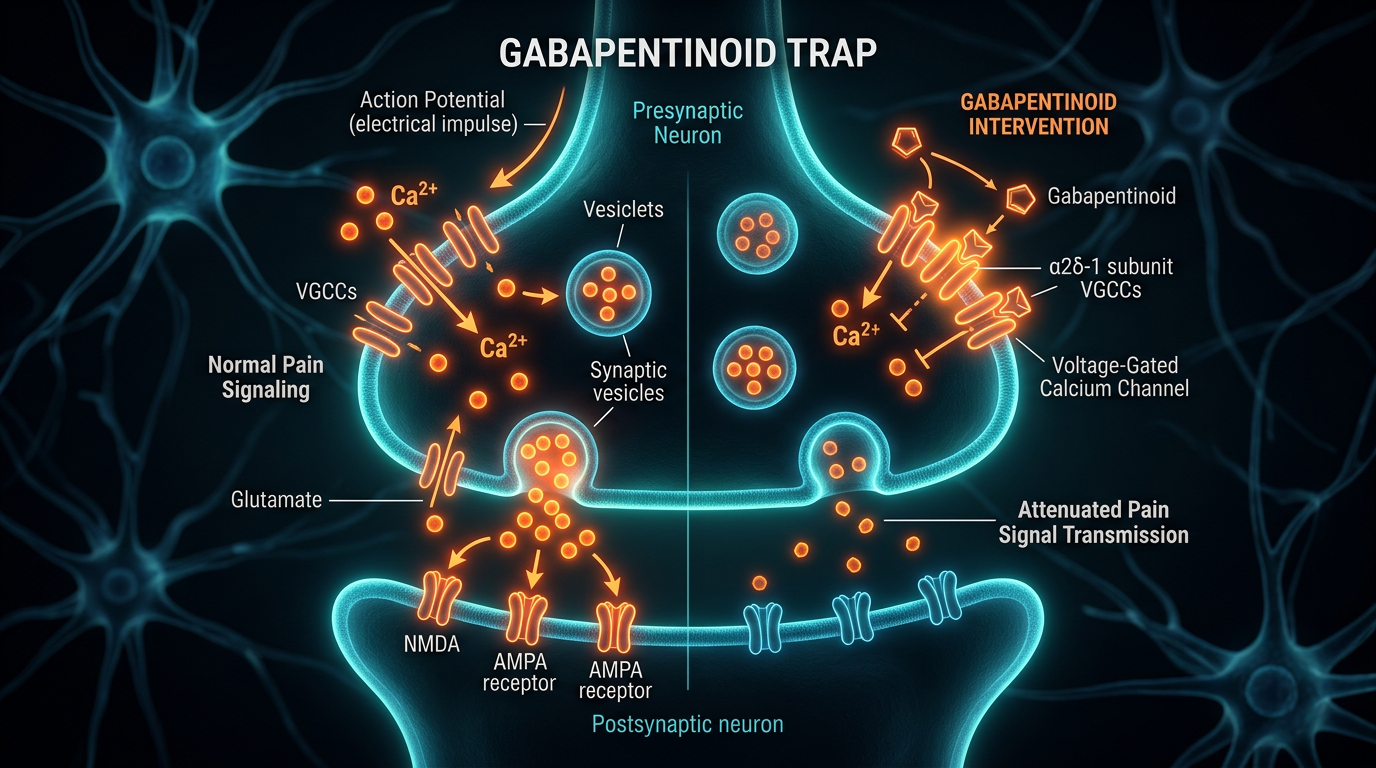
The Gabapentinoid Trap: Neurochemical Consequences of Nerve Pain Suppression
While widely prescribed for neuropathic pain, gabapentinoids significantly alter synaptic formation and cognitive function. We examine the long-term biological cost of these common prescriptions on the brain's structural integrity.
Overview
In the landscape of modern pharmacology, few classes of drugs have ascended to dominance as rapidly or as quietly as the gabapentinoids. Originally synthesised to mimic the inhibitory neurotransmitter gamma-aminobutyric acid (GABA), Gabapentin (Neurontin) and its more potent successor Pregabalin (Lyrica) were initially conceived as anticonvulsants. However, through an aggressive expansion of "off-label" applications and a desperate medical establishment seeking alternatives to the opioid crisis, these substances have become the standard of care for everything from diabetic neuropathy to generalised anxiety disorder.
But beneath the veneer of clinical utility lies a profound and troubling biological reality. We are currently witnessing a massive, uncontrolled experiment on the structural integrity of the human brain. The "Gabapentinoid Trap" refers to a phenomenon where the short-term suppression of nerve pain is bought at the cost of long-term neuroplasticity and synaptic formation. As a senior biological researcher for INNERSTANDING, I have observed that while these drugs effectively dampen the "noise" of damaged nerves, they do so by fundamentally altering the brain’s ability to build and maintain its own architecture.
The fundamental issue is not merely one of side effects; it is one of biological trade-offs. When we introduce a molecule that binds with high affinity to the $\alpha2\delta-1$ subunit of voltage-gated calcium channels, we are not simply "turning down the volume" on pain. We are interfering with the very machinery that allows neurons to communicate, adapt, and survive. This article serves as a comprehensive interrogation of the neurochemical consequences of gabapentinoid use, exposing the mechanisms by which these "nerve calmers" may be orchestrating a silent epidemic of cognitive decline and structural atrophy.
Between 2007 and 2017, prescriptions for gabapentinoids in England quadrupled, reaching over 14 million items per year, a trajectory that has only recently begun to face scrutiny by regulatory bodies.
##
The Biology — How It Works
To understand the trap, one must first understand the molecular target. Despite their name, gabapentinoids do not bind to GABA-A or GABA-B receptors. Their primary mechanism involves the $\alpha2\delta-1$ protein, a critical component of high-voltage-activated calcium channels found throughout the central nervous system.
The Calcium Channel Gateway
Calcium ions ($Ca^{2+}$) are the primary signalling molecules of the brain. When an electrical impulse reaches a nerve terminal, these calcium channels open, allowing an influx of ions that triggers the release of neurotransmitters into the synapse. In the context of chronic pain, these channels are often overactive, leading to a "wind-up" effect where the brain is flooded with excitatory signals like glutamate and Substance P.
Gabapentinoids bind to the $\alpha2\delta-1$ subunit, effectively reducing the density of these channels on the cell membrane and decreasing their activation. By inhibiting the influx of calcium, the drug reduces the release of excitatory neurotransmitters. In the short term, this is highly effective at reducing the "hypersensitivity" associated with nerve damage. The patient experiences a cessation of burning, stabbing, or electric-shock sensations.
The Problem of Specificity
The tragedy of the gabapentinoid mechanism is its lack of anatomical specificity. The $\alpha2\delta-1$ subunit is not unique to pain pathways; it is ubiquitous in the hippocampus (the seat of memory), the prefrontal cortex (the executive control centre), and the cerebellum (responsible for motor coordination). When a patient ingests Pregabalin for sciatica, the drug does not simply navigate to the lumbar spine; it saturates the entire cerebral cortex, dampening excitatory transmission globally. This results in the characteristic "brain fog" that patients frequently report—a state of induced cognitive lethargy where the brain's "spark" is systematically dimmed.
##
Mechanisms at the Cellular Level
The most alarming discovery in recent pain science involves the role of the $\alpha2\delta-1$ receptor beyond simple ion gating. Research, most notably out of Stanford University, has revealed that this receptor is the primary binding site for Thrombospondins (TSPs), proteins secreted by astrocytes that are essential for the formation of new excitatory synapses.
The Death of Synaptogenesis
In a healthy brain, astrocytes (support cells) release TSPs to signal to neurons that it is time to form a new connection. This process, known as synaptogenesis, is the biological basis of learning, memory, and recovery from injury. When Gabapentin or Pregabalin occupies the $\alpha2\delta-1$ receptor, it physically blocks TSPs from binding.
- —Synaptic Stagnation: The brain loses its ability to form new excitatory synapses. While existing synapses remain (for a time), the "wiring" of the brain becomes static.
- —Inhibition of Repair: In the wake of a stroke or traumatic brain injury, the brain relies on synaptogenesis to reroute signals. Gabapentinoids effectively "lock" the brain in its damaged state by preventing this remodelling.
- —Dendritic Pruning: Chronic exposure leads to a reduction in dendritic spine density, essentially thinning the forest of neural connections.
Research has shown that Gabapentin is a potent inhibitor of new synapse formation in the developing and adult brain, raising serious questions about its long-term use in populations requiring high levels of cognitive plasticity.
Mitochondrial Dysfunction
Furthermore, emergent evidence suggests that chronic gabapentinoid use interferes with mitochondrial trafficking within the neuron. Because these drugs alter calcium homeostasis, they disrupt the energetic balance of the cell. Neurons are incredibly energy-hungry; when their calcium signalling is artificially suppressed, the mitochondria—the powerhouses of the cell—fail to migrate to the synapses where they are needed most. This leads to synaptic fatigue and, eventually, neuronal apoptosis (programmed cell death).
##
Environmental Threats and Biological Disruptors
The "Gabapentinoid Trap" does not exist in a vacuum. Its effects are exacerbated by the modern environment, creating a synergistic profile of neurobiological decay. When a patient is prescribed these drugs, they are often already dealing with systemic inflammation, poor sleep, and nutritional deficiencies.
Synergistic Neurotoxicity
In the modern British lifestyle, exposure to ultra-processed foods, chronic blue light, and sedentary behaviour creates a "pro-inflammatory" state. When gabapentinoids are introduced into this environment:
- —Blood-Brain Barrier (BBB) Integrity: Chronic inflammation increases the permeability of the BBB, allowing gabapentinoids to reach higher concentrations in the brain than would otherwise be possible.
- —Glymphatic Clearance: These drugs are known to alter sleep architecture, specifically reducing REM sleep and deep slow-wave sleep. This prevents the "glymphatic system" from flushing out metabolic waste (like beta-amyloid) during the night, leading to a buildup of neurotoxic debris.
The Endocrine Interference
We must also consider the impact on the hypothalamic-pituitary-adrenal (HPA) axis. Gabapentinoids can suppress the release of certain gonadotropins, leading to lower levels of testosterone and oestrogen. Given that these hormones are neuroprotective, their suppression further leaves the brain vulnerable to the structural degradation mentioned previously. The patient is caught in a pincer movement: the drug is stopping the brain from building new connections, while the hormonal environment is failing to protect the ones that remain.
##
The Cascade: From Exposure to Disease
The progression from the first prescription to systemic neurochemical failure follows a predictable, yet devastating, cascade. It is rarely an overnight collapse; instead, it is a slow erosion of self.
Phase 1: The Honeymoon (Weeks 1-4)
The patient experiences significant pain relief. The dampened excitatory transmission provides an initial sense of "calm" or even mild euphoria. This is the period where the GP views the intervention as a success.
Phase 2: The Cognitive Softening (Months 2-6)
As synaptogenesis is consistently inhibited, the patient begins to notice "minor" issues. Misplacing keys, struggling to find words (anomic aphasia), and a general sense of being "behind a pane of glass." In the UK medical system, these are often dismissed as symptoms of the underlying pain or "getting older."
Phase 3: Structural Adaptation (6 Months - 2 Years)
The brain begins to homeostatically upregulate its calcium channels to overcome the drug’s blockade. This leads to tolerance. The patient requires higher doses to achieve the same pain relief, but the higher dose further inhibits synaptogenesis. The "trap" is now set. The brain’s architecture is now physically altered; it has fewer synapses and a higher density of dysfunctional receptors.
Phase 4: The Withdrawal Crisis and Permanent Deficit
When a patient attempts to cease the medication, the upregulated receptors are suddenly left "unmasked." This causes a massive, excitotoxic surge of glutamate.
- —Excitotoxicity: The over-activation of neurons leads to oxidative stress and cell death.
- —The "Rebound" Effect: Pain returns with a vengeance, often worse than the original injury (hyperalgesia).
- —Persistent Cognitive Impairment: For some, even after cessation, the "brain fog" does not fully lift, suggesting that the inhibition of synaptogenesis has left a permanent mark on the brain's structural integrity.
Public Health England (PHE) reported in 2019 that 1 in 4 adults in England were prescribed a potentially addictive drug, including gabapentinoids, with many remaining on them for years despite a lack of evidence for long-term efficacy.
##
What the Mainstream Narrative Omits
The pharmaceutical industry and many medical journals have long categorised gabapentinoids as "safe" alternatives to opioids. This narrative is built on a series of significant omissions and half-truths.
The "Non-Addictive" Myth
For years, Gabapentin and Pregabalin were marketed as having "low abuse potential." We now know this is categorically false. Pregabalin, in particular, has a significant "street value" and is frequently used to potentiate the effects of opioids or to mitigate the symptoms of withdrawal. The "high" associated with large doses of Pregabalin is a result of profound changes in the dopaminergic pathways of the nucleus accumbens—the same area targeted by cocaine and heroin.
The Failure of "Off-Label" Efficacy
Perhaps the most egregious omission is the lack of evidence for the conditions these drugs are most commonly prescribed for. While gabapentinoids are effective for specific neuropathic conditions (like post-herpetic neuralgia), they are frequently prescribed for non-specific lower back pain and fibromyalgia.
- —Meta-analyses have repeatedly shown that for chronic lower back pain, gabapentinoids offer no clinically significant benefit over placebo.
- —Yet, they remain a "first-line" treatment in many UK surgeries because they are perceived as "safer" than morphine.
The Teratogenic Risk
Mainstream narratives often gloss over the potential impact on future generations. Recent studies have pointed to an increased risk of major birth defects in children born to women taking Pregabalin during the first trimester. More subtly, the inhibition of synaptogenesis is a catastrophic mechanism to introduce to a developing foetus or a breastfeeding infant.
##
The UK Context
The United Kingdom has become a focal point for the gabapentinoid crisis. The NHS, strained by budget cuts and an ageing population, has inadvertently facilitated a "prescription-first" culture.
The Class C Reclassification
In April 2019, following a dramatic rise in drug-related deaths, the UK government reclassified Gabapentin and Pregabalin as Class C Controlled Substances under the Misuse of Drugs Act 1971. This was a reactive measure, acknowledging that these drugs were being diverted and misused on a massive scale.
In Scotland, the rate of drug-related deaths involving gabapentinoids is particularly high; Pregabalin was present in over 1,100 deaths in 2022 alone, often in combination with methadone or benzodiazepines.
The Socio-Economic Divide
There is a clear "pain gap" in the UK. Data suggests that prescriptions for gabapentinoids are significantly higher in the most deprived areas of the country—regions like the "rust belt" towns in the North of England and the central belt of Scotland. In these areas, where access to multidisciplinary pain clinics, physiotherapy, and psychological support is limited, GPs often feel they have no tool other than the prescription pad. This has led to the "chemical coshing" of the working class, where the structural causes of pain (physical labour, poor housing, stress) are masked by a drug that systematically erodes the patient's cognitive capacity to improve their own situation.
The Cost to the NHS
The financial burden is not merely the cost of the pills—which is substantial—but the long-term cost of managing the fallout. The NHS is now facing a wave of patients with "Pregabalin-induced cognitive impairment," a rise in falls among the elderly (due to ataxia caused by the drug), and the complex, resource-heavy requirements of supervised tapering programmes.
##
Protective Measures and Recovery Protocols
If you or someone you know is caught in the Gabapentinoid Trap, the path to recovery is not through abrupt cessation—which can be dangerous—but through a structured, biologically informed reclamation of neural function.
1. The Hyper-Slow Taper
The brain has physically adapted to the presence of the drug. To avoid excitotoxicity, the "stripping" of these receptors must be done with extreme caution.
- —The 10% Rule: Many advocates and enlightened clinicians suggest reducing the dose by no more than 10% per month.
- —Liquid Titration: In the final stages of a taper, using liquid formulations allows for the micro-adjustments necessary to prevent "rebound" pain and neurological distress.
2. Stimulating Synaptogenesis
To counteract the inhibition of synaptogenesis, one must aggressively pursue activities and substances that increase Brain-Derived Neurotrophic Factor (BDNF).
- —Aerobic Exercise: Vigorous exercise is the most potent natural stimulator of BDNF. It encourages the brain to rebuild the connections that gabapentinoids have pruned.
- —Lion's Mane Mushroom (*Hericium erinaceus*): This functional fungus contains hericenones and erinacines, which stimulate Nerve Growth Factor (NGF) and may aid in the recovery of damaged peripheral nerves.
- —Polyphenols: Compounds such as curcumin (with piperine) and resveratrol help reduce the neuro-inflammation that occurs during the withdrawal phase.
3. Nutritional Foundations for Repair
The "machinery" of the synapse requires specific building blocks that are often depleted in the chronic pain patient.
- —Omega-3 Fatty Acids (EPA/DHA): Essential for the structural integrity of neuronal membranes. High-dose, high-quality fish oil is non-negotiable for neural recovery.
- —Magnesium Threonate: Unlike other forms of magnesium, the *threonate* form effectively crosses the blood-brain barrier. It acts as a natural calcium channel blocker, helping to stabilise the "wind-up" of neurons without the structural damage caused by gabapentinoids.
- —B-Vitamin Complex (Methylated): Crucial for the myelination of nerves and the synthesis of neurotransmitters.
4. Cognitive Rehabilitation
The brain is a "use it or lose it" organ. During and after a taper, patients must engage in "cognitive physiotherapy." Learning a new language, playing a musical instrument, or even complex logic puzzles can force the brain to re-engage its synaptogenetic machinery, effectively "re-wiring" the areas that were silenced by the medication.
##
Summary: Key Takeaways
The Gabapentinoid Trap is a cautionary tale of what happens when we attempt to solve complex, systemic biological problems with a "silver bullet" that targets a fundamental mechanism of life.
- —Synaptic Blockade: Gabapentinoids do not just block pain; they block the formation of new excitatory synapses by interfering with the $\alpha2\delta-1$ / Thrombospondin pathway.
- —Cognitive Atrophy: The "brain fog" associated with these drugs is not a side effect; it is a direct manifestation of inhibited neuroplasticity and structural stagnation.
- —UK Crisis: The UK is currently grappling with a legacy of over-prescription, particularly in deprived areas, leading to a Class C reclassification and a rise in drug-related mortality.
- —The Need for Awareness: Patients must be informed that these drugs are not "GABA-boosters" but are potent modifiers of the brain's physical architecture.
- —Path to Recovery: Recovery is possible through a slow, meticulous taper combined with strategies to boost BDNF, such as exercise, specific supplementation, and cognitive challenge.
As we move forward in the field of pain science, we must move away from the "suppression model"—where we simply silence the nerves—and toward a "restoration model." The goal of pain management should not be to render the brain a static, silent organ, but to provide it with the resources it needs to heal, adapt, and remain integrated. The Gabapentinoid Trap has taught us that the price of silence is often too high. It is time to reclaim the structural integrity of the human mind.
This article is provided for informational and educational purposes only. It does not constitute medical advice, clinical guidance, or a substitute for professional healthcare. Information reflects cited research at time of publication. Always consult a qualified healthcare professional before acting on any health information.
RESEARCH FOUNDATIONS
Biological Credibility Archive
Citations provided for educational reference. Verify via PubMed or institutional databases.
Medical Disclaimer
The information in this article is for educational purposes only and does not constitute medical advice, diagnosis, or treatment. Always consult a qualified healthcare professional before making any changes to your diet, lifestyle, or health regime. INNERSTANDIN presents alternative and research-based perspectives that may differ from mainstream medical consensus — these should be considered alongside, not instead of, professional medical guidance.
Read Full DisclaimerReady to learn more?
Continue your journey through our classified biological research.
DISCUSSION ROOM
Members of THE COLLECTIVE discussing "The Gabapentinoid Trap: Neurochemical Consequences of Nerve Pain Suppression"
SILENT CHANNEL
Be the first to discuss this article. Your insight could help others understand these biological concepts deeper.
RABBIT HOLE
Follow the biological thread deeper