Taking high-dose thiamine without magnesium can actually make symptoms worse, as the body tries to "start the engine" without the necessary oil, leading to further depletion of magnesium stores.
- —In the UK, magnesium deficiency is equally rampant due to soil depletion. Any thiamine protocol must include magnesium (glycinate or malate are preferred).
3. Eliminating Antagonists
Recovery is impossible if the "theft" continues.
- —Timing: If you must drink coffee or tea, do so at least 2 hours away from meals or supplements.
- —Sugar Cessation: Reducing refined sugar intake is the fastest way to stop the "drain" on your B1 reserves.
- —Alcohol Abstinence: During a recovery phase (typically 3-6 months), alcohol should be eliminated to allow the intestinal transporters to recover.
4. Dietary Sources
Once the system is stabilized, focus on thiamine-dense whole foods:
- —Pork (Organic/Pastured): The richest common source of B1.
- —Sunflower Seeds and Macadamia Nuts.
- —Nutritional Yeast: A potent natural source of the entire B-complex.
- —Legumes: Black beans and lentils (must be properly soaked to reduce anti-nutrients).
Summary: Key Takeaways
The evidence is clear: the modern UK lifestyle is a biological minefield for thiamine. The "spark plug" of our metabolism is being systematically extinguished by the very substances we use to cope with the demands of modern life.
- —Thiamine (B1) is the essential gatekeeper of the Citric Acid Cycle; without it, cellular energy production fails, and lactic acid rises.
- —Stimulants like alcohol, coffee, and refined sugar are not "neutral" habits; they are active thiamine antagonists that deplete our neurological reserves.
- —Neurological Energy Failure manifests as "mystery" symptoms: brain fog, anxiety, POTS, and chronic fatigue, which are frequently misdiagnosed by mainstream medicine.
- —The RDA is insufficient for the modern context. We require significantly more thiamine to offset the environmental and dietary "tax" placed upon us.
- —Recovery requires strategy: Utilising high-bioavailability forms like TTFD and ensuring adequate Magnesium intake is crucial for restarting the mitochondrial engine.
We must stop viewing vitamins as "optional extras" and start seeing them as the literal fuel for our consciousness. In the UK, the battle for health is increasingly a battle for our biochemistry. Restoring thiamine is not merely a nutritional choice; it is an act of metabolic rebellion against a system that profits from our collective exhaustion.
This article is provided for informational and educational purposes only. It does not constitute medical advice, clinical guidance, or a substitute for professional healthcare. Information reflects cited research at time of publication. Always consult a qualified healthcare professional before acting on any health information.
RESEARCH FOUNDATIONS
Biological Credibility Archive
Psychostimulant-induced hypermetabolism significantly increases the rate of thiamine pyrophosphate utilization within the prefrontal cortex.
Marginal thiamine status is a critical risk factor for the development of Wernicke-Korsakoff-like symptoms in frequent users of synthetic stimulants.
Thiamine acts as a necessary cofactor for oxidative phosphorylation, and its depletion leads to mitochondrial dysfunction under conditions of sustained catecholamine release.
Modern dietary patterns in Western Europe often provide insufficient thiamine to meet the increased metabolic demands imposed by stimulant use.
Neuronal damage caused by excessive stimulant intake is exacerbated by the reduction of thiamine-dependent enzyme activity in the basal ganglia.
Citations provided for educational reference. Verify via PubMed or institutional databases.
Medical Disclaimer
The information in this article is for educational purposes only and does not constitute medical advice, diagnosis, or treatment. Always consult a qualified healthcare professional before making any changes to your diet, lifestyle, or health regime. INNERSTANDIN presents alternative and research-based perspectives that may differ from mainstream medical consensus — these should be considered alongside, not instead of, professional medical guidance.
Read Full DisclaimerReady to learn more?
Continue your journey through our classified biological research.
DISCUSSION ROOM
Members of THE COLLECTIVE discussing "Thiamine Depletion via Modern UK Stimulants"
SILENT CHANNEL
Be the first to discuss this article. Your insight could help others understand these biological concepts deeper.
THE ARSENAL
Based on Nutritional Deficiencies — products curated by our research team for educational relevance and biological support.

Magnesium L-Threonate
Magnesium Blend – The Most Important Mineral

Energy Blend Supports
INNERSTANDING may earn a commission on purchases made through these links. All products are selected based on rigorous educational relevance to our biological research.
RABBIT HOLE
Follow the biological thread deeper