Gate Control Theory Revisited: The Bio-Physics of Sensory Competition
The classic Gate Control Theory explains how non-painful input can close the 'gates' to painful signals in the spinal cord. Modern applications of this bio-physical principle provide alternatives to chemical-based pain management.
Overview
The history of pain science is often divided into two distinct eras: the pre-1965 era of "Specificity Theory" and the post-1965 era of "Gate Control Theory." For centuries, the medical establishment viewed pain through a Cartesian lens—a simple, direct-wire system where a stimulus at the periphery (a burnt finger) travelled along a dedicated path to a specific "pain centre" in the brain. This linear, mechanical view suggested that the intensity of pain was always directly proportional to the amount of tissue damage. It was a model that failed to explain why soldiers on the battlefield often felt no pain despite horrific injuries, or why "phantom limb" pain persisted in the absence of a limb.
In 1965, Ronald Melzack and Patrick Wall published their seminal paper in *Science*, "Pain Mechanisms: A New Theory." This was the birth of Gate Control Theory (GCT), a revolutionary framework that moved the focus from passive transmission to active modulation. At its core, GCT proposes that the spinal cord contains a neurological "gate" that either blocks pain signals or allows them to continue to the brain. This "gate" is not a physical structure but a functional mechanism within the dorsal horn of the spinal cord. It represents the first sophisticated understanding of sensory competition—the idea that different types of nerve impulses compete for entry into the central nervous system.
For the modern seeker of health and sovereignty, revisiting Gate Control Theory is not merely an academic exercise; it is a necessity. We live in an era where chronic pain has been commodified, treated primarily through the blunt instrument of pharmacology. By understanding the biophysics of how the "gate" operates, we uncover the potential for non-chemical neuromodulation. This article will dissect the intricate biophysical dance between different nerve fibres and explain how we can leverage the body’s own electrical architecture to suppress pain, bypass the pharmaceutical industrial complex, and reclaim our biological autonomy.
##
The Biology — How It Works
To grasp the brilliance of Gate Control Theory, one must first understand the primary actors in this neural drama: the peripheral nerve fibres. These fibres are categorised by their diameter and the presence of a myelin sheath—a fatty insulation that determines the speed of signal transmission.
There are three primary players in the "gate" mechanism:
- —A-beta (Aβ) Fibres: These are large-diameter, highly myelinated fibres. They are the "express trains" of the nervous system, responsible for transmitting non-painful stimuli such as touch, pressure, and vibration. Because of their heavy insulation, they transmit signals at speeds of up to 75 metres per second.
- —A-delta (Aδ) Fibres: These are smaller-diameter, thinly myelinated fibres. They carry "fast pain" signals—the sharp, immediate prick of a needle or the sting of a burn.
- —C-fibres: These are the smallest, unmyelinated fibres. They are the "slow trains," carrying dull, aching, or burning sensations. Their transmission speed is a sluggish 0.5 to 2 metres per second.
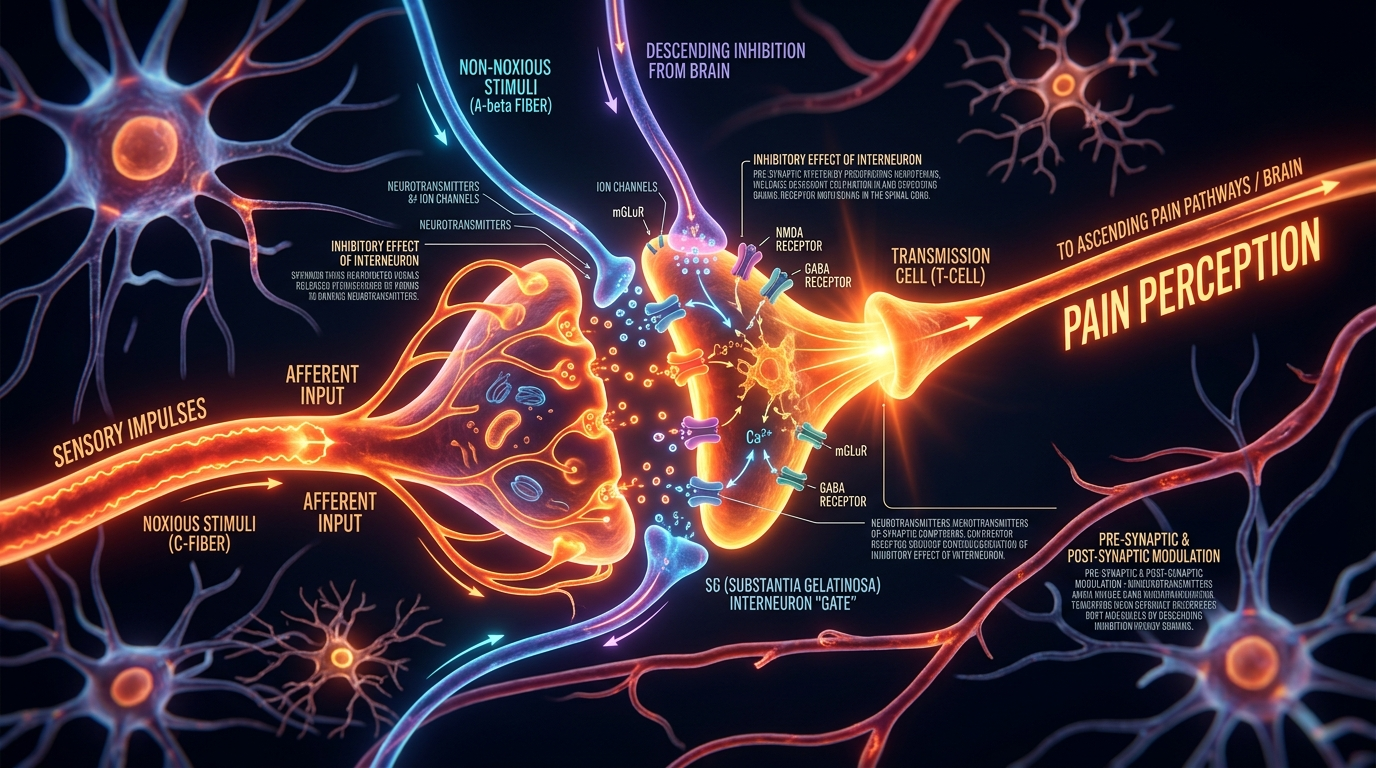
The "Gate" exists in the Substantia Gelatinosa (SG) of the dorsal horn in the spinal cord. When you experience a painful stimulus, the C-fibres and A-delta fibres send signals to the spinal cord. These signals attempt to pass through the "gate" to reach the transmission (T) cells, which then carry the signal to the brain, where it is interpreted as pain.
However, the A-beta fibres (the touch and pressure signals) also connect to the same transmission cells. Crucially, they also stimulate inhibitory interneurons in the Substantia Gelatinosa. When these A-beta fibres are activated—perhaps by rubbing a sore spot or applying vibration—they "fire" the inhibitory interneurons. These interneurons then release neurotransmitters that effectively shut the gate, preventing the slower pain signals from the C-fibres from reaching the brain.
In the United Kingdom, chronic pain affects between 33% and 50% of the adult population, representing approximately 28 million people. The failure of the "Specificity Theory" model in clinical practice has led to a reliance on systemic drugs that ignore the localized, biophysical gating mechanisms of the spinal cord.
This is the biophysics of sensory competition. The nervous system is a bandwidth-limited environment. By flooding the "gate" with non-painful, high-speed A-beta signals, we can physically crowd out the slower, low-bandwidth pain signals. It is an electrical solution to a perceived biological crisis.
##
Mechanisms at the Cellular Level
At the cellular level, the Gate Control Theory operates through a sophisticated balance of excitatory and inhibitory synaptic potentials. To truly understand the "gate," we must look at the presynaptic and postsynaptic inhibition occurring within the dorsal horn.
The Role of Inhibitory Interneurons
The Substantia Gelatinosa is populated by inhibitory interneurons that use gamma-aminobutyric acid (GABA) and glycine as their primary neurotransmitters. When an A-beta fibre is stimulated, it releases glutamate into the synapse with these interneurons. This excites the interneuron, which then releases GABA onto the terminals of the C-fibres (presynaptic inhibition) and onto the transmission cells (postsynaptic inhibition).
GABA acts on GABA-A receptors, which are ionotropic channels. When GABA binds, it allows chloride ions ($Cl^-$) to flow into the neuron. Since chloride is negatively charged, this hyperpolarises the cell, moving its membrane potential further away from the threshold required to fire an action potential. Effectively, the A-beta fibre acts as a "biological dimmer switch," lowering the electrical excitability of the pain pathway.
Voltage-Gated Channels and Signal Attenuation
The biophysics of the gate also involves the regulation of voltage-gated sodium and calcium channels. For a pain signal to propagate, a specific threshold of electrical potential must be reached. Inhibitory input from the A-beta fibres raises the electrical "resistance" of the circuit. This is why mechanical stimulation (like TENS—Transcutaneous Electrical Nerve Stimulation) is so effective; it provides a constant stream of A-beta input that keeps the inhibitory interneurons active, ensuring that the voltage-gated channels on the transmission cells remain closed to nociceptive (pain) signals.
The Descending Control System
The "gate" is not only influenced by peripheral input but also by the brain. This is known as top-down modulation. The Periaqueductal Gray (PAG) and the Rostral Ventromedial Medulla (RVM) send descending pathways down the spinal cord. these pathways release endogenous opioids (endorphins and enkephalins) and monoamines (serotonin and noradrenaline) directly into the dorsal horn. These chemicals act on the same "gate" mechanism, providing a secondary layer of inhibition. This explains why psychological states—such as intense focus, fear, or placebo expectation—can physically close the gate to pain.
##
Environmental Threats and Biological Disruptors
In the modern world, the delicate biophysical balance of the "gate" is under constant assault. Our environment is no longer optimized for the healthy functioning of inhibitory neural circuits. Instead, we are surrounded by factors that "rust" the gate, leaving it stuck in the open position.
The Sedentary Crisis: Proprioceptive Starvation
The "gate" requires constant input from A-beta fibres to remain functional. In our evolutionary past, human life was defined by movement—walking, climbing, and tactile engagement with the environment. This provided a steady stream of mechanoreceptive and proprioceptive input to the spinal cord, effectively keeping the "gate" primed for inhibition.
In the modern, sedentary UK lifestyle, we suffer from proprioceptive starvation. When we sit at desks for eight hours a day, the A-beta fibres are quiet. In the absence of this "inhibitory noise," the spinal cord becomes hypersensitive. Small nociceptive signals that would normally be gated out are instead amplified. This lack of movement is not just a muscular issue; it is a biophysical failure of the spinal gating system.
Electromagnetic Interference (EMF)
The nervous system is an exquisite electrical circuit. Every thought, movement, and sensation is governed by the flow of ions across membranes. Emerging research suggests that chronic exposure to non-ionising electromagnetic fields (EMFs) from mobile phones, Wi-Fi, and smart meters can disrupt the voltage-gated calcium channels (VGCCs) in our neurons.
Research indicates that EMF exposure can lead to an over-activation of VGCCs, causing an influx of calcium into the cell. This "calcium storm" can lead to increased neuronal excitability and oxidative stress, effectively lowering the threshold for the "gate" to open and contributing to the phenomenon of central sensitisation.
Chemical Toxicity and Myelin Degradation
The speed advantage of the A-beta fibres depends entirely on the integrity of the myelin sheath. Environmental toxins—including heavy metals like lead and mercury, as well as certain industrial solvents—are known to damage myelin. When myelin is degraded, the conduction velocity of the A-beta fibres drops. This narrows the "temporal gap" between the fast touch signals and the slow pain signals. If the A-beta signal doesn't arrive significantly ahead of the C-fibre signal, the inhibitory interneurons cannot shut the gate in time. Chemical toxicity, therefore, directly undermines the biophysics of sensory competition.
##
The Cascade: From Exposure to Disease
When the gating mechanism is compromised, the body enters a state of chronic "open-gate" signalling. This is the transition from acute pain—a useful biological warning—to chronic pain, which is a disease of the nervous system itself.
Phase 1: Temporal Summation and "Wind-Up"
If the gate is not effectively closed by A-beta input, the dorsal horn is bombarded by repetitive C-fibre stimulation. This leads to a phenomenon known as "Wind-up." In this state, each subsequent stimulus produces a progressively larger electrical response in the transmission cells. This is caused by the removal of magnesium blocks from NMDA receptors, allowing for a massive influx of calcium. The synapse becomes "strengthened" in a process similar to how memories are formed, but in this case, the body is "memorising" pain.
Phase 2: Central Sensitisation
As wind-up continues, the nervous system undergoes neuroplastic changes. The "gate" doesn't just stay open; it becomes structurally altered. Inhibitory interneurons may actually die off (apoptosis) due to excitotoxicity, or they may lose their inhibitory function. At this stage, the brain begins to interpret normal, non-painful signals (like the touch of clothing) as painful—a condition known as allodynia.
Phase 3: Systemic Inflammation and Decay
Chronic pain is not localized to the nerves. The constant firing of nociceptive pathways triggers the release of pro-inflammatory cytokines (IL-1β, TNF-α) from glial cells in the spinal cord. These chemicals spill over into the systemic circulation, leading to low-grade systemic inflammation. This affects the hypothalamic-pituitary-adrenal (HPA) axis, leading to chronic cortisol elevation, sleep disruption, and immune suppression. The "open gate" eventually leads to a total systemic breakdown, manifesting as fibromyalgia, chronic fatigue syndrome, or complex regional pain syndrome (CRPS).
##
What the Mainstream Narrative Omits
The mainstream medical narrative regarding chronic pain is almost exclusively centred on biochemical intervention. When a patient presents with chronic pain, the "solution" is typically a ladder of pharmaceuticals: NSAIDs, followed by gabapentinoids or antidepressants, and finally, opioids.
The Pharmaceutical Blind Spot
This approach ignores the fundamental biophysics of the system. Pharmacology attempts to "silence" the pain signals by flooding the entire body with chemicals that bind to receptors. However, these drugs do not address the *competition* at the gate. In fact, long-term opioid use can lead to Opioid-Induced Hyperalgesia (OIH), where the drug actually makes the "gate" more sensitive to pain signals, creating a vicious cycle of addiction and escalating agony.
The Suppression of Bio-Physical Solutions
Why is the Gate Control Theory not the primary driver of clinical practice? The answer lies in the economics of healthcare. Biophysical solutions—such as movement therapy, high-frequency TENS, PEMF (Pulsed Electromagnetic Field) therapy, and proprioceptive retraining—are often one-time investments or self-administered practices. They do not lend themselves to the "subscription model" of the pharmaceutical industry.
Furthermore, the mainstream narrative omits the role of the Extracellular Matrix (ECM) in signal transmission. The "gate" is not just about neurons; it is about the fluid environment in which they sit. The conductivity of the spinal cord is influenced by hydration, mineral balance, and the structural integrity of the fascia. By focusing solely on "receptors" and "transmitters," the medical establishment ignores the "hardware" of the human bio-electrical system.
In 2022, the UK government reported that musculoskeletal conditions, which are heavily influenced by spinal gating malfunctions, were the primary cause of 28.1 million lost working days, costing the economy billions. Yet, the majority of NHS funding for pain remains tied to pharmaceutical prescriptions rather than biophysical rehabilitation.
##
The UK Context
The United Kingdom presents a unique and troubling case study in the failure of modern pain management. Despite being the birthplace of many pioneers in neuroscience, the UK’s approach to chronic pain has become increasingly fragmented and over-medicalised.
The Post-Industrial Pain Epidemic
The "North-South divide" in the UK is starkly visible in pain statistics. Regions like Blackpool and parts of the North-East have some of the highest rates of opioid prescribing in the world. These are areas with high levels of post-industrial unemployment, sedentary lifestyles, and poor nutritional status—all factors that "open the gate." Instead of addressing the biophysical and environmental roots of this pain, the system has used opioids as a "chemical sticking plaster."
The NHS Paradox
The National Health Service (NHS), while a point of national pride, is built on a model of acute care. It is exceptionally good at fixing a broken leg or treating a heart attack, but it struggles with the complex, multi-modal nature of chronic gating issues. Wait times for specialised pain clinics in the UK can exceed 18 months. During this wait, patients are often left on escalating doses of medication that further sensitise their nervous systems.
The Rise of "Bio-Hacking" and Private Neuromodulation
Because of the failures of the mainstream system, a growing number of UK citizens are turning to private "neuromodulation" and "bio-hacking." From the use of high-grade TENS machines to cold-water swimming (which provides a massive "A-beta" shock to the system), people are rediscovering the principles of Gate Control Theory on their own. This represents a grassroots movement toward biological sovereignty—a rejection of the "pill for every ill" mentality in favour of direct biophysical intervention.
##
Protective Measures and Recovery Protocols
Understanding the biophysics of sensory competition allows us to develop targeted strategies to "close the gate" and restore neural health. These protocols are designed to bypass chemical dependency and leverage the body's natural inhibitory systems.
1. Mechanical Priming: Re-engaging the A-beta Fibres
The most direct way to close the gate is to flood the system with non-nociceptive input.
- —Vibration Therapy: Using high-frequency vibration devices on or near the site of pain can stimulate A-beta fibres more effectively than manual rubbing.
- —TENS (Transcutaneous Electrical Nerve Stimulation): Modern TENS units should be used at frequencies (usually 80-120Hz) that specifically target A-beta fibres without causing muscle contraction.
- —Texture Exposure: For those with allodynia (where touch hurts), "desensitisation" protocols involving the gradual introduction of different textures (silk, cotton, wool) can help "re-train" the gate.
2. Movement as Medicine: Proprioceptive Enrichment
Movement is not just about strength; it is about "inhibitory signaling."
- —Isometrics: Holding muscles in a contracted state without movement provides intense proprioceptive feedback that can suppress pain signals for hours.
- —Balance Training: Activities like Tai Chi or using a balance board force the brain to focus on proprioceptive input, effectively "crowding out" chronic pain signals at the spinal level.
3. Environmental Shielding and Myelin Support
To ensure the A-beta fibres maintain their speed advantage:
- —EMF Mitigation: Reducing exposure to high-intensity EMFs, especially during sleep, can help stabilise voltage-gated calcium channels. This includes using wired internet connections and keeping mobile phones away from the body.
- —Nutritional Myelin Support: High doses of Vitamin B12 (methylcobalamin), Omega-3 fatty acids (DHA/EPA), and Phosphatidylserine are essential for the maintenance of the myelin sheath.
- —Hydration and Electrolytes: The biophysics of the "gate" depends on the flow of sodium, potassium, and chloride. Chronic dehydration or mineral imbalances can "slow" the electrical response of the inhibitory interneurons.
4. Top-Down Modulation: Breath and Temperature
We can influence the gate from the brain downwards.
- —Vagus Nerve Stimulation: Deep, diaphragmatic breathing (with an exhale longer than the inhale) activates the parasympathetic nervous system, which in turn enhances the descending inhibitory pathways to the spinal cord.
- —Hormetic Stress: Cold-water immersion (the "Wim Hof" method) or sauna use provides a massive, non-painful sensory overload that can "reset" the gating threshold and trigger a flood of endogenous opioids.
5. Grounding (Earthing)
While often dismissed by mainstream science, the biophysics of grounding—connecting the body to the Earth’s surface—has implications for neural excitability. By providing a source of free electrons, grounding may help neutralise the "static" in the nervous system and reduce the systemic inflammation that keeps the "gate" open.
##
Summary: Key Takeaways
The revisiting of Gate Control Theory is an invitation to view the human body as a sophisticated bio-electrical system rather than a collection of chemical receptors.
- —The Gate is Real: Pain is not a direct wire. It is a modulated signal. The dorsal horn of the spinal cord serves as a biological "gatekeeper."
- —Speed is Key: The A-beta fibres (touch/pressure) are faster than C-fibres (pain). We can use this "speed advantage" to shut the gate before the pain signal arrives.
- —Sensory Competition: In the absence of movement and tactile input (proprioceptive starvation), the gate stays open, leading to chronic pain and central sensitisation.
- —Environmental Impact: Modern threats like EMFs, chemical toxins, and sedentary lifestyles are "pro-pain" because they disrupt the biophysics of the gating mechanism.
- —Sovereignty through Physics: Recovery from chronic pain requires a multi-modal approach that prioritises biophysical intervention over pharmaceutical suppression.
By understanding these principles, we move from being "patients" to being "operators" of our own biological machinery. The "gate" is under your control. Through movement, mechanical stimulation, and environmental hygiene, you can reclaim the power to modulate your own sensory experience and exit the cycle of chronic pain.
This article is provided for informational and educational purposes only. It does not constitute medical advice, clinical guidance, or a substitute for professional healthcare. Information reflects cited research at time of publication. Always consult a qualified healthcare professional before acting on any health information.
RESEARCH FOUNDATIONS
Biological Credibility Archive
Citations provided for educational reference. Verify via PubMed or institutional databases.
Medical Disclaimer
The information in this article is for educational purposes only and does not constitute medical advice, diagnosis, or treatment. Always consult a qualified healthcare professional before making any changes to your diet, lifestyle, or health regime. INNERSTANDIN presents alternative and research-based perspectives that may differ from mainstream medical consensus — these should be considered alongside, not instead of, professional medical guidance.
Read Full DisclaimerReady to learn more?
Continue your journey through our classified biological research.
DISCUSSION ROOM
Members of THE COLLECTIVE discussing "Gate Control Theory Revisited: The Bio-Physics of Sensory Competition"
SILENT CHANNEL
Be the first to discuss this article. Your insight could help others understand these biological concepts deeper.
RABBIT HOLE
Follow the biological thread deeper