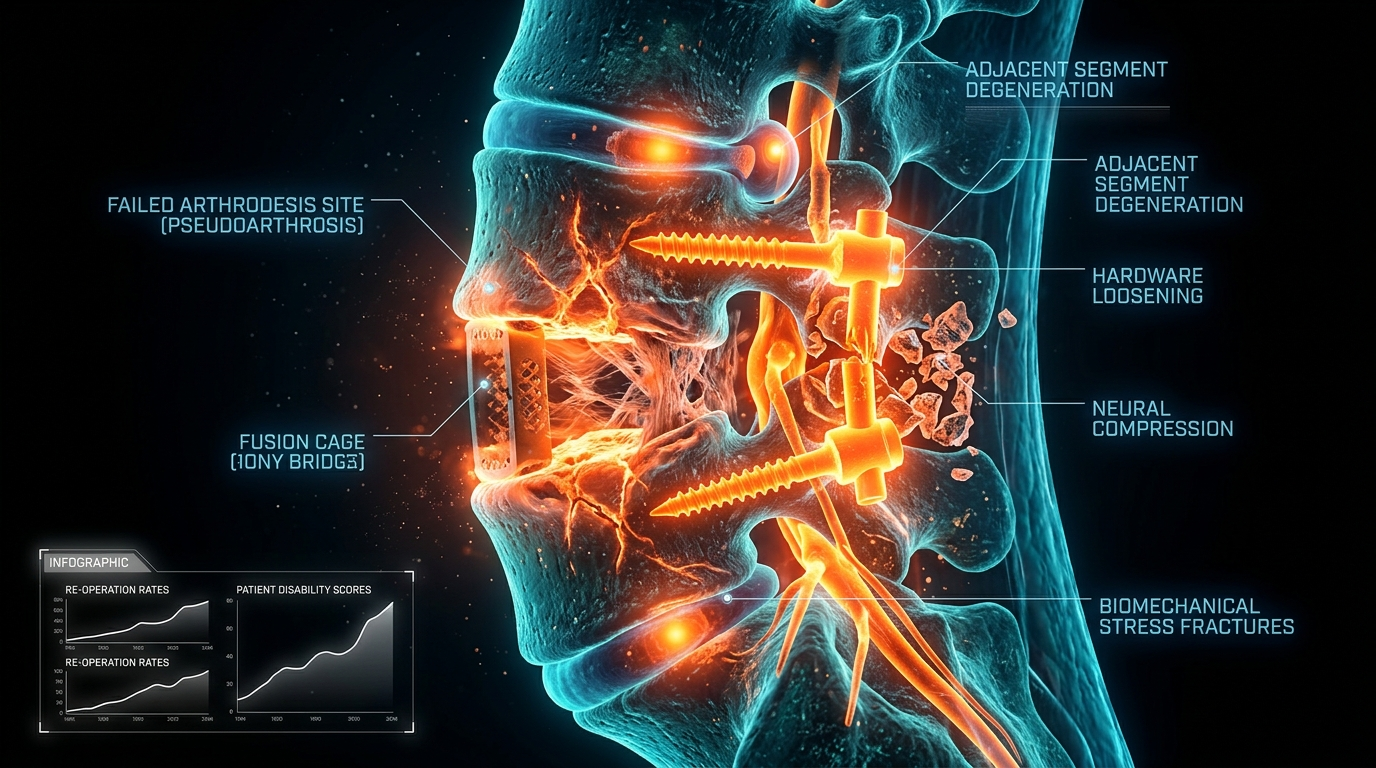
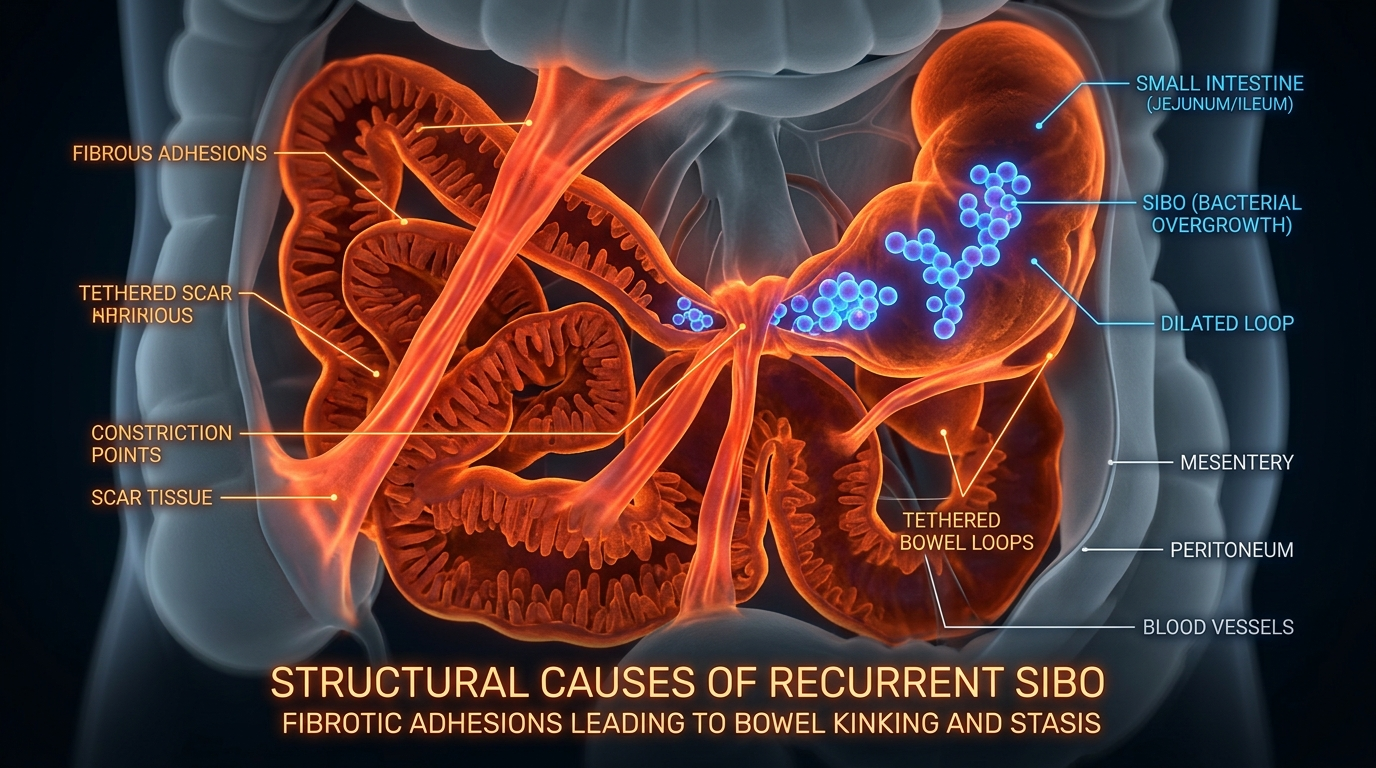
Adhesions and Scar Tissue: The Structural Causes of Recurrent SIBO
Abdominal surgeries or endometriosis can create internal adhesions that physically kink the small intestine. These structural impediments create 'blind loops' where bacteria can multiply undisturbed by normal motility.
Overview
The prevailing narrative surrounding Small Intestinal Bacterial Overgrowth (SIBO) remains stubbornly focused on the microbial population itself. Patients are conditioned to view their condition through the lens of 'infection'—a rogue colony of bacteria that simply needs to be eradicated with a sufficiently potent course of Rifaximin or herbal antimicrobials. However, for a significant cohort of chronic sufferers, this approach is akin to painting over damp. The rot is not in the paint; it is in the structure of the building. In the world of clinical gastroenterology and visceral biology, we are increasingly recognising that recurrent SIBO is often a mechanical failure rather than a biological one.
Adhesions and scar tissue represent the 'invisible' culprits of the SIBO epidemic. These internal bands of fibrous tissue, which form as a natural but often overzealous part of the body's healing process, act as physical constraints within the abdominal cavity. Imagine the small intestine as a highly sophisticated, six-metre-long flexible hose. For optimal function, this hose must remain free to move, glide, and pulse. Adhesions are the equivalent of tying knots in that hose or pinning it to the floorboards.
When the small intestine is physically tethered or kinked by scar tissue, the result is a catastrophic disruption of motility. This leads to the formation of 'blind loops'—anatomical pockets or segments where the normal 'sweeping' action of the gut, known as the Migrating Motor Complex (MMC), cannot reach. In these stagnant zones, bacteria do not merely survive; they thrive, fermenting food particles and producing the gases (hydrogen, methane, and hydrogen sulfide) that define the SIBO experience. Without addressing these structural impediments, any attempt to 'kill' the bacteria is doomed to fail, as the environment remains perfectly primed for immediate recolonisation. This article serves as an authoritative exploration into the structural genesis of SIBO, exposing the cellular mechanisms of adhesion formation and the systemic failure of modern medicine to address the physical architecture of the gut.
##
The Biology — How It Works
To understand why adhesions are so destructive, one must first appreciate the delicate choreography of the small intestine. Unlike the large intestine, which is largely fixed in place, the small intestine is suspended by a double-layered fold of peritoneum called the mesentery. This allows the small intestine a remarkable degree of mobility, which is essential for its primary functions: digestion, nutrient absorption, and, crucially, self-cleaning.
The Migrating Motor Complex (MMC)
The MMC is the 'housekeeper' of the small intestine. It is a distinct electrical and mechanical pattern of activity that occurs during fasting. Every 90 to 120 minutes, a wave of intense contraction sweeps from the stomach through to the end of the ileum. This process is designed to clear out undigested food, cellular debris, and, most importantly, excess bacteria, pushing them into the colon where they belong.
According to clinical data, a dysfunctional MMC is the single greatest risk factor for the development of SIBO. In patients with structural adhesions, the MMC is physically blocked. The wave of contraction hits a 'kink' or a tethered segment of the bowel and loses its kinetic energy, leaving the segment distal to the adhesion effectively 'un-swept'.
The Mechanics of the 'Blind Loop'
When an adhesion pulls a loop of the small intestine into an acute angle—a phenomenon often called 'kinking'—it creates what is known in surgical literature as a Blind Loop. This is not necessarily a complete obstruction (which would be a surgical emergency), but a functional bypass. The flow of chyme (liquidated food) slows down or becomes turbulent at the site of the kink.
This stasis creates a micro-environment where the pH shifts and the oxygen concentration drops, favouring the overgrowth of anaerobic and facultative anaerobic bacteria. These bacteria, such as *E. coli* and *Klebsiella*, begin to deconjugate bile acids. This is a critical biological failure: deconjugated bile acids are toxic to the intestinal lining and cannot effectively emulsify fats. Consequently, the patient suffers from malabsorption, fat-soluble vitamin deficiencies (A, D, E, K), and chronic inflammation, all because a physical band of tissue is preventing the gut from moving.
##
Mechanisms at the Cellular Level
The formation of an adhesion is a complex, multi-stage biochemical cascade that occurs within the peritoneal cavity. To understand why some people develop life-altering adhesions while others heal cleanly, we must look at the microscopic level of fibrinogenesis.
The Peritoneal Response to Insult
The peritoneum is a serous membrane lined with a single layer of mesothelial cells. Under normal conditions, these cells produce a lubricating fluid that allows the intestines to glide over one another with zero friction. However, when the peritoneum is damaged—whether by the scalpel of a surgeon, the inflammatory lesions of endometriosis, or a traumatic blow—the body initiates an immediate emergency repair protocol.
- —Exudation and Fibrin Formation: Within seconds of injury, the permeability of local blood vessels increases. A protein-rich exudate, containing fibrinogen, leaks into the peritoneal cavity.
- —The Fibrin Matrix: Fibrinogen is converted into fibrin, which acts as a 'biological glue'. In a healthy scenario, this fibrin is temporary. It creates a 'bridge' between tissues to stabilise the area during initial healing.
- —The Fibrinolytic System: Normally, the body releases Tissue Plasminogen Activator (tPA), an enzyme that dissolves the fibrin glue once the underlying tissue has begun to repair.
When Healing Becomes Pathology
The transition from a temporary fibrin bridge to a permanent adhesion occurs when there is an imbalance between fibrin formation and fibrinolysis. If the inflammatory insult is too great, or if the patient’s systemic fibrinolytic capacity is low, the fibrin bridge is not dissolved.
Instead, it acts as a scaffold for fibroblasts. These cells migrate into the fibrin matrix and begin depositing Type I and Type III collagen. They are often accompanied by the growth of new blood vessels (angiogenesis) and, crucially, new nerve fibres. This turns a simple 'sticky spot' into a permanent, vascularised, and often painful band of dense connective tissue.
The Role of TGF-β
At the heart of this process is Transforming Growth Factor-beta (TGF-β), a potent pro-fibrotic cytokine. In the presence of chronic inflammation—such as that found in untreated endometriosis or repeated abdominal infections—TGF-β remains elevated. This keeps the fibroblasts in a state of hyper-activity, continually thickening and tightening the scar tissue. This 'remodelling' can continue for years, meaning an adhesion formed during an appendectomy at age ten can slowly tighten until it causes SIBO at age thirty.
##
Environmental Threats and Biological Disruptors
While surgery is the primary driver of adhesions, it is not the only factor. Our modern environment provides a plethora of 'biological disruptors' that tilt the body's healing response toward excessive scarring.
Iatrogenic Insult: The Paradox of Surgery
It is a bitter irony that the very interventions meant to save us are often the catalysts for chronic illness. Post-operative adhesions occur in up to 93% of patients undergoing abdominal or pelvic surgery. Even laparoscopic ('keyhole') surgery, while less invasive, involves the insufflation of the abdomen with carbon dioxide. This gas can dry out the peritoneal lining, causing widespread micro-trauma and subsequent 'filmy' adhesions throughout the cavity.
Endometriosis: The Internal Scar-Maker
For women, endometriosis is a primary structural cause of SIBO that is frequently overlooked. Endometrial-like tissue growing outside the uterus undergoes the same monthly cycle of bleeding and shedding. However, this blood has no exit path. It stays within the pelvic cavity, causing intense localised inflammation. This inflammation is a massive driver of adhesion formation, often 'gluing' the small intestine to the uterus, bladder, or pelvic wall.
Statistics from UK-based endometriosis charities indicate that it takes an average of 7.5 years to receive a diagnosis. For many women, this represents nearly a decade of unmanaged internal scarring, making structural SIBO an almost inevitable consequence.
Chronic Inflammatory States
A diet high in ultra-processed foods, refined sugars, and industrial seed oils keeps the body in a state of low-grade systemic inflammation. This environment is highly conducive to fibrosis. When the body is already 'primed' for inflammation, any minor intestinal insult—even a bout of severe food poisoning (post-infectious IBS)—can trigger a more aggressive fibrin response than it would in a metabolically healthy individual.
##
The Cascade: From Exposure to Disease
The progression from a structural insult to a full-blown case of SIBO follows a predictable, yet devastating, cascade. It is rarely a sudden onset; rather, it is a slow erosion of GI function.
Step 1: The Primary Insult
The journey begins with an event that damages the peritoneum: a C-section, an appendectomy, a bout of pelvic inflammatory disease (PID), or even a severe physical trauma (such as a car accident where the seatbelt causes internal shearing).
Step 2: The Silent Tightening
Over the following months and years, the fibrin bridges mature into collagenous adhesions. The patient feels nothing, or perhaps only a vague 'tugging' sensation when stretching. Internally, however, the small intestine is losing its ability to move freely. The 'gliding' motion required for peristalsis is compromised.
Step 3: Motility Failure and Stasis
As the adhesions tighten, they create physical 'bottlenecks'. The Migrating Motor Complex (MMC) can no longer clear the entire length of the small intestine. 'Islands' of stasis form. In these islands, the microbial environment shifts. The pH rises as stagnant chyme ferments, and the protective mucosal layer begins to thin.
Step 4: Bacterial Colonisation
Bacteria that usually reside in the colon (such as *Bacteroides* and *Firmicutes*) or even the oral cavity migrate upwards or proliferate in the stagnant segments of the small intestine. They find a feast of undigested carbohydrates and fibres that have become trapped in the 'blind loops'.
Step 5: Symptomatic SIBO and Systemic Toxicity
The bacteria produce gases that cause the characteristic bloating of SIBO. But the damage goes deeper. The metabolic byproducts of these bacteria—such as lipopolysaccharides (LPS)—begin to leak through the intestinal wall (Leaky Gut). This triggers a systemic immune response, leading to brain fog, chronic fatigue, and joint pain. The patient is now trapped in a cycle: the SIBO causes more inflammation, which potentially drives more adhesion growth, further worsening the structural problem.
##
What the Mainstream Narrative Omits
The standard medical approach to SIBO is fundamentally reductionist. It treats the human body as a chemical test tube rather than a dynamic, mechanical organism. There are three critical omissions in the mainstream narrative that prevent patients from achieving lasting recovery.
The Failure of the 'Kill Phase'
Most gastroenterologists rely solely on antibiotics. While Rifaximin is excellent at reducing the bacterial load, it does nothing to address the *reason* the bacteria were there in the first place. If a person has a structural 'kink' in their intestine, no amount of antibiotic will straighten it. This is why the 'relapse rate' for SIBO is so high—often reported at over 40% within three months of treatment.
The Ignored Role of Visceral Manipulation
Mainstream medicine has a blind spot regarding manual therapy. While a surgeon is trained to cut tissue, few are trained to understand the subtle 'motility' and 'mobility' of organs. There is a profound lack of referral to specialised visceral physical therapists who can manually break down adhesions without further surgery. The irony is that further surgery to 'clear' adhesions often causes even more adhesions to form—a phenomenon known as 'recurrent adhesive bowel obstruction'.
The Psychosomatic Dismissal
Because adhesions do not always show up on standard imaging (CT scans or MRIs are notoriously poor at detecting filmy or even dense adhesions), patients are often told their pain and bloating are 'functional' or 'psychosomatic'. This gaslighting occurs because the medical model prioritises what can be seen on a screen over the patient's surgical history and physical symptoms.
##
The UK Context
The situation for SIBO sufferers in the United Kingdom is particularly precarious, shaped by the unique constraints of the National Health Service (NHS) and a general lag in the adoption of functional GI protocols.
Recent data indicates that the NHS performs over 5 million abdominal and pelvic surgeries annually. Given the 90%+ rate of adhesion formation, the 'pool' of potential structural SIBO patients in the UK is staggering.
The NHS Diagnostic Gap
The NHS rarely tests for SIBO. When it does, it typically uses hydrogen breath tests which are often misinterpreted. More importantly, there is almost no provision within the NHS for the treatment of non-obstructive adhesions. Unless an adhesion is causing a total bowel blockage (a life-threatening emergency), it is generally ignored. This leaves thousands of Britons in a 'grey zone' of chronic ill-health, where they are too sick to function but not 'urgent' enough for surgical review.
The Private Sector and Specialised Care
In the UK, the most advanced work in structural SIBO is being done in the private sector, often by practitioners trained in the 'Wurn Technique' or other forms of Visceral Manipulation. However, these treatments are expensive and not widely available outside of London and major hubs. This creates a two-tier system where only those with significant financial resources can access the structural 'un-kinking' they need to truly resolve their SIBO.
The Endometriosis Crisis
With 1.5 million UK women living with endometriosis, the link between this condition and SIBO is a national health crisis. The current UK 'Gold Standard' for endometriosis is laparoscopic excision surgery. While superior to 'ablation' (burning the tissue), it still carries the risk of post-operative adhesions. UK patients are rarely warned that their endometriosis surgery might be the starting point for a decade of digestive misery.
##
Protective Measures and Recovery Protocols
If structural adhesions are the cause of your recurrent SIBO, the solution must be multi-dimensional. You cannot simply 'poison' your way out of a mechanical problem. A truly effective protocol must address the physical, biochemical, and lifestyle factors that govern scar tissue.
1. Manual Physical Therapy: Breaking the Bonds
The most direct way to address adhesions is through specialised manual therapy.
- —Visceral Manipulation: A gentle manual therapy that helps to restore the movement of the internal organs. Developed by French osteopath Jean-Pierre Barral, it focuses on the 'sliding' surfaces of the peritoneum.
- —The Clear Passage Approach: This is a non-surgical treatment (the Wurn Technique) that uses specific manual pressures to break down the cross-links in collagen fibres. Clinical studies have shown it to be effective in opening blocked Fallopian tubes and, crucially, resolving SIBO by restoring gut motility.
2. Systemic Enzyme Therapy (Fibrinolytics)
To support the body's internal 'clean-up' crew, one can utilise systemic enzymes. These are taken on an empty stomach so they can enter the bloodstream and act systemically rather than just digesting food.
- —Serrapeptase and Nattokinase: These enzymes have a high affinity for fibrin. They work to 'dissolve' the non-living fibrin tissue that forms the basis of adhesions.
- —Dosage and Timing: This must be a long-term strategy. It can take 6-12 months of consistent enzyme therapy to notice a shift in the density of internal scar tissue.
3. Prokinetic Support
If the gut is physically sluggish due to adhesions, we must chemically 'nudge' the MMC.
- —Pharmaceutical Prokinetics: Low-dose Erythromycin or Prucalopride (Resolor) can help stimulate the MMC.
- —Natural Prokinetics: Ginger root and 5-HTP (found in supplements like MotilPro) are effective for milder cases.
- —Meal Spacing: To allow the MMC to function, one must strictly adhere to at least 4-5 hours between meals and a 12-hour fast overnight. This is non-negotiable for structural SIBO patients.
4. Anti-Fibrotic Nutrition
Diet should be focused on lowering TGF-β and supporting healthy collagen turnover.
- —Avoid: Inflammatory seed oils (canola, sunflower), refined grains, and high-fructose corn syrup, all of which fuel the fibroblasts.
- —Include: High doses of Vitamin C (essential for healthy collagen remodelling), Bioflavonoids (to stabilise mast cells), and Omega-3 fatty acids (to lower systemic inflammation).
- —Hydration: Fascia and adhesions are highly sensitive to hydration. Dehydrated tissue is more rigid and 'sticky'. Proper mineralisation (electrolytes) is key.
5. Vagus Nerve Stimulation
The Vagus nerve is the 'off-switch' for inflammation in the gut and the 'on-switch' for motility. Adhesions create a 'stress state' in the body, which inhibits the Vagus nerve.
- —Techniques: Cold water immersion, deep diaphragmatic breathing, and even gargling can help tone the Vagus nerve, encouraging the nervous system to prioritise 'Rest and Digest' over 'Fight or Flight'.
##
Summary: Key Takeaways
The journey of the chronic SIBO patient is often one of frustration and cyclical failure. By understanding the role of adhesions and scar tissue, we shift the paradigm from 'infection' to 'architecture'.
- —Structure Dictates Function: You cannot have a healthy microbiome in a physically compromised intestine. Adhesions are the primary 'hidden' cause of motility failure.
- —The SIBO-Surgery Connection: Anyone with a history of abdominal surgery (C-section, appendectomy, gallbladder removal) or endometriosis should consider their SIBO to be structural until proven otherwise.
- —The Limitation of Antibiotics: Rifaximin is a tool for symptom management, not a cure for structural stasis. Relapse is inevitable if the physical 'kinks' remain.
- —Mechanics of Stasis: Adhesions create 'blind loops' where bacteria proliferate undisturbed by the housekeeping waves of the Migrating Motor Complex.
- —Cellular Healing: Adhesions are the result of an imbalance in fibrinolysis, driven by chronic inflammation and pro-fibrotic cytokines like TGF-β.
- —The UK Challenge: NHS protocols are currently ill-equipped to deal with the mechanical causes of SIBO, necessitating a proactive, often private, approach to recovery.
- —A Multi-Modal Solution: Lasting recovery requires a combination of manual visceral therapy, systemic enzymes to dissolve fibrin, and rigorous prokinetic support to keep the 'hose' flowing.
The path to 'Innerstanding' your gut health requires a deep respect for the physical reality of your body. Your intestines are not just a site for chemical reactions; they are a living, moving masterpiece of biological engineering. When that engineering is compromised by the 'invisible knots' of scar tissue, the solution must be as structural as the problem itself. It is time to stop fighting the bacteria and start freeing the gut.
This article is provided for informational and educational purposes only. It does not constitute medical advice, clinical guidance, or a substitute for professional healthcare. Information reflects cited research at time of publication. Always consult a qualified healthcare professional before acting on any health information.
RESEARCH FOUNDATIONS
Biological Credibility Archive
Citations provided for educational reference. Verify via PubMed or institutional databases.
Medical Disclaimer
The information in this article is for educational purposes only and does not constitute medical advice, diagnosis, or treatment. Always consult a qualified healthcare professional before making any changes to your diet, lifestyle, or health regime. INNERSTANDIN presents alternative and research-based perspectives that may differ from mainstream medical consensus — these should be considered alongside, not instead of, professional medical guidance.
Read Full DisclaimerReady to learn more?
Continue your journey through our classified biological research.
DISCUSSION ROOM
Members of THE COLLECTIVE discussing "Adhesions and Scar Tissue: The Structural Causes of Recurrent SIBO"
SILENT CHANNEL
Be the first to discuss this article. Your insight could help others understand these biological concepts deeper.
THE ARSENAL
Based on SIBO & Small Intestine Health — products curated by our research team for educational relevance and biological support.

Magnesium Blend – The Most Important Mineral

Clean Slate – Detoxes thousands of chemicals,heavy metals, pesticides, allergens, mold spores and fungus

Vegan Essential Amino Acids – Plant-Powered Protein Building
INNERSTANDING may earn a commission on purchases made through these links. All products are selected based on rigorous educational relevance to our biological research.
RABBIT HOLE
Follow the biological thread deeper