Enzymatic Co-Factors: The Thiamine-Magnesium Synergy in Pyruvate Dehydrogenase Complex Function
An in-depth investigation into the biochemical necessity of magnesium for thiamine activation and its collective role in the Pyruvate Dehydrogenase Complex, the essential bridge for cellular energy production.

# Enzymatic Co-Factors: The Thiamine-Magnesium Synergy in Pyruvate Dehydrogenase Complex Function\n\nIn the landscape of cellular bioenergetics, the transition from glycolysis to the Krebs cycle represents a pivotal 'checkpoint' in human metabolism. At the heart of this transition lies the Pyruvate Dehydrogenase Complex (PDC), a multi-enzyme assembly that converts pyruvate into acetyl-CoA. However, this complex is not self-sustaining; its function is entirely dependent on a delicate synergy between two essential micronutrients: Thiamine (Vitamin B1) and Magnesium (Mg).\n\nFor practitioners and health enthusiasts focused on root-cause wellness, understanding this synergy is paramount. Without adequate magnesium, thiamine remains biologically inert, and without thiamine, the body cannot efficiently oxidise glucose, leading to a cascade of metabolic dysfunctions ranging from chronic fatigue to neurological decline.\n\n## The PDC: The Gatekeeper of Aerobic Metabolism\n\nThe Pyruvate Dehydrogenase Complex is a massive mitochondrial structure comprised of three distinct enzymes: pyruvate transacetylase (E1), dihydrolipoyl transacetylase (E2), and dihydrolipoyl dehydrogenase (E3). Its primary role is to link the anaerobic process of glycolysis (occurring in the cytoplasm) with the aerobic ATP-generating machinery of the mitochondria.\n\nWhen the PDC functions optimally, pyruvate is decarboxylated and transformed into Acetyl-CoA, which then enters the Citric Acid Cycle.
When the PDC fails, pyruvate is diverted into the production of lactate. This shift not only results in significantly lower ATP yield (2 ATP vs. 36 ATP) but also contributes to intracellular acidosis, a state often associated with mitochondrial disease and metabolic syndrome.\n\n## Thiamine: The Active Catalyst\n\nThiamine acts as the primary co-enzyme for the E1 subunit of the PDC. However, the thiamine consumed via diet or supplementation is not the form used by the mitochondria. It must first be phosphorylated into Thiamine Pyrophosphate (TPP). This conversion is the first point of the magnesium-thiamine intersection.
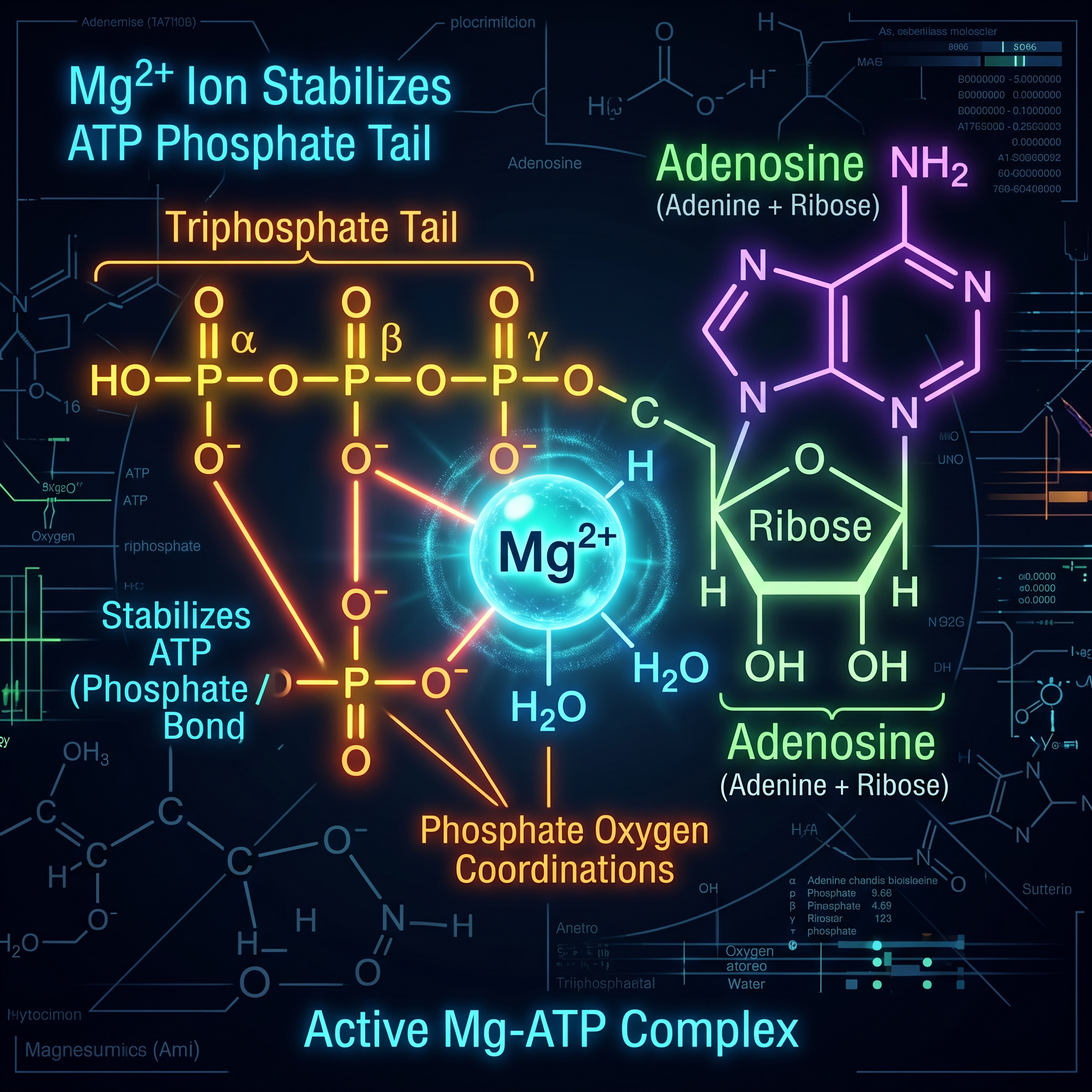
The enzyme responsible for this transformation, thiamine pyrophosphokinase, requires magnesium as a mandatory co-factor. \n\nWithout sufficient magnesium, even high doses of supplemental thiamine cannot be converted into TPP. This creates a functional thiamine deficiency, where blood levels of B1 may appear normal, yet the cellular machinery is starving for the activated form.\n\n## Magnesium: The Structural Anchor\n\nBeyond the activation of thiamine, magnesium serves a structural role within the PDC itself. In the E1 subunit, magnesium acts as a 'bridge' or a divalent cation anchor that holds the TPP molecule in the correct orientation within the enzyme's active site. This binding allows for the decarboxylation of pyruvate to occur.\n\nResearch suggests that the affinity of the E1 enzyme for TPP is significantly reduced in magnesium-deficient states. Effectively, magnesium provides the lock-and-key stability required for the metabolic spark to ignite.
Without this stability, the PDC becomes 'decoupled,' and the flow of energy substrates into the mitochondria is bottlenecked.\n\n## The Magnesium-Thiamine Paradox\n\nA critical clinical phenomenon known as the 'Magnesium-Thiamine Paradox' occurs when thiamine is administered in the presence of an underlying magnesium deficiency. Because thiamine administration ramps up the demand for ATP and enzymatic activity, it rapidly consumes the remaining cellular magnesium stores. \n\nIn severe cases, such as the treatment of Wernicke-Korsakoff syndrome or refeeding syndrome, providing thiamine without magnesium can exacerbate neurological symptoms or lead to metabolic collapse. In a broader context, individuals attempting to resolve 'brain fog' or fatigue with B-complex vitamins may find their symptoms worsening or plateauing if they do not concurrently address their magnesium status.\n\n## Root Causes of Co-Factor Depletion\n\nIn modern clinical practice, we rarely see isolated deficiencies. The depletion of the PDC co-factors is typically driven by systemic factors:\n\n1. High Carbohydrate Intake: Diets high in refined sugars and flours increase the demand for the PDC to process glucose, rapidly 'burning through' thiamine and magnesium supplies.\n2. Chronic Stress: The HPA-axis activation increases the excretion of magnesium through the kidneys, while stress-induced metabolic demand taxes B-vitamin stores.\n3. Alcohol Consumption: Alcohol is a potent antagonist to thiamine absorption and interferes with the renal reabsorption of magnesium, making it a 'perfect storm' for PDC dysfunction.\n4. Soil Depletion: Industrial farming practices have significantly reduced the magnesium content of staple crops, making it difficult to reach the RDA through food alone.\n\n## Clinical Signs of PDC Bottlenecks\n\nWhen the synergy between thiamine and magnesium fails, the symptoms are often multisystemic. Because the brain and heart have the highest mitochondrial density, they are usually the first to manifest signs of dysfunction:\n\n* Neurological: Irritability, 'brain fog,' poor memory, and in advanced stages, ataxia or peripheral neuropathy.\n* Cardiovascular: Tachycardia, exercise intolerance, and fluid retention (classically associated with 'Wet Beriberi').\n* Metabolic: Elevated fasting lactate levels, unexplained muscle soreness, and post-exertional malaise.\n\n## Optimising the Synergy: Practical Considerations\n\nTo restore the function of the Pyruvate Dehydrogenase Complex, a coordinated approach is required.
Supplementing with high-potency thiamine (such as benfotiamine or thiamine HCl) must be balanced with bioavailable magnesium.\n\nMagnesium Malate is often the preferred form for metabolic support, as malate is itself an intermediate in the Krebs cycle, providing an additional layer of energy support. Magnesium Bisglycinate is also excellent for its high absorption rate and neurological calming effects.\n\nFurthermore, the presence of other B-vitamins (specifically Riboflavin/B2 for the E3 subunit and Niacin/B3 for NAD+ production) and Alpha-Lipoic Acid (a co-factor for the E2 subunit) ensures that the entire PDC assembly is supported, rather than just one link in the chain.\n\n## Conclusion\n\nThe Pyruvate Dehydrogenase Complex is a testament to the complexity and interconnectedness of human biochemistry. It serves as a reminder that nutrients do not work in isolation. The synergy between thiamine and magnesium is the foundational key to unlocking cellular energy. By ensuring the adequacy of both co-factors, we can support the root-cause of metabolic health, allowing the body to efficiently turn fuel into the vitality required for life.

Methylene Blue – Advanced Cellular Chemistry
A pharmaceutical-grade compound designed to optimise mitochondrial function and cellular energy production. This high-purity formula supports metabolic efficiency and mental clarity by acting as a powerful electron donor within your cells.
Vetting Notes
Pending
This article is provided for informational and educational purposes only. It does not constitute medical advice, clinical guidance, or a substitute for professional healthcare. Information reflects cited research at time of publication. Always consult a qualified healthcare professional before acting on any health information.
RESEARCH FOUNDATIONS
Biological Credibility Archive
Citations provided for educational reference. Verify via PubMed or institutional databases.
Medical Disclaimer
The information in this article is for educational purposes only and does not constitute medical advice, diagnosis, or treatment. Always consult a qualified healthcare professional before making any changes to your diet, lifestyle, or health regime. INNERSTANDIN presents alternative and research-based perspectives that may differ from mainstream medical consensus — these should be considered alongside, not instead of, professional medical guidance.
Read Full DisclaimerReady to learn more?
Continue your journey through our classified biological research.
DISCUSSION ROOM
Members of THE COLLECTIVE discussing "Enzymatic Co-Factors: The Thiamine-Magnesium Synergy in Pyruvate Dehydrogenase Complex Function"
SILENT CHANNEL
Be the first to discuss this article. Your insight could help others understand these biological concepts deeper.
THE ARSENAL
Based on Magnesium Forms, Functions & Deficiency — products curated by our research team for educational relevance and biological support.

Magnesium Blend – The Most Important Mineral
Methylene Blue – Advanced Cellular Chemistry

Energy Blend Supports
INNERSTANDING may earn a commission on purchases made through these links. All products are selected based on rigorous educational relevance to our biological research.
RABBIT HOLE
Follow the biological thread deeper