Spinal Arthrodesis Failures: The Biological Case Against Unnecessary Surgery
Rates of spinal fusion surgery continue to rise despite evidence showing high failure rates for non-specific back pain. We analyze why structural interventions often fail to resolve what is essentially a neurological signaling problem.
Overview
The modern medical landscape is currently grappling with what can only be described as a 'fusion epidemic'. Over the past two decades, the rate of spinal arthrodesis—commonly known as spinal fusion surgery—has skyrocketed, particularly in Western nations. In the United Kingdom and the United States, this procedure has transitioned from a last-resort intervention for unstable fractures or gross spinal deformities into a primary treatment for "non-specific" chronic low back pain. However, as biological researchers at INNERSTANDING, we must confront the uncomfortable reality: the clinical outcomes for these procedures are often dismal. We are witnessing a systemic failure to distinguish between a mechanical structural issue and a complex neurological signalling crisis.
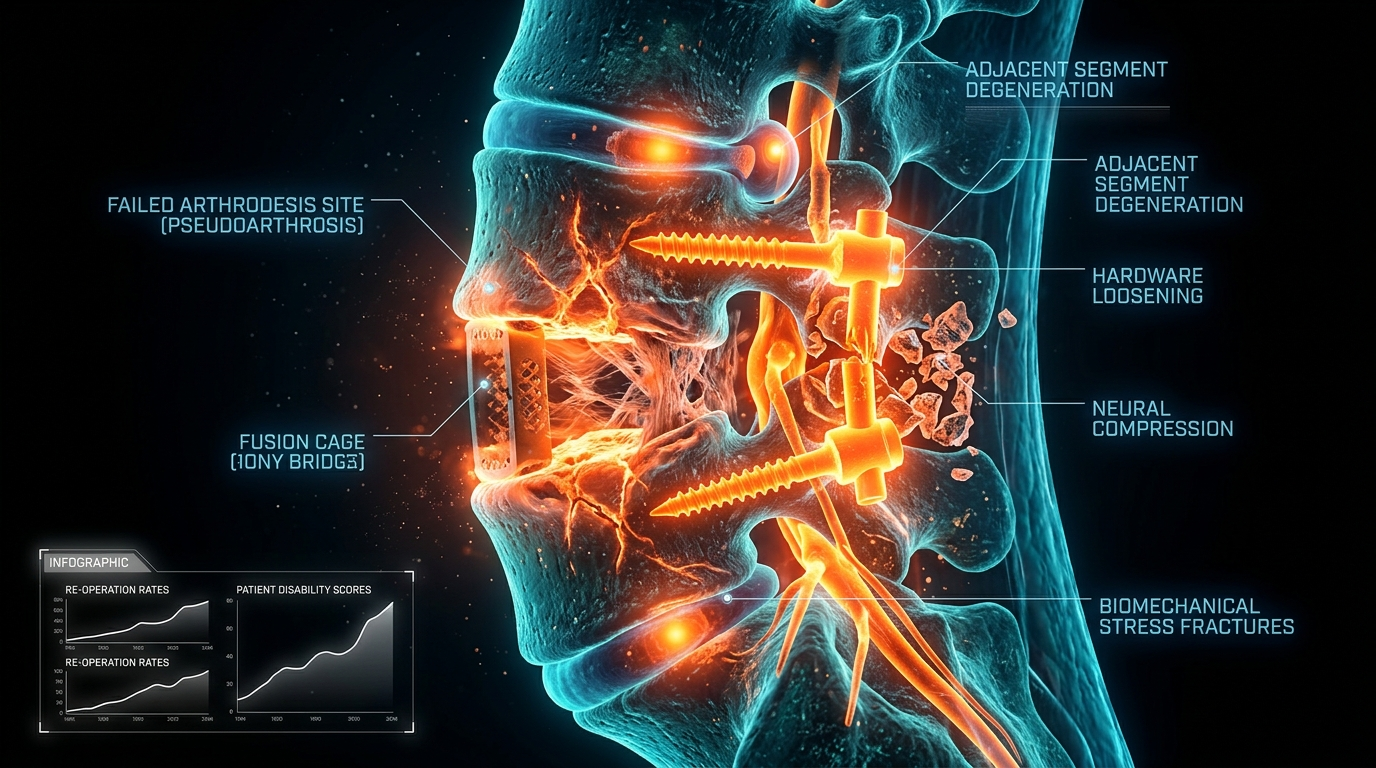
Spinal fusion involves the permanent joining of two or more vertebrae using bone grafts and hardware such as pedicle screws and rods. The underlying logic is deceptively simple: if movement causes pain, we must stop the movement. Yet, this Newtonian, biomechanical approach to a biological organism is fundamentally flawed. It treats the human spine like a series of inanimate struts and hinges rather than a living, sensing, and highly adaptive organ system. The biological cost of this misunderstanding is profound. When we fuse a segment of the spine, we do not merely "stabilise" it; we irreversibly alter the loading mechanics of the entire kinetic chain, trigger a cascade of inflammatory cytokines, and often leave the patient with a permanent neurological "alarm" that no amount of titanium can silence.
The disconnect between radiological findings and clinical symptoms is perhaps the most significant oversight in modern orthopaedics. Magnetic Resonance Imaging (MRI) frequently reveals "degenerative changes" in individuals who are completely asymptomatic. Conversely, patients with debilitating pain often present with relatively "clean" scans. By pursuing surgery based on a photograph of a structure—an image that often shows the normal, age-related "wrinkles" of the internal body—the medical-industrial complex is performing high-stakes structural interventions on what is essentially a software problem. This article will dissect the biological, cellular, and neurological reasons why spinal fusion is failing patients and why the case against unnecessary surgery is becoming irrefutable.
##
The Biology — How It Works
To understand why spinal arthrodesis fails, we must first understand the biological requirements for a successful fusion and how the body responds to the presence of foreign hardware. The process of arthrodesis is a race between two competing forces: osteogenesis (the formation of new bone) and mechanical failure. For a fusion to "take," the body must be in a physiological state that allows for the massive mobilisation of osteoblasts—the cells responsible for bone synthesis. This is not a passive process; it is a metabolic marathon that requires an ideal systemic environment.
The Biomechanical Paradox
The human spine is designed for segmental motion. Each intervertebral disc and facet joint pair acts as a shock absorber and a pivot point. When a segment is fused, that motion does not simply disappear; it is redistributed. This leads to what is known in the literature as Adjacent Segment Disease (ASD). The levels immediately above and below the fusion site are suddenly subjected to an exponential increase in torque and shear forces. From a biological standpoint, the cells within the adjacent discs—the chondrocytes—cannot keep pace with this sudden mechanical overload. They begin to express matrix metalloproteinases (MMPs), which degrade the collagenous structure of the disc, leading to rapid "wear and tear" that necessitates further surgery within five to ten years.
The Role of Bone Morphogenetic Proteins (BMPs)
In an attempt to guarantee fusion success, surgeons often use recombinant human bone morphogenetic protein-2 (rhBMP-2). While this protein is a potent stimulator of bone growth, its biological "dark side" is frequently overlooked in clinical summaries. BMPs are highly inflammatory. Their introduction into the spinal environment can lead to significant soft tissue swelling, seroma formation, and, most alarmingly, the unintended stimulation of neural growth or bone formation within the spinal canal (ectopic bone). The biological reality is that we are using a sledgehammer to crack a nut, often triggering a pro-inflammatory state that prevents the very healing the patient seeks.
The Hardware Interference
The introduction of titanium or PEEK (Polyetheretherketone) cages and pedicle screws creates a permanent foreign body response. While these materials are biocompatible, they are not biologically inert. They disrupt the local electrical environment of the bone—the piezoelectric effect—which is crucial for healthy bone remodelling. Furthermore, the presence of metal can lead to the release of micro-particles through a process known as fretting corrosion. These particles are engulfed by macrophages, which then release a slew of pro-inflammatory cytokines like TNF-alpha and IL-6, contributing to a state of chronic local inflammation that can irritate adjacent nerve roots and perpetuate the pain cycle.
##
Mechanisms at the Cellular Level
At the heart of the failure of spinal fusion lies the misunderstanding of nociception versus pain. Pain is a conscious experience produced by the brain; nociception is the cellular detection of potentially tissue-damaging stimuli. In chronic back pain, the cellular mechanisms have often shifted into a state of permanent "high alert," a phenomenon known as central sensitisation.
Glial Cell Activation and Neuroinflammation
Within the spinal cord's dorsal horn, glial cells (the immune cells of the central nervous system) play a pivotal role in pain processing. When the spine is subjected to the massive trauma of surgery—cutting through muscle, retracting nerve roots, and drilling into bone—these glial cells transition from a "resting" to an "activated" state. Once activated, they release neuroexcitatory substances such as glutamate and pro-inflammatory cytokines. This creates a "smog" of inflammation that lowers the threshold for pain signals. In this hyper-excitable state, even normal movements or light pressure are interpreted by the brain as intense pain. The surgery, intended to fix a mechanical problem, essentially "pours petrol" on the neurological fire of glial activation.
The Annulus Fibrosus and Nerve Ingrowth
A healthy intervertebral disc is largely aneural (lacking nerves), except for the outer third of the annulus fibrosus. However, in a "degenerative" disc, there is often a pathological ingrowth of nerve fibres and blood vessels into the deeper layers of the disc, sometimes reaching all the way into the nucleus pulposus. These new nerve fibres are often nociceptive (pain-sensing) and are highly sensitised by the acidic environment of a decaying disc. Fusion surgery attempts to stop the movement of these fibres, but it does nothing to address the chemical milieu that is stimulating them. If the inflammatory "soup" remains, the pain persists, regardless of whether the bone has successfully fused.
The Ischaemic Factor
Cells require oxygen and nutrients to thrive and repair. The microvasculature of the spine is delicate. Chronic inflammation and surgical scarring (fibrosis) lead to a state of localised ischaemia (reduced blood flow). When cells are deprived of oxygen, they switch to anaerobic metabolism, producing lactic acid. This drop in pH directly activates acid-sensing ion channels (ASICs) on nociceptors, creating a self-perpetuating cycle of pain. A fused segment, surrounded by scar tissue and metallic hardware, is often a desert of poor circulation, making it biologically impossible for the tissue to return to a "pain-free" state.
##
Environmental Threats and Biological Disruptors
The success or failure of spinal surgery is not solely determined in the operating theatre; it is heavily influenced by the patient's internal biological environment. Modern life is replete with "biological disruptors" that undermine the integrity of connective tissue and the efficacy of the immune system.
The Impact of Glycation and Metabolic Health
Patients with insulin resistance or Type 2 diabetes are at a significantly higher risk of fusion failure. High levels of circulating glucose lead to the formation of Advanced Glycation End-products (AGEs). These molecules create "cross-links" in the collagen of the discs and bones, making them brittle and less resilient. AGEs also bind to their receptors (RAGE), triggering a systemic inflammatory response. If a patient is in a pro-inflammatory metabolic state, the body is more likely to view the surgical site as a site of perpetual injury rather than a site of repair.
In the UK, it is estimated that nearly 1 in 3 adults has some form of metabolic syndrome, a condition that fundamentally impairs the body's ability to recover from major spinal interventions.
The Smoking and Vasoconstriction Link
It is well-documented in surgical literature that smokers have significantly lower fusion rates. The biology behind this is clear: nicotine is a potent vasoconstrictor. It reduces the blood flow to the vertebral endplates, which are the primary source of nutrition for the discs and the "soil" for the bone graft. Smoking also inhibits osteoblast activity and increases the production of carbon monoxide, further depriving the healing bone of oxygen. However, the mainstream narrative often fails to emphasise that "passive" environmental toxins and poor air quality can exert similar, albeit less intense, pressures on the spinal microenvironment.
Cortisol and the Stress Response
The endocrine system plays a massive role in tissue healing. Chronic psychological stress leads to the dysregulation of the HPA (hypothalamic-pituitary-adrenal) axis, resulting in chronically elevated cortisol. While cortisol is an anti-inflammatory in the short term, chronic elevation leads to "glucocorticoid resistance," where cells no longer respond to the anti-inflammatory signal. High cortisol also inhibits bone formation and stimulates bone resorption. A patient undergoing surgery while in a state of high chronic stress is biologically predisposed to "non-union"—the failure of the bones to fuse—and the development of Failed Back Surgery Syndrome (FBSS).
##
The Cascade: From Exposure to Disease
The journey to an "unnecessary" spinal fusion rarely starts with a catastrophic event. Instead, it is usually a slow cascade of biological failures, often exacerbated by the medical system itself.
The Iatrogenic Descent
The cascade begins with an episode of acute back pain—a common human experience. The biological response should be one of protection, rest, and then gradual movement. However, the mainstream medical approach often involves early imaging (MRI). Once a "bulge" or "degeneration" is identified, the patient is given a structural label. This label acts as a psychological "nocebo," inducing fear and guarded movement.
Guarding and Muscle Atrophy
Fear-avoidance behaviour leads to the "guarding" of the paraspinal muscles, particularly the multifidus. These muscles are crucial for spinal stability. When they are not used, they undergo rapid fatty infiltration. The muscle fibres are replaced by fat, a process that is often irreversible. This loss of muscular support increases the load on the discs and facet joints, leading to further nociceptive signalling.
The Surgical Trauma as a "Second Hit"
By the time a patient is offered a fusion, their nervous system is already sensitised. The surgery acts as a "second hit." The massive physical trauma of the procedure, the disruption of the fascia, and the stripping of muscles from the bone create a massive wave of afferent signalling to the brain. In a system that is already hyper-vigilant, this trauma is not processed as a healing event but as a further assault. The "post-surgical paradox" is that the surgery designed to stabilise the spine often destabilises the nervous system, leading to a permanent state of chronic pain that is far worse than the original discomfort.
Data from the UK’s National Health Service (NHS) suggests that up to 40% of patients who undergo spinal surgery for chronic pain do not experience significant long-term relief, with a substantial portion reporting worsened symptoms.
##
What the Mainstream Narrative Omits
The drive toward spinal fusion is fuelled by a combination of biomechanical reductionism and financial incentives that the mainstream narrative rarely acknowledges. There is a glaring omission of the "Bio-Psycho-Social" model in favour of the "Biomedical-Industrial" model.
The Profit Margin of Hardware
Spinal fusion is a lucrative business. The cost of the hardware alone—the screws, cages, and plates—can run into thousands of pounds per case. Hospitals and private clinics are incentivised to perform fusions over more conservative, time-consuming, and less profitable interventions like specialised physiotherapy or cognitive functional therapy. This creates a systemic bias toward surgical intervention, even when the evidence for its efficacy in non-specific back pain is weak to non-existent.
The Myth of the "Fixed" Spine
The mainstream narrative presents the spine as a mechanical structure that can be "fixed" like a car. This ignores the dynamic nature of biology. A fused spine is not a "fixed" spine; it is a modified spine. The narrative omits the fact that once you fuse one level, you are essentially signing the patient up for a lifetime of monitoring and potentially more surgeries as the adjacent segments fail. They also omit the reality of perineural fibrosis—the formation of scar tissue around the nerve roots—which is an almost inevitable consequence of opening the spinal canal and is a leading cause of post-surgical leg pain.
The Placebo and Nocebo Effect
There is compelling evidence that a significant portion of the "success" in spinal surgery is due to the placebo effect. The "theatre" of surgery—the general anaesthesia, the incisions, the authoritative surgeon—is a powerful psychological intervention. Conversely, when the surgery fails, the "nocebo" effect of being told "the fusion didn't take" or "your spine is still unstable" can trap a patient in a cycle of despair that further sensitises their nervous system. The mainstream narrative rarely discusses the power of the mind in modulating pain, fearing it sounds "unscientific," yet it is one of the most well-documented biological realities in pain science.
##
The UK Context
In the United Kingdom, the approach to spinal fusion is a study in contrasts. While the National Institute for Health and Care Excellence (NICE) has issued clear guidelines recommending against spinal fusion for non-specific low back pain, the procedure remains common, particularly in the private sector and in certain NHS trusts.
The NHS Postcode Lottery
The availability and recommendation of spinal fusion in the UK often depend on where a patient lives—the infamous "postcode lottery." Some trusts have moved toward a more multidisciplinary approach, focusing on the "Back-Skills Training" (BeST) programme, which emphasises psychological and physical rehabilitation. Others, however, continue to maintain high surgical rates. The GIRFT (Get It Right First Time) initiative in the UK has highlighted the massive variability in spinal surgery outcomes across the country, calling for a radical rethink of how we manage back pain.
The Private Sector Surge
As NHS waiting lists for "elective" surgeries have grown, there has been a significant surge in patients seeking spinal fusion through private medical insurance or self-pay. In the private sector, the constraints of NICE guidelines are often more loosely applied, and the financial incentives for surgeons to operate are more direct. This has led to a situation where the most invasive and risky procedures are being marketed to desperate patients as "cutting-edge" solutions.
According to recent UK healthcare audits, the cost of treating chronic back pain exceeds £12 billion annually, yet the quality of life for chronic sufferers has not significantly improved in decades, largely due to the over-reliance on structural interventions.
##
Protective Measures and Recovery Protocols
If the biological case against unnecessary spinal fusion is so strong, what is the alternative? Recovery from chronic back pain—and the prevention of the need for surgery—requires a shift from "fixing the structure" to "calming the system."
Calming the Neuro-Immune System
The first step in any recovery protocol is to lower the "threat level" of the nervous system. This involves:
- —Pain Education: Understanding that pain does not always equal damage. Learning about central sensitisation can, in itself, lower the brain's alarm response.
- —Sleep Hygiene: Deep sleep is the only time the brain's glymphatic system clears out metabolic waste. It is also when the body releases the majority of its growth hormone for tissue repair.
- —Anti-Inflammatory Nutrition: Moving away from the "Western Diet" (high in refined sugars and seed oils) toward a diet rich in Omega-3 fatty acids, polyphenols, and antioxidants helps to dampen systemic neuroinflammation.
Movement as Medicine: Cognitive Functional Therapy (CFT)
Traditional "rehab" often focuses on "core stability," which can actually lead to more muscle guarding and tension. Cognitive Functional Therapy, an approach gaining traction in the UK, focuses on restoring relaxed, natural movement. By gradually exposing the body to the movements it fears, the patient can "re-train" the brain to recognise that the spine is robust and capable of movement without danger.
The Biological Scaffold: Supplementation and Lifestyle
To support the health of the intervertebral discs and bone, certain biological interventions are crucial:
- —Magnesium and Vitamin D3/K2: Essential for bone metabolism and muscle relaxation. Most UK citizens are chronically deficient in Vitamin D, particularly in the winter months, which directly impacts bone density and immune function.
- —Collagen Peptides and Vitamin C: These provide the raw materials for collagen synthesis within the annulus fibrosus and the bone matrix.
- —Vagus Nerve Stimulation: Techniques such as breathwork and cold exposure can help shift the body from a "sympathetic" (fight or flight) state into a "parasympathetic" (rest and digest) state, which is the only state in which true tissue healing can occur.
Avoiding the "Surgical Trap"
The most protective measure a patient can take is to seek multiple opinions and specifically ask about the biological evidence for surgery. If a surgeon cannot explain how the procedure will address the "chemical" and "neurological" aspects of pain—and only focuses on the "mechanical" aspect—it is a significant red flag.
##
Summary: Key Takeaways
The biological case against unnecessary spinal fusion is rooted in the recognition that the human spine is a living, sensing system, not a mechanical bridge. The failure of arthrodesis to solve chronic pain is not usually a failure of the surgeon's skill, but a failure of the underlying medical philosophy.
- —Mechanical Solutions for Biological Problems: Fusing vertebrae fails because it ignores the cellular and neurological reality of pain. It addresses the "image" on a scan rather than the "environment" of the body.
- —The Cascade of Failure: Surgery often acts as a "second hit" to a sensitised nervous system, leading to glial cell activation, chronic neuroinflammation, and Adjacent Segment Disease.
- —Systemic Disruptors: Metabolic health, smoking, and chronic stress are the primary drivers of fusion failure. Without addressing these, surgery is often a doomed endeavour.
- —The Profit Factor: The mainstream narrative is heavily influenced by the financial gains associated with spinal hardware, often leading to the over-prescription of invasive procedures.
- —The UK Landscape: Despite NICE guidelines, spinal fusion rates remain high, particularly in the private sector, highlighting a need for patients to be more informed and critical of surgical recommendations.
- —The Path Forward: Recovery lies in "systemic desensitisation"—using movement, nutrition, and psychological education to calm the nervous system and support the body's innate capacity for healing.
At INNERSTANDING, we advocate for a paradigm shift. We must move away from the "structural fix" and toward a "biological harmony." The spine is designed to move, to feel, and to adapt. When we try to silence its signals with screws and rods without understanding the message it is sending, we are not practicing medicine; we are merely managing a biological crisis with the wrong tools. The future of spinal health is not in the operating theatre, but in the cellular and neurological empowerment of the individual.
This article is provided for informational and educational purposes only. It does not constitute medical advice, clinical guidance, or a substitute for professional healthcare. Information reflects cited research at time of publication. Always consult a qualified healthcare professional before acting on any health information.
RESEARCH FOUNDATIONS
Biological Credibility Archive
Citations provided for educational reference. Verify via PubMed or institutional databases.
Medical Disclaimer
The information in this article is for educational purposes only and does not constitute medical advice, diagnosis, or treatment. Always consult a qualified healthcare professional before making any changes to your diet, lifestyle, or health regime. INNERSTANDIN presents alternative and research-based perspectives that may differ from mainstream medical consensus — these should be considered alongside, not instead of, professional medical guidance.
Read Full DisclaimerReady to learn more?
Continue your journey through our classified biological research.
DISCUSSION ROOM
Members of THE COLLECTIVE discussing "Spinal Arthrodesis Failures: The Biological Case Against Unnecessary Surgery"
SILENT CHANNEL
Be the first to discuss this article. Your insight could help others understand these biological concepts deeper.
RABBIT HOLE
Follow the biological thread deeper