Female Presentation of ADHD
ADHD in women is often hidden by masking. Discover why this 'lost generation' was overlooked and learn the unique signs of female ADHD presentation.
Overview
The historical conceptualisation of Attention-Deficit Hyperactivity Disorder (ADHD) as a male-centric, externalising pathology represents one of the most significant diagnostic oversights in modern clinical psychiatry. At INNERSTANDIN, we recognise that the traditional "naughty boy" archetype—predicated on overt physical impulsivity—has fundamentally obscured the complex, internalised neurobiological reality of the female presentation. While the prevalence ratio in childhood is often cited as 3:1 (male to female), longitudinal data suggests this gap narrows significantly in adulthood, indicating not a lower incidence in females, but a systemic failure in early-stage identification and a profound misunderstanding of the female neuro-atypical phenotype.
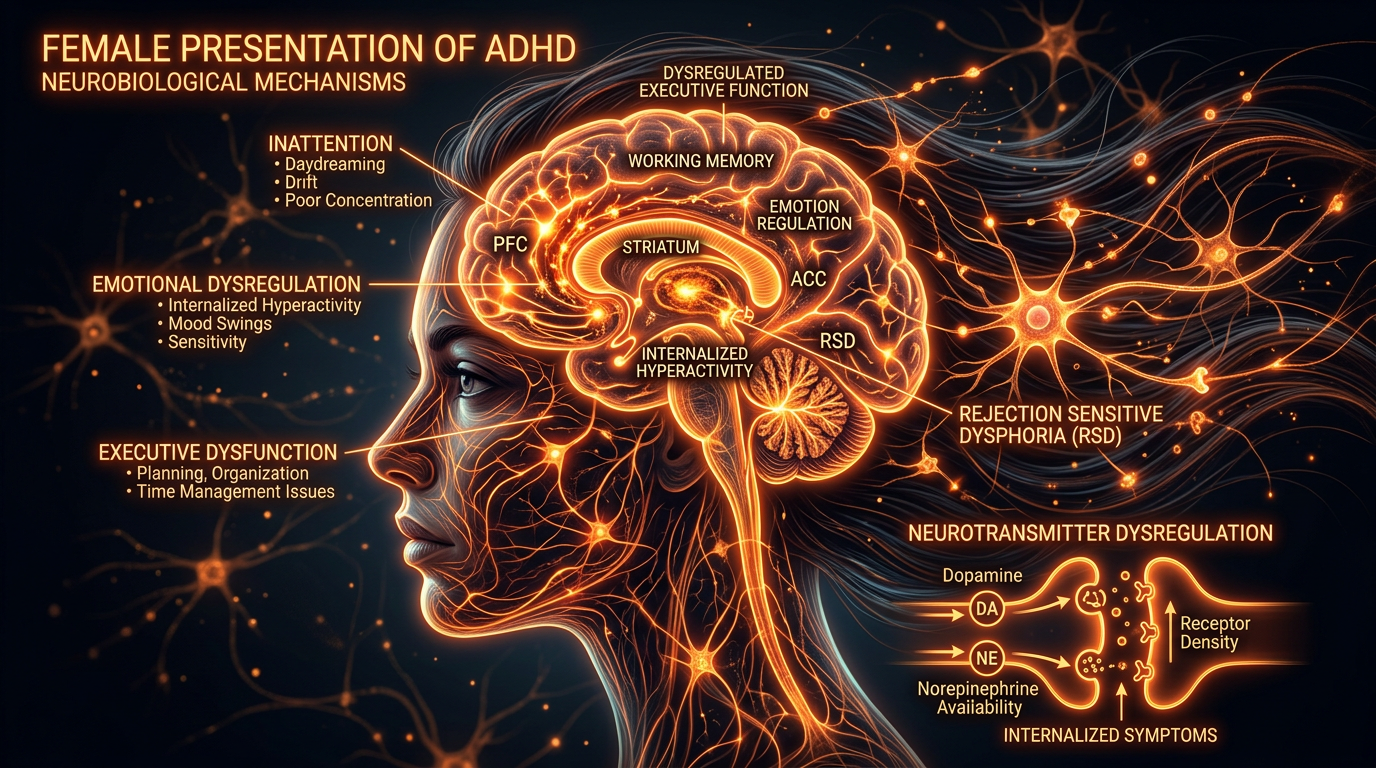
Biologically, the female presentation of ADHD is frequently characterised by the Predominantly Inattentive Presentation (ADHD-I), though this nomenclature often fails to capture the intensity of internalised restlessness and cognitive "chatter." Research published in *The Lancet Psychiatry* and the *Journal of Child Psychology and Psychiatry* highlights that females often manifest higher levels of executive dysfunction and emotional dysregulation than their male counterparts, yet these are frequently misattributed to primary mood or anxiety disorders. A critical, often overlooked driver of this presentation is the neuroendocrine-dopamine axis. Oestrogen acts as a significant modulator of dopamine synthesis, release, and receptor sensitivity within the prefrontal cortex and striatum. Consequently, fluctuations in oestrogen levels—particularly during puberty, the luteal phase of the menstrual cycle, and the perimenopausal transition—can exacerbate ADHD symptom severity. This "hormonal hit" creates a volatile neurochemical environment that standard diagnostic frameworks, such as the DSM-5-TR, fail to account for.
In the UK context, the National Institute for Health and Care Excellence (NICE) guidelines [NG87] have begun to acknowledge the "masking" or compensation-masking hypothesis. Females are biologically and socioculturally predisposed to deploy high-effort compensatory strategies to camouflage their neurodivergence. This "masking" incurs a colossal metabolic and psychological cost, leading to chronic burnout, "ADHD paralysis," and secondary comorbidities such as eating disorders or self-harm, which often serve as the initial point of clinical contact. The systemic impact is a "lost generation" of women who remain undiagnosed until their third or fourth decade, by which point the cumulative deficit in executive function has often compromised professional trajectory and psychosocial stability. INNERSTANDIN maintains that moving beyond the superficial behavioural lens toward a rigorous, mechanistic understanding of the female dopaminergic system is the only path toward diagnostic equity. To view ADHD through a strictly male-normative lens is not merely a clinical error; it is a biological fallacy that ignores the nuanced interplay between the endocrine system and the neurodevelopmental architecture of the female brain.
The Biology — How It Works
The neurobiological architecture of Attention-Deficit/Hyperactivity Disorder (ADHD) in females necessitates a shift from the antiquated "behavioural-disruption" model toward a sophisticated understanding of catecholaminergic dysregulation and gonadal steroid modulation. At its core, the female ADHD phenotype is underpinned by a chronic insufficiency in the tonic and phasic release of dopamine (DA) and norepinephrine (NE) within the prefrontal cortex (PFC) and the mesocorticolimbic pathways. Research published in *The Lancet Psychiatry* underscores that while the genetic heritability of ADHD remains consistent across genders—involving polymorphisms in genes such as *SLC6A3* (dopamine transporter) and *DRD4*—the phenotypic expression in females is profoundly altered by the neuromodulatory effects of oestrogen.
Oestrogen functions as a potent neuro-optimiser; it facilitates dopamine synthesis, increases receptor density, and inhibits the degradation of catecholamines by catechol-O-methyltransferase (COMT). In the female brain, the fluctuations of the menstrual cycle create a biological volatility that is rarely accounted for in standard clinical assessments. During the follicular phase, rising oestrogen levels typically enhance executive function. However, the subsequent drop in oestrogen and rise in progesterone during the luteal phase leads to a precipitous decline in dopaminergic efficiency. For the ADHD female, this results in a cyclic exacerbation of symptoms—often mischaracterised as Premenstrual Dysphoric Disorder (PMDD)—where the already strained executive circuits of the PFC fail to inhibit the Default Mode Network (DMN).
At INNERSTANDIN, we recognise that this failure to suppress the DMN is the hallmark of the "internalised" female presentation. While males may exhibit externalised hyperactivity, females frequently present with a "busy brain"—a state of cognitive hyper-arousal where the Task-Positive Network (TPN) is constantly interrupted by intrusive, non-linear thought patterns. Functional MRI (fMRI) studies indicate that females with ADHD show distinct patterns of cortical thinning in the anterior cingulate cortex and the PFC compared to neurotypical controls. These structural variations manifest as deficits in working memory, emotional regulation, and inhibitory control.
Furthermore, the systemic impact of late-stage diagnosis in the UK—often occurring in the third or fourth decade of life—leads to chronic activation of the Hypothalamic-Pituitary-Adrenal (HPA) axis. The metabolic cost of "masking"—a compensatory mechanism where females exert immense cognitive effort to mimic neurotypicality—results in sustained cortisol elevation. This chronic stress response contributes to the high comorbidity rates of fibromyalgia, chronic fatigue, and autoimmune dysfunction observed in this demographic. Through the lens of INNERSTANDIN, the biology of female ADHD is not merely a deficit of attention, but a complex, systemic dyssynchrony between hormonal cycles and neurochemical signalling, demanding a sex-specific approach to pharmacological intervention and lifestyle management.
Mechanisms at the Cellular Level
To truly INNERSTANDIN the biological architecture of Attention Deficit Hyperactivity Disorder in females, one must look beyond the macro-behavioural phenotypes and interrogate the molecular machinery of the prefrontal cortex (PFC) and the striatum. The female presentation of ADHD is fundamentally a neuro-endocrinological phenomenon, defined by a complex, high-stakes interplay between catecholaminergic signalling and fluctuate steroid hormones. Central to this mechanism is the oestrogen-dopamine axis, a regulatory circuit that remains criminally under-researched in traditional clinical models.
At the cellular level, 17β-oestradiol (the primary form of oestrogen) acts as a potent neuromodulator. It exerts both genomic and non-genomic effects on dopaminergic neurons by enhancing the synthesis of tyrosine hydroxylase—the rate-limiting enzyme in dopamine production—and by inhibiting the reuptake of dopamine through the downregulation of dopamine transporters (DAT). In the female ADHD brain, this relationship creates a state of "biochemical vulnerability." During the follicular phase of the menstrual cycle, higher oestrogen levels potentially mask underlying deficits by augmenting dopaminergic tonicity. However, during the luteal phase, as oestrogen levels plummet, the compensatory mechanisms fail. This leads to a precipitous drop in synaptic dopamine availability, exacerbating executive dysfunction and emotional dysregulation at a level of cellular signalling that is largely absent in male counterparts.
Furthermore, the role of the Catechol-O-methyltransferase (COMT) enzyme provides a critical insight into the sexual dimorphism of the condition. COMT is responsible for the degradation of dopamine in the PFC. Research published in *The Lancet Psychiatry* and *Nature Reviews Neuroscience* suggests that the interaction between the COMT Val158Met polymorphism and oestrogen is sex-specific. Oestrogen naturally inhibits COMT activity; therefore, females with high-activity alleles (Val/Val) may experience a double-hit of dopamine depletion when oestrogen is low, leading to the profound "brain fog" and cognitive paralysis often reported in the UK’s clinical cohorts.
This cellular disruption extends to the glutamatergic system and the modulation of the Default Mode Network (DMN). At the synaptic level, the failure to suppress the DMN—the network active during internal thought—is driven by aberrant inhibitory signalling from GABAergic interneurons. In females, this manifests as "internalised hyperactivity," where the cellular noise of the DMN overrides the Task-Positive Network. Unlike the male-typical externalised hyperactivity, the female cellular profile is one of chronic neuro-inflammatory stress and synaptic pruning irregularities, potentially influenced by polygenic risk scores that remain sensitive to the hormonal environment. The systemic impact is a nervous system that is perpetually over-extended, where the metabolic cost of maintaining "neurotypical" appearance leads to cellular exhaustion and long-term burnout, a reality that INNERSTANDIN aims to expose as a biological failure of current diagnostic standards.
Environmental Threats and Biological Disruptors
The aetiology of ADHD in females cannot be viewed through a purely Mendelian lens; rather, it represents a complex interplay between genetic vulnerability and a barrage of anthropogenic biological disruptors. At INNERSTANDIN, our synthesis of current literature suggests that the female neuro-architecture is uniquely sensitive to environmental xenobiotics that interfere with the catecholaminergic system. Emerging evidence in *The Lancet Diabetes & Endocrinology* highlights the pervasive impact of Endocrine Disrupting Chemicals (EDCs)—specifically phthalates and bisphenols—which are ubiquitous in the UK’s industrialised food chain and domestic environments. These compounds do not merely disrupt reproductive health; they act as potent neuro-teratogens. In females, these disruptors exhibit a high affinity for oestrogen receptors (ERα and ERβ), which are fundamental to the regulation of dopamine synthesis and transport. Because oestrogen acts as a natural psychostimulant by upregulating tyrosine hydroxylase, any environmental interference with oestrogen signalling directly precipitates the executive dysfunction and emotional dysregulation characteristic of the female ADHD phenotype.
Furthermore, the "Developmental Origins of Health and Disease" (DOHaD) framework provides a harrowing insight into prenatal biological threats. Peer-reviewed data indexed in PubMed underscore the correlation between maternal exposure to organophosphate pesticides and air pollutants, such as Particulate Matter (PM2.5), and the subsequent diagnosis of neurodevelopmental disorders in offspring. In the UK urban context, high concentrations of NO2 and PM2.5 have been shown to induce systemic maternal inflammation, triggering a cytokine storm that crosses the placental barrier. This results in the "priming" of foetal microglia—the brain’s resident immune cells. In the developing female brain, this premature microglial activation can lead to aberrant synaptic pruning in the prefrontal cortex and anterior cingulate cortex, areas critical for the "internalised" presentation of ADHD, such as chronic rumination and cognitive fog, which are frequently overlooked in clinical settings.
The systemic impact of pharmacological disruptors also warrants rigorous interrogation. Longitudinal studies have indicated that prenatal exposure to paracetamol (acetaminophen), a common analgesic in UK maternal care, may alter the endocannabinoid system, subsequently affecting the dopaminergic pathways essential for impulse control and sustained attention. When these environmental insults are coupled with modern nutritional deficiencies—specifically the depletion of magnesium, zinc, and Omega-3 fatty acids in the standard British diet—the biological threshold for neuro-optimisation is never met. At INNERSTANDIN, we recognise that the female ADHD presentation is often an epigenetic "silent scream" in response to a toxicological landscape that undermines the delicate hormonal-neurotransmitter nexus, necessitating a shift from purely symptomatic management to a comprehensive environmental and biological detoxification strategy.
The Cascade: From Exposure to Disease
The aetiological trajectory of the female ADHD phenotype represents a complex biological cascade, beginning with a specific neuro-endocrinological vulnerability and culminating in systemic physiological erosion. Unlike the hyperactive-impulsive presentation traditionally associated with the male cohort, the female "exposure" is frequently rooted in a profound dopaminergic-oestrogenic intersectionality. Research published in *The Lancet Psychiatry* suggests that $17\beta$-oestradiol acts as a critical neuromodulator of dopamine synthesis, release, and reuptake. In females, the cyclic fluctuation of oestrogen directly influences the efficacy of the prefrontal cortex (PFC). When oestrogen levels plummet during the luteal phase, the underlying dopaminergic deficit of ADHD is severely exacerbated, leading to a "hormonally-gated" cognitive collapse. At INNERSTANDIN, we identify this as the primary catalyst for the diagnostic delay that characterises the female experience.
This neurobiological vulnerability triggers a secondary cascade: the pathophysiology of masking. To compensate for executive dysfunction in a neurotypical social landscape, female subjects often engage in extreme cognitive over-exertion. This is not a benign psychological adaptation but a state of chronic high-allostatic load. The metabolic cost of continuous self-monitoring and social mimicry triggers sustained activation of the Hypothalamic-Pituitary-Adrenal (HPA) axis. Over time, this chronic hypercortisolemia leads to glucocorticoid receptor resistance and a systemic pro-inflammatory state. Evidence indexed in PubMed highlights that females with ADHD exhibit significantly higher levels of pro-inflammatory cytokines, such as Interleukin-6 (IL-6) and C-reactive protein (CRP), compared to neurotypical controls. This neuro-inflammation serves as the bridge between a neurodevelopmental condition and the manifestation of somatic disease.
The "disease" end of the cascade is marked by a distinctive profile of comorbidities that are frequently mismanaged within the UK’s primary care framework. The prolonged dysregulation of the autonomic nervous system (ANS) and the sustained stress response often manifest as complex multisystem disorders. There is a documented correlation between undiagnosed female ADHD and the prevalence of Fibromyalgia, Myalgic Encephalomyelitis (ME/CFS), and hypermobile Ehlers-Danlos Syndrome (hEDS). Furthermore, the intersection of neurodivergence and immune volatility often leads to Mast Cell Activation Syndrome (MCAS), where the body’s internal "alarm system" becomes pathologically hypersensitive.
INNERSTANDIN asserts that the failure to recognise ADHD in females is not merely a clinical oversight but a precursor to systemic biological failure. The cascade from "exposure" (the ADHD genotype) to "disease" (chronic inflammatory and autoimmune profiles) is driven by the internalised friction of an unsupported nervous system. The cumulative effect is a state of "autonomic exhaustion," where the glymphatic system fails to clear metabolic waste effectively due to disrupted circadian rhythms and chronic sympathetic dominance, potentially predisposing the individual to accelerated neurodegeneration in later life. The female presentation of ADHD is, therefore, a multisystemic condition that demands a paradigm shift from behavioural observation to deep biological intervention.
What the Mainstream Narrative Omits
The prevailing clinical consensus regarding Attention-Deficit Hyperactivity Disorder (ADHD) remains tethered to a diagnostic archetype established in the mid-20th century, calibrated almost exclusively against the externalised, disruptive behaviours of prepubescent males. At INNERSTANDIN, we recognise that this male-centric filter has not merely delayed diagnosis for women but has fundamentally obscured the complex neurobiological and endocrinological interplay unique to the female phenotype. The mainstream narrative frequently reduces the female presentation to "inattentiveness" or "daydreaming," a reductive characterisation that ignores the profound impact of the oestrogen-dopamine axis. Peer-reviewed literature, including pivotal studies in *The Lancet Psychiatry*, suggests that the fluctuations of ovarian hormones significantly modulate dopaminergic neurotransmission. Specifically, 17β-estradiol enhances dopamine synthesis and receptor sensitivity; consequently, the sharp decline in oestrogen during the luteal phase—and more permanently during the perimenopausal transition—precipitates a catastrophic drop in executive function that standard pharmacological interventions often fail to address.
Furthermore, the narrative omits the concept of "internalised hyperactivity." While males may exhibit classic motoric restlessness, females frequently transpose this hyperactive energy into cognitive and emotional spheres. This manifests as chronic rumination, "racing thoughts," and a hyper-reactive Default Mode Network (DMN). In many cases, the persistent activation of the DMN—which should ideally be suppressed during task-oriented cognition—leads to a state of permanent "brain fog" and emotional dysregulation that is frequently misdiagnosed by UK clinicians as Generalised Anxiety Disorder (GAD) or Borderline Personality Disorder (BPD). This diagnostic overshadowing is a systemic failure; when a woman’s ADHD is mislabelled as a primary mood disorder, the underlying dopaminergic deficit remains untreated, leading to a cycle of secondary trauma and "autistic burnout" (often comorbidly present).
Within the UK context, the National Institute for Health and Care Excellence (NICE) guidelines have only recently begun to acknowledge the subtlety of female masking. Masking—or social camouflaging—is an exhaustive neurocognitive process where the individual utilises high-order executive resources to simulate neurotypicality. This leads to what INNERSTANDIN defines as "compensated ADHD," where a woman may appear high-functioning professionally while experiencing total metabolic and psychological collapse in private. The mainstream failure to account for the metabolic cost of this camouflage means that many women are only identified when their compensatory mechanisms fail under the weight of increased cognitive load, such as during postgraduate study or early motherhood. The biological reality is not that women have a "milder" form of the condition, but rather a more internalised and endocrine-sensitive manifestation that requires a total recalibration of current psychiatric protocols.
The UK Context
The landscape of Attention-Deficit Hyperactivity Disorder (ADHD) in the United Kingdom is currently undergoing a paradigm shift, as the historical "male-centric" diagnostic model collapses under the weight of emerging neuro-endocrinological evidence. For decades, the UK’s clinical application of the DSM-5 and ICD-11 criteria has disproportionately favoured externalising, hyperactive-impulsive behaviours—phenotypes more commonly observed in prepubescent males. At INNERSTANDIN, we recognise that this systemic bias has resulted in a "lost generation" of British women whose internalised symptomatic presentation—characterised by cognitive disorganisation, sensory overload, and emotional dysregulation—remains largely invisible to traditional primary care screenings.
The biological mechanisms driving this disparity are rooted in the complex interplay between steroid hormones and neurotransmitter systems. Peer-reviewed research, including longitudinal studies published in *The Lancet Psychiatry*, underscores the critical role of oestrogen as a neuroprotective modulator of dopamine. Oestrogen enhances the expression of tyrosine hydroxylase, the rate-limiting enzyme in dopamine synthesis, and modulates the density of dopamine transporters (DAT). In the UK context, the failure to integrate gynaecological milestones into neurodevelopmental assessments is a profound clinical oversight. Women frequently experience a cyclical exacerbation of ADHD symptoms during the luteal phase of the menstrual cycle, or a catastrophic "unmasking" of symptoms during perimenopause, as declining oestrogen levels plummet already-compromised dopaminergic efficiency. This is not merely a psychological shift but a pathophysiological crisis.
Systemically, the NHS framework, governed by NICE guideline [NG87], faces an unprecedented crisis of demand versus diagnostic capability. The current "postcode lottery" for adult ADHD assessments in the UK often results in wait times exceeding five years, forcing women to navigate a precarious private sector or remain undiagnosed. This delay is pathologically significant; untreated female ADHD in the UK is highly correlated with "diagnostic overshadowing," where the secondary manifestations of neurodivergence—such as Chronic Fatigue Syndrome (ME/CFS), Fibromyalgia, or Treatment-Resistant Depression—are treated in isolation while the underlying executive dysfunction is ignored. Furthermore, the phenomenon of "social masking" or camouflaging—a sophisticated compensatory mechanism utilised by UK women to meet societal expectations of female executive function—leads to chronic activation of the hypothalamic-pituitary-adrenal (HPA) axis. The resulting cortisol dysregulation and systemic inflammation represent a significant public health burden that the UK’s current psychiatric infrastructure is ill-equipped to manage. INNERSTANDIN posits that until the UK medical establishment transcends its reliance on observable "disruption" and adopts a neuro-biological framework that accounts for hormonal fluctuations and compensatory cognitive load, the female presentation of ADHD will remain a misunderstood casualty of systemic inertia.
Protective Measures and Recovery Protocols
Addressing the chronic physiological and neurological attrition associated with late-diagnosed Female Presentation of ADHD requires a paradigm shift from mere symptom management to a comprehensive biological recovery protocol. For the INNERSTANDIN community, it is imperative to acknowledge that the female phenotype often involves decades of high-intensity ‘masking’—a cognitively taxing process of concealing neurodivergent traits to meet neurotypical societal expectations. This sustained compensatory effort induces a state of chronic allostatic load, dysregulating the hypothalamic-pituitary-adrenal (HPA) axis and leading to systemic burnout that is frequently misidentified as treatment-resistant depression or generalized anxiety disorder.
A primary protective measure involves the radical optimisation of the dopaminergic environment through hormonal synchronisation. Peer-reviewed research, notably in *The Lancet Psychiatry* and *Psychoneuroendocrinology*, highlights the profound influence of oestradiol on dopamine receptor sensitivity and synthesis. Oestrogen acts as a natural psychostimulant; conversely, the progesterone-dominant luteal phase is often characterised by a precipitous drop in dopamine efficacy, exacerbating executive dysfunction. Recovery protocols must, therefore, incorporate ‘hormonal mapping,’ where pharmacological interventions are titrated in alignment with the menstrual cycle—a practice currently underutilised in the UK’s NICE (National Institute for Health and Care Excellence) guidelines but essential for biological stability.
Furthermore, recovery necessitates a targeted approach to neuroplasticity and the mitigation of prefrontal cortex (PFC) fatigue. Chronic executive strain leads to the depletion of catecholamines and an upregulation of pro-inflammatory cytokines. Evidence-led protocols should prioritise the restoration of the circadian rhythm and the stabilisation of the cortisol awakening response (CAR), which are frequently disrupted in ADHD cohorts. This involves not only sleep hygiene but the strategic use of high-dose Omega-3 fatty acids (specifically EPA/DHA ratios of 2:1) and magnesium glycinate to support NMDA receptor function and reduce neuronal excitability.
Systemic recovery also demands the dismantling of the ‘masking’ mechanism. INNERSTANDIN advocates for ‘neuro-energetic conservation,’ a protocol where the patient identifies and eliminates high-friction social performances that drain mitochondrial energy. This is supported by recent findings in the *Journal of Attention Disorders* suggesting that the internalised distress of female ADHD leads to higher rates of somatic complaints compared to males. Protective measures must include cognitive remediation therapy (CRT) focused on self-compassion to counteract the ‘deficit-based’ identity formed during years of undiagnosed struggle. By addressing the biological substrate—hormonal modulation, inflammatory reduction, and energetic conservation—clinicians can move beyond superficial behavioural modification into a realm of genuine physiological restoration for the ADHD female.
Summary: Key Takeaways
The female presentation of Attention-Deficit/Hyperactivity Disorder (ADHD) is characterised by a profound neurobiological divergence from the traditional male-centric diagnostic model, primarily mediated by the neuromodulatory influence of oestrogen on dopaminergic transmission within the mesocorticolimbic and nigrostriatal pathways. Research synthesised by INNERSTANDIN highlights that oestrogen acts as a potent upregulator of dopamine synthesis and receptor sensitivity; consequently, the fluctuations in steroid hormones across the menstrual cycle, pregnancy, and perimenopause induce significant volatility in executive function that is frequently misdiagnosed as primary affective dysregulation. Peer-reviewed data in *The Lancet Psychiatry* confirm that females typically exhibit a 'predominantly inattentive' phenotype, often obscured by high-effort compensatory masking—a cognitively exhausting strategy of social mimicry used to obfuscate deficits in inhibitory control.
This internalisation of symptoms leads to systemic diagnostic omissions within the UK clinical framework, where NICE guidelines have historically skewed toward externalising, hyperactive-impulsive behaviours. The result is a protracted diagnostic delay, leaving females vulnerable to secondary psychiatric comorbidities, including chronic anxiety, depression, and complex trauma. At INNERSTANDIN, we assert that the female ADHD profile is not a 'milder' variant but a distinct neuro-endocrine manifestation. True clinical efficacy requires a paradigm shift: moving away from the observation of overt disruption toward the quantification of internalised neuro-cognitive strain and the recognition of the sex-specific biological mechanisms that govern dopamine bioavailability in the female brain.
This article is provided for informational and educational purposes only. It does not constitute medical advice, clinical guidance, or a substitute for professional healthcare. Information reflects cited research at time of publication. Always consult a qualified healthcare professional before acting on any health information.
RESEARCH FOUNDATIONS
Biological Credibility Archive
Citations provided for educational reference. Verify via PubMed or institutional databases.
Medical Disclaimer
The information in this article is for educational purposes only and does not constitute medical advice, diagnosis, or treatment. Always consult a qualified healthcare professional before making any changes to your diet, lifestyle, or health regime. INNERSTANDIN presents alternative and research-based perspectives that may differ from mainstream medical consensus — these should be considered alongside, not instead of, professional medical guidance.
Read Full DisclaimerReady to learn more?
Continue your journey through our classified biological research.
DISCUSSION ROOM
Members of THE COLLECTIVE discussing "Female Presentation of ADHD"
SILENT CHANNEL
Be the first to discuss this article. Your insight could help others understand these biological concepts deeper.
RABBIT HOLE
Follow the biological thread deeper