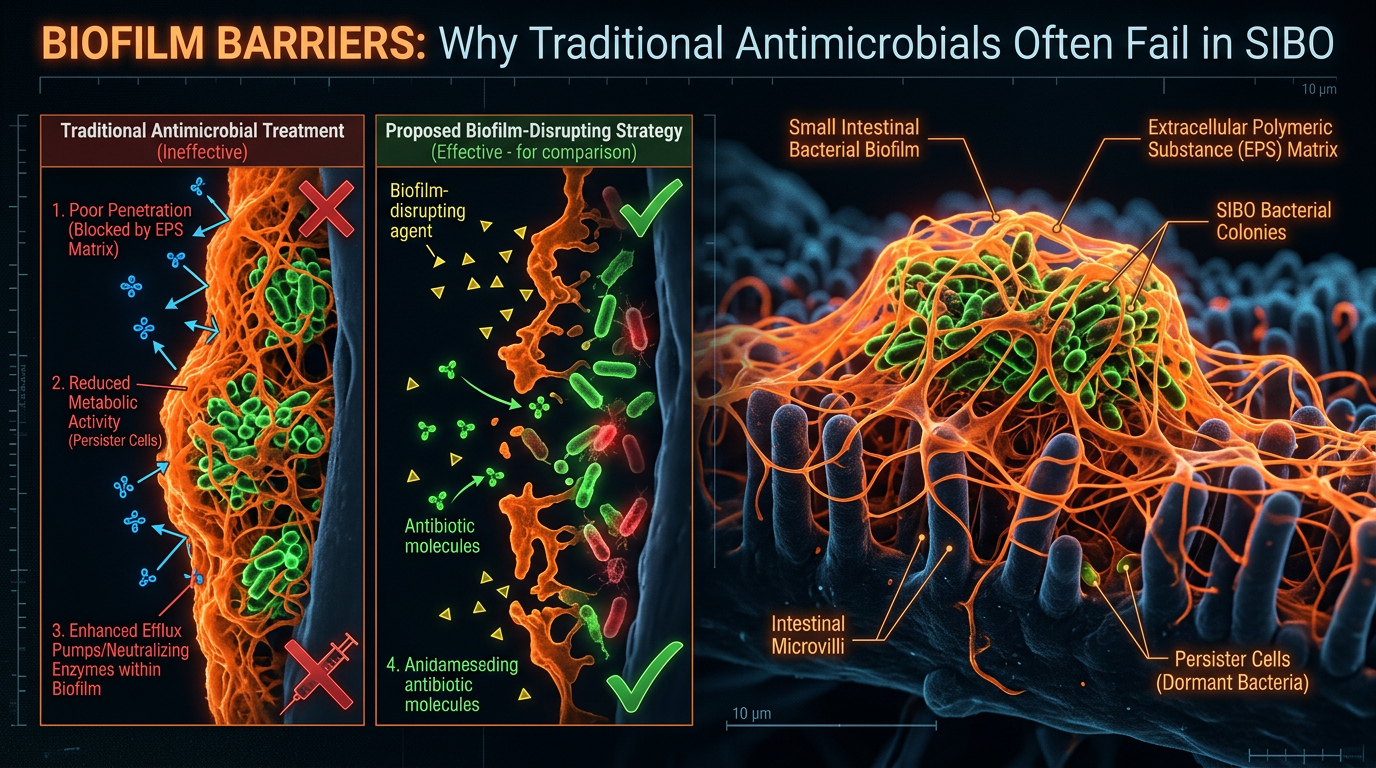
Biofilm Barriers: Why Traditional Antimicrobials Often Fail in SIBO
Bacterial colonies in the small intestine protect themselves with a sticky extracellular matrix known as a biofilm. These structures shield pathogens from both the immune system and pharmaceutical interventions.
Overview
The persistent failure of conventional gastroenterology to address Small Intestinal Bacterial Overgrowth (SIBO) effectively is not merely a clinical oversight; it is a fundamental misunderstanding of microbial ecology. For decades, the mainstream medical establishment has treated SIBO as a simple arithmetic problem—an excess of bacteria in the wrong place that requires subtraction via pharmaceutical antimicrobials. However, the patient reality in the United Kingdom and globally tells a different story: one of chronic relapse, systemic inflammation, and a "revolving door" of antibiotic prescriptions that yield diminishing returns.
The missing link in this diagnostic and therapeutic failure is the biofilm. In the harsh environment of the human digestive tract, bacteria do not exist as isolated, free-swimming (planktonic) entities. Instead, they are sophisticated, communal organisms that construct complex, self-protecting fortresses known as biofilms. These structures are not merely passive shields; they are highly engineered extracellular matrices that act as a sophisticated biological "cloaking device," rendering the microbial inhabitants up to 1,000 times more resistant to antibiotics, botanicals, and the host’s innate immune system.
To understand why SIBO remains one of the most stubborn conditions in functional medicine, one must look beyond the bacteria themselves and examine the architecture of their survival. Biofilms represent a paradigm shift in our understanding of chronic infection. They explain why a patient can complete a rigorous fourteen-day course of Rifaximin or Neomycin, experience a fleeting window of symptomatic relief, and then suffer a total resurgence of symptoms within weeks. We are not dealing with a simple infection; we are dealing with an entrenched, multi-species biological occupation.
According to recent UK health surveys, approximately 15-20% of the British population suffers from Irritable Bowel Syndrome (IBS), a significant portion of which (up to 78%) is now believed to be caused by underlying SIBO. Yet, the standard NHS "treatment" pathway frequently fails to account for the protective role of biofilms, leading to a cycle of chronic illness.
##
The Biology — How It Works
A biofilm is a collective of microorganisms in which cells stick to each other and often also to a surface. These adherent cells become embedded within a slimy extracellular matrix that is composed of Extracellular Polymeric Substances (EPS). This matrix is the "mortar" between the "bricks" of the bacterial colony.
The Lifecycle of a Biofilm Fortress
The formation of a biofilm in the small intestine is a meticulously choreographed four-stage process that transforms a transient bacterial population into a permanent biological fixture.
- —Initial Attachment: The process begins when planktonic bacteria, often driven into the small intestine by impaired motility (the Migrating Motor Complex), encounter the mucosal lining. Through specialised proteins called adhesins, they latch onto the intestinal wall. At this stage, the process is still reversible.
- —Irreversible Adhesion and Microcolony Formation: Once attached, the bacteria undergo a dramatic shift in gene expression. They stop investing energy in flagella (movement) and begin secreting the EPS matrix. They begin to multiply, forming clusters known as microcolonies.
- —Maturation: The "city" is built. The EPS matrix thickens, incorporating proteins, lipids, and even Extracellular DNA (eDNA) stolen from the host or dead bacteria. The biofilm develops a complex three-dimensional architecture, complete with "water channels" that circulate nutrients and remove waste products. This is no longer a collection of individuals; it is a multicellular organism.
- —Dispersal: Once the colony reaches a critical mass or becomes stressed by external factors (like an antibiotic), it releases "scout" cells back into the planktonic state to colonise other segments of the small intestine. This is why SIBO often feels like a "moving target" for clinicians.
Quorum Sensing: The Bacterial Internet
Biofilms are governed by a sophisticated communication system called Quorum Sensing (QS). Bacteria secrete signalling molecules known as autoinducers. As the population density increases, so does the concentration of these molecules. When a certain threshold (a "quorum") is reached, it triggers a simultaneous change in the behaviour of the entire colony.
Through QS, the biofilm can coordinate its defences. It can sense the presence of an antibiotic and collectively "decide" to pump out the toxin using multi-drug efflux pumps, or it can shift the entire colony’s metabolism into a dormant state to wait out the chemical storm. This is the biological equivalent of an entire city switching off its lights and retreating to underground bunkers when an air-raid siren sounds.
##
Mechanisms at the Cellular Level
To appreciate why a biofilm is nearly impenetrable to traditional medicine, we must examine the specific cellular and biochemical mechanisms that define its resistance.
The Diffusion Barrier
The EPS matrix acts as a physical and chemical filter. Antibiotics are typically designed to target specific metabolic processes in actively dividing, free-floating bacteria. However, the negatively charged polysaccharides and eDNA within the biofilm matrix can trap positively charged antibiotic molecules, preventing them from ever reaching the bacteria at the core. In the case of aminoglycoside antibiotics, the matrix can literally "bind" the drug, neutralising it on contact.
Metabolic Heterogeneity and Persister Cells
Within the 3D structure of a biofilm, oxygen and nutrient gradients are formed. Bacteria at the surface are metabolically active, while those deep within the core are oxygen-starved and nutrient-deprived. These core bacteria enter a state of metabolic "suspended animation."
Since most antibiotics (such as those that inhibit cell wall synthesis) require the bacteria to be actively dividing to work, these dormant bacteria are inherently immune. These are known as Persister Cells. When the course of antibiotics ends and the "active" surface layer of the biofilm has been stripped away, these Persister Cells "wake up," re-multiply, and rebuild the fortress. This is the primary mechanism of SIBO relapse.
Horizontal Gene Transfer (HGT)
A biofilm is a hotbed for genetic evolution. Because the bacteria are packed so tightly together in a protective environment, they frequently exchange genetic material through a process called conjugation. If one bacterium in the colony possesses a plasmid for antibiotic resistance, it can rapidly share that "defence code" with neighbouring species—even those of different genera. This creates a multi-drug resistant "super-colony" within the small intestine that is exponentially more dangerous than the sum of its parts.
Crucial Fact: Research indicates that the rate of Horizontal Gene Transfer within a biofilm is up to 1,000 times higher than in planktonic populations. This makes the gut a literal laboratory for the creation of treatment-resistant SIBO.
##
Environmental Threats and Biological Disruptors
The modern environment, particularly in highly industrialised nations like the UK, provides the perfect "catalyst" for biofilm formation. The bacteria are not creating these shields in a vacuum; they are doing so as a survival response to an increasingly toxic internal environment.
The Role of Heavy Metals
Biofilms have a high affinity for heavy metals such as mercury, lead, and aluminium. In fact, bacteria often incorporate these metals into their matrix to provide structural rigidity. The metals act as a "scaffold," making the biofilm harder and more resistant to enzymatic breakdown. For the patient, this creates a "toxic synergy": the biofilm protects the bacteria, and the bacteria sequester heavy metals, preventing the body’s natural detoxification pathways from clearing them.
Glyphosate and Pesticide Exposure
The UK’s agricultural reliance on glyphosate-based herbicides has profound implications for gut health. Glyphosate acts as a potent chelator, stripping minerals like manganese and zinc from the host while selectively killing "beneficial" bacteria like *Lactobacillus* and *Bifidobacterium*. Pathogenic bacteria, such as *E. coli* and *Salmonella*, are often resistant to glyphosate. This shift in the microbial landscape triggers a stress response in the remaining pathogens, encouraging them to form biofilms as a protective measure against the chemical onslaught.
Chlorinated Water and Microplastics
The UK water supply, while "safe" by regulatory standards, is heavily chlorinated. Chronic exposure to low-level chlorine is a known trigger for biofilm production in water pipes—and the same principle applies to the human gut. Furthermore, the burgeoning crisis of microplastics provides "rafts" or physical substrates upon which bacteria can begin the initial attachment phase of biofilm formation, facilitating the transport of pathogens deep into the small intestinal tract.
##
The Cascade: From Exposure to Disease
The presence of an entrenched biofilm in the small intestine initiates a systemic cascade of biological decay. It is not a localised problem; it is a systemic emergency.
The Destruction of the Brush Border
The EPS matrix doesn't just sit on top of the intestinal lining; it embeds itself into the glycocalyx—the delicate hair-like projections (microvilli) on the surface of enterocytes. This physical occupation blunts the microvilli, leading to:
- —Malabsorption: The body can no longer effectively absorb B12, iron, and fat-soluble vitamins (A, D, E, K).
- —Disaccharidase Deficiency: The enzymes needed to break down sugars (lactase, sucrase) are located on the tips of these microvilli. When the biofilm destroys the tips, the patient develops profound "food intolerances" to carbohydrates, which in turn feed the biofilm bacteria.
Molecular Mimicry and Autoimmunity
The chronic immune activation caused by the biofilm's presence leads to "Leaky Gut" (Increased Intestinal Permeability). As the biofilm shed proteins and LPS (lipopolysaccharides) into the bloodstream, the immune system becomes hyper-vigilant. Through a process called molecular mimicry, the immune system may begin to attack host tissues that resemble bacterial proteins. This is a primary driver in the link between SIBO and autoimmune conditions like Hashimoto’s thyroiditis and Rheumatoid Arthritis.
The Vagus Nerve and the Motility Trap
Biofilms produce neurotoxic metabolic byproducts that can impair the function of the Enteric Nervous System. Specifically, they can inhibit the Migrating Motor Complex (MMC)—the "cleansing wave" that moves debris and bacteria out of the small intestine during fasting. This creates a vicious cycle: the biofilm impairs motility, and impaired motility allows the biofilm to grow larger and more entrenched.
##
What the Mainstream Narrative Omits
The current medical model for SIBO is fundamentally reductionist. It relies almost exclusively on the Hydrogen/Methane Breath Test and a subsequent "kill phase" using Rifaximin. There are several critical flaws in this narrative that INNERSTANDING seeks to expose.
The "Sterile Gut" Fallacy
Mainstream gastroenterology often speaks as if the goal is to "wipe out" the overgrowth. This is biologically impossible and ecologically disastrous. The goal should be the restoration of *eubiosis*—a healthy balance. By focusing solely on "killing," practitioners often ignore the fact that the "scaffold" (the biofilm) remains. When the antibiotic treatment stops, the remaining bacteria simply move back into the pre-existing housing. This is why "re-treatment" rates are so high.
The Failure to Address "Phase II" Biofilms
Most practitioners who *do* acknowledge biofilms use simple disruptors like NAC (N-Acetyl Cysteine). While helpful, NAC only addresses "Phase I" or early-stage biofilms. Older, more mature biofilms incorporate minerals like calcium, magnesium, and iron into their matrix. These "Phase II" biofilms require advanced chelating agents and specific enzymes (like bismuth subnitrate or serrapeptase) to be broken down. Ignoring the maturity of the biofilm is a recipe for clinical failure.
The Myth of the "Standard" Diet
The UK's standard dietary advice for IBS—the Low FODMAP diet—is often used as a "treatment" for SIBO. While it can reduce symptoms by "starving" the bacteria of their preferred fuel, it does nothing to dismantle the biofilm matrix. In fact, prolonged Low FODMAP dieting can cause the bacteria to retreat even further into the biofilm state as a survival mechanism, making them even harder to eradicate later.
##
The UK Context
In the United Kingdom, the challenge of SIBO and biofilm-related illness is compounded by a healthcare system that is decades behind the current microbiological research.
The NHS Postcode Lottery
Access to SIBO breath testing on the NHS is notoriously difficult. Many GPs still view SIBO as a "niche" or "alternative" diagnosis, despite the overwhelming evidence linking it to IBS. Patients are often told their symptoms are purely psychosomatic or are given "wastebasket" diagnoses of IBS and prescribed anti-spasmodics or low-dose antidepressants, which do absolutely nothing to address the underlying bacterial fortress.
The Antibiotic Resistance Crisis
The UK government has rightfully highlighted antibiotic resistance as a major public health threat. However, the over-prescription of antibiotics for SIBO—without addressing the biofilm—is a significant contributor to this problem. When we use Rifaximin repeatedly without success, we are effectively "training" the gut microbiota to resist the very tools we have left to fight them.
UK Statistics: Public Health England (now UKHSA) has reported that nearly 20% of all antibiotic prescriptions in the UK may be unnecessary. In the context of SIBO, the "unnecessary" part isn't the intent to treat, but the *method* of treatment that fails to bypass the biofilm barrier, leading to repeated, ineffective dosing.
The Environmental Load in Britain
The UK's high density of "hard water" areas (particularly in the South and East of England) means many patients are consuming high levels of calcium and magnesium in their tap water. While these are essential minerals, in the context of an active SIBO infection, they can be "harvested" by bacteria to reinforce the biofilm matrix, making the condition significantly more difficult to treat in these regions compared to "soft water" areas.
##
Protective Measures and Recovery Protocols
Dismantling a SIBO biofilm requires a strategic, multi-phased approach that goes far beyond simple antimicrobial therapy. One must "unmask" the bacteria before attempting to eliminate them.
Phase 1: Biofilm Disruption (The Unmasking)
Before introducing any "killing" agents (botanical or pharmaceutical), the matrix must be destabilised. This requires a combination of:
- —Thiol-based Disruptors: N-Acetyl Cysteine (NAC) and Alpha-Lipoic Acid can help break down the disulfide bonds in the EPS matrix.
- —Enzymatic Degradation: Using specific enzymes like Interfase Plus or high-dose Serrapeptase and Lumbrokinase. These enzymes "digest" the proteins and fibrin that hold the biofilm together.
- —Chelation: Mature biofilms are held together by metal ions. Using agents like Bismuth Subnitrate or EDTA (under strict clinical supervision) can "pull" the minerals out of the biofilm wall, causing the structure to collapse.
Phase 2: Precision Eradication
Only once the biofilm is "leaky" should antimicrobials be introduced. In the INNERSTANDING protocol, we prioritise potent, broad-spectrum botanicals that have inherent anti-biofilm properties, such as:
- —Allicin (from Garlic): One of the few substances capable of penetrating the biofilm and inhibiting the "Quorum Sensing" communication between bacteria.
- —Oil of Oregano (Emulsified): Highly effective against the lipid components of the bacterial cell wall.
- —Berberine: Acts as a potent efflux pump inhibitor, preventing the bacteria from "spitting out" the antimicrobial agents.
Phase 3: The Prokinetic and Motility Support
The most critical step in preventing relapse is ensuring the bacteria cannot re-establish their fortress. This requires "re-booting" the Migrating Motor Complex.
- —Ginger and Artichoke Extracts: Proven to stimulate antral contractions in the stomach and small intestine.
- —Low-dose Erythromycin or Prucalopride: Pharmaceutical prokinetics that may be necessary in severe cases to ensure the small intestine remains a "running stream" rather than a "stagnant pond."
Phase 4: Re-acidification and Mucosal Repair
A biofilm thrives in an alkaline or neutral small intestine. Restoring the natural acidic gradient of the upper GI tract using Betaine HCl (if appropriate) makes the environment hostile to colonisation. Furthermore, the use of Immunoglobulins (SBI) can help "mop up" the LPS and bacterial debris released during the biofilm breakdown, preventing a "Herxheimer" or "die-off" reaction.
##
Summary: Key Takeaways
- —SIBO is a Biofilm Disease: The failure of traditional treatments is almost always due to the presence of an Extracellular Polymeric Substance (EPS) matrix that shields bacteria from drugs and the immune system.
- —Persistence Over Resistance: Bacteria in a biofilm aren't always "resistant" in the genetic sense; they are "persistent" because they are dormant. If you don't wake them up and break their shield, they will return.
- —The Environment Matters: UK-specific factors like hard water, glyphosate exposure, and chlorinated water supplies provide the raw materials and the "stress signals" that encourage bacteria to build biofilms.
- —Mainstream Medicine is Lagging: The "kill only" approach is an ecological failure. Effective SIBO resolution requires a "Disrupt, Kill, Flush, Protect" cycle.
- —Metals are the Scaffold: Mature (Phase II) biofilms use calcium, iron, and heavy metals as structural reinforcements. Successful treatment often requires the use of mineral chelators and specialised enzymes.
- —Motility is the Final Frontier: You cannot successfully treat SIBO/Biofilms if the "conveyor belt" of the small intestine is broken. Prokinetic support is not optional; it is the foundation of long-term recovery.
The path to overcoming SIBO is not found in a single "magic bullet" antibiotic. It is found in the meticulous and scientific dismantling of the bacterial fortress. By understanding the biology of the biofilm, we can finally stop treating the symptoms and start addressing the structural reality of the disease. At INNERSTANDING, we advocate for this "Ecological Medicine"—a paradigm that respects the complexity of the microbiome while ruthlessly exposing the mechanisms that allow pathogens to thrive. The "Biofilm Barrier" is the last great hurdle in gut health; once crossed, true systemic healing becomes possible.
This article is provided for informational and educational purposes only. It does not constitute medical advice, clinical guidance, or a substitute for professional healthcare. Information reflects cited research at time of publication. Always consult a qualified healthcare professional before acting on any health information.
RESEARCH FOUNDATIONS
Biological Credibility Archive
Citations provided for educational reference. Verify via PubMed or institutional databases.
Medical Disclaimer
The information in this article is for educational purposes only and does not constitute medical advice, diagnosis, or treatment. Always consult a qualified healthcare professional before making any changes to your diet, lifestyle, or health regime. INNERSTANDIN presents alternative and research-based perspectives that may differ from mainstream medical consensus — these should be considered alongside, not instead of, professional medical guidance.
Read Full DisclaimerReady to learn more?
Continue your journey through our classified biological research.
DISCUSSION ROOM
Members of THE COLLECTIVE discussing "Biofilm Barriers: Why Traditional Antimicrobials Often Fail in SIBO"
SILENT CHANNEL
Be the first to discuss this article. Your insight could help others understand these biological concepts deeper.
THE ARSENAL
Based on SIBO & Small Intestine Health — products curated by our research team for educational relevance and biological support.

Magnesium Blend – The Most Important Mineral

Clean Slate – Detoxes thousands of chemicals,heavy metals, pesticides, allergens, mold spores and fungus

Vegan Essential Amino Acids – Plant-Powered Protein Building
INNERSTANDING may earn a commission on purchases made through these links. All products are selected based on rigorous educational relevance to our biological research.
RABBIT HOLE
Follow the biological thread deeper