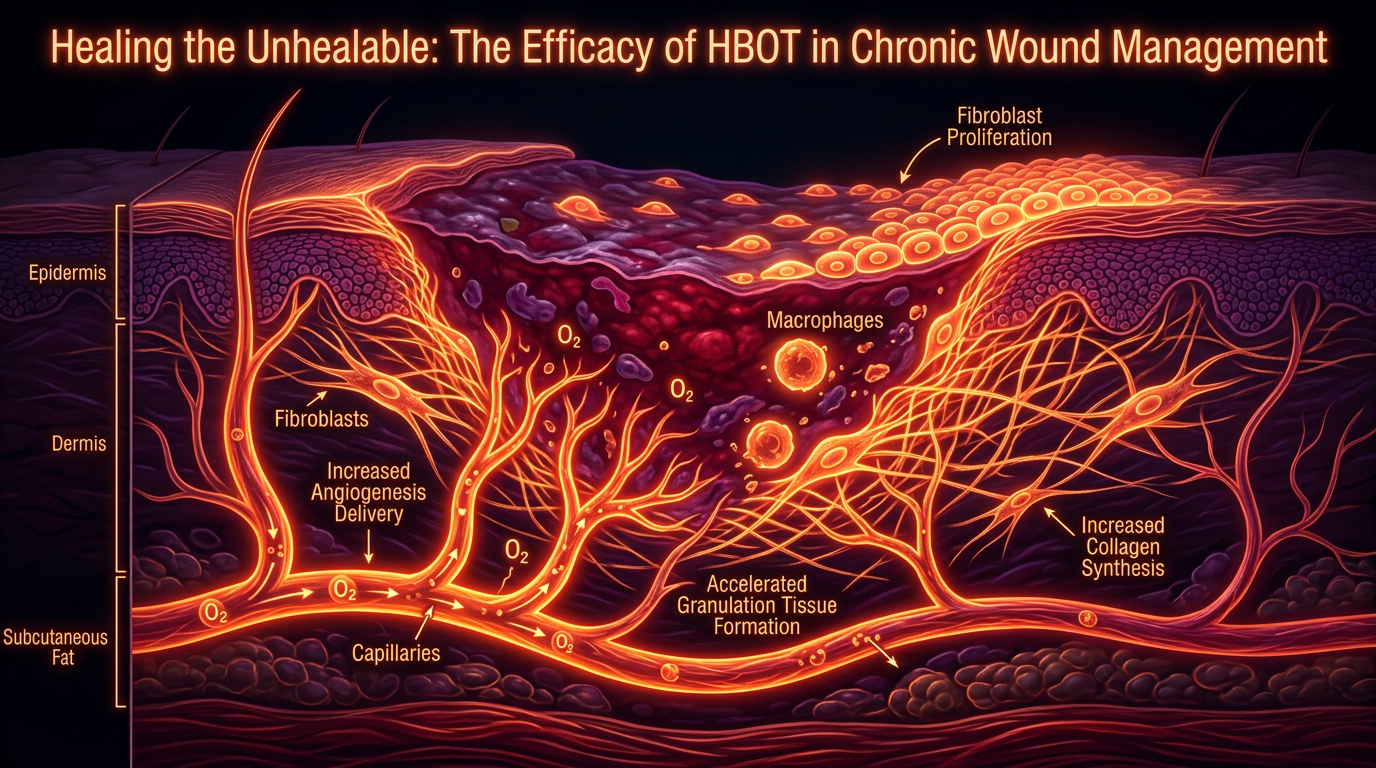
Healing the Unhealable: The Efficacy of HBOT in Chronic Wound Management
A deep dive into how hyperbaric oxygen therapy provides a lifeline for patients suffering from diabetic foot ulcers and non-healing radiation injuries.
# Healing the Unhealable: The Efficacy of HBOT in Chronic Wound Management
The modern medical landscape is currently besieged by a silent epidemic: the chronic, non-healing wound. In the United Kingdom alone, the burden of wound management has reached a critical inflection point, exhausting NHS resources and leaving millions in a state of prolonged morbidity. When the body’s innate regenerative intelligence is silenced by systemic dysfunction, traditional topical interventions often fail.
To truly understand the "unhealable" wound, one must look beneath the bandage and into the cellular environment of hypoxia. This research piece explores Hyperbaric Oxygen Therapy (HBOT) not merely as an adjunctive treatment, but as a fundamental physiological catalyst capable of restarting the stalled machinery of human repair.
The Biological Stagnation: Why Wounds Fail
A chronic wound—defined as a lesion that fails to proceed through an orderly and timely series of events to produce functional and structural integrity—is a symptom of biological bankruptcy. At the heart of this failure lies a profound deficiency in cellular energy and a breakdown in intercellular communication.
The Hypoxic Ceiling
All healing is energy-dependent. The synthesis of collagen, the migration of epithelial cells, and the oxidative burst of macrophages (the body’s primary defence against wound pathogens) all require significant amounts of Adenosine Triphosphate (ATP). Oxygen is the final electron acceptor in the mitochondrial respiratory chain; without it, ATP production slows to a crawl.
In chronic wounds, the local microenvironment is severely hypoxic. Peripheral vascular disease, diabetes-induced microangiopathy, and localized oedema create a physical barrier to oxygen delivery. When the partial pressure of oxygen ($pO_2$) drops below 20 mmHg, cell division stops, and the wound enters a state of senescent stasis.
The Biofilm Fortress
Further complicating the biological landscape is the presence of polymicrobial biofilms. These are not merely bacterial colonies but sophisticated, multi-species fortresses that secrete an extracellular polymeric substance (EPS). This shield renders the bacteria up to 1,000 times more resistant to conventional antibiotics and hides them from the host's immune system.
The Mechanism of HBOT: Beyond the Red Blood Cell
The orthodox understanding of oxygen transport is limited to the capacity of haemoglobin. In a healthy individual breathing room air at sea level, haemoglobin is already 97–98% saturated. Increasing oxygen intake under normal atmospheric pressure (1.0 ATA) yields negligible gains in systemic delivery.
Hyperbaric Oxygen Therapy operates on the principles of Henry’s Law, which states that the amount of a gas dissolved in a liquid is proportional to its partial pressure.
Plasma Saturation and the Diffusion Radius
Inside a hyperbaric chamber, typically pressurised between 2.0 and 2.4 ATA, the patient breathes 100% medical-grade oxygen. Under these conditions, oxygen is forced directly into the blood plasma, the cerebrospinal fluid, and the lymph.
- —Plasma Oxygenation: At 3.0 ATA, enough oxygen can be dissolved in the plasma to support life even in the total absence of red blood cells.
- —Enhanced Diffusion: Because the concentration gradient is so steep, oxygen can diffuse four times further from the capillary into the surrounding tissue than it could under normal conditions. This bypasses the "no-man's land" of necrotic tissue and reaches the ischaemic core of the wound.
The Hyperoxic-Hypoxic Paradox
One of the most profound "truths" exposed by recent research is that HBOT does not just work by providing oxygen; it works by triggering a genetic response to the *fluctuation* of oxygen. By rapidly increasing oxygen levels and then returning to normoxia, the body perceives a "relative" hypoxia. This triggers the activation of Hypoxia-Inducible Factors (HIF-1α), which in turn stimulates:
- —Angiogenesis: The formation of new blood vessels via Vascular Endothelial Growth Factor (VEGF).
- —Stem Cell Mobilisation: Research indicates that a single course of HBOT can increase the concentration of circulating CD34+ haematopoietic stem cells by eight-fold, effectively "recruiting" the body’s repair kit from the bone marrow.
"The cost of managing wounds in the UK is estimated at £8.3 billion annually. Of this, the management of non-healing wounds accounts for 67% of the total expenditure, with the NHS performing over 7,000 lower limb amputations per year—many of which are preventable through advanced oxygen protocols." — *Source: NHS England Wound Care Strategy Programme.*
Environmental Disruptors: The Modern Obstacles to Repair
We must address why the modern body is increasingly incapable of self-repair. While HBOT provides the fuel, environmental toxins often act as the "brakes" on recovery.
Glyphosate and Collagen Synthesis
The widespread use of glyphosate-based herbicides in the UK food chain has a direct impact on wound integrity. Glyphosate acts as a glycine analogue. During collagen synthesis—the primary structural protein of a wound—the body may mistakenly incorporate glyphosate instead of glycine. This leads to "junk proteins" that lack structural stability, resulting in wounds that easily re-open or never fully close.
Electromagnetic Interference (EMI)
Emerging data suggest that the heavy saturation of non-ionising radiation (from 5G infrastructure and Wi-Fi) can disrupt the voltage-gated calcium channels (VGCCs) in the cellular membrane. This leads to calcium flooding, oxidative stress, and a disruption of the bioelectrical signals that guide cells toward the site of an injury (galvanotaxis). HBOT helps counteract this by reinforcing the antioxidant defence system, specifically increasing levels of Superoxide Dismutase (SOD).
The Micronutrient Gap
The efficacy of HBOT is intrinsically linked to the availability of co-factors. A body depleted of Vitamin C, Zinc, and Copper cannot build a basement membrane, regardless of how much oxygen is present. Modern soil depletion in the British Isles means that "standard" diets are often insufficient for the metabolic demands of hyperbaric-induced repair.
- —Mitochondrial Dysfunction: Microplastics and heavy metals (such as aluminium and mercury) can lodge within mitochondrial membranes, uncoupling the electron transport chain and rendering oxygen therapy less effective.
- —Chronic Inflammation: High-linoleic acid seed oils contribute to a pro-inflammatory prostaglandin profile (PGE2), which keeps the wound in the inflammatory phase and prevents it from transitioning to the proliferative phase.
The Truth Exposed: Why is HBOT Underutilised?
If the evidence for HBOT in treating diabetic foot ulcers, gas gangrene, and crushing injuries is so robust, why is it not a frontline treatment in every NHS trust?
The answer lies in the divergence between Acute Care Economics and Regenerative Science. HBOT is a capital-intensive therapy. A multi-place chamber requires significant floor space, specialised staffing, and rigorous safety protocols. In a "pills-and-dressings" medical model, the high upfront cost of a 40-session HBOT protocol is often viewed as prohibitive, despite the fact that it prevents the astronomical cost of an amputation and the subsequent lifelong care required.
Furthermore, oxygen is a non-patentable element. There is no pharmaceutical incentive to fund the massive, multi-centre double-blind trials required to change "Standard of Care" guidelines at a bureaucratic level. Consequently, HBOT remains relegated to a "last resort" status, used only when the limb is already at the brink of loss.
Recovery Protocols: The INNERSTANDING Approach
For HBOT to be effective in "healing the unhealable," it must be applied with precision. A scattergun approach is insufficient for the complex, chronic patient.
The Saturation Phase
For chronic wounds (particularly diabetic foot ulcers or Wagner Grade 3 lesions), the protocol typically demands high frequency.
- —Pressure: 2.0 to 2.4 ATA.
- —Duration: 90 minutes of 100% oxygen (with "air breaks" every 20-30 minutes to prevent oxygen toxicity).
- —Frequency: 5 days per week.
- —Quantity: 20 sessions for initial vascular signalling; 40–60 sessions for full tissue remodelling.
Synergistic Integration
To optimise the HBOT environment, the following must be addressed concurrently:
- —Debridement: The removal of necrotic tissue and biofilm must occur alongside HBOT to allow the oxygenated plasma to reach viable tissue.
- —Nutritional Loading: High-dose Liposomal Vitamin C, Zinc Picolinate, and Magnesium Bisglycinate should be administered to provide the "bricks" for the oxygen "engine."
- —Grounding and Shielding: Patients are encouraged to reduce EMF exposure during the recovery period to allow the body's bio-electric field to stabilise.
"In the UK, diabetic patients are 23 times more likely to undergo a leg, foot, or toe amputation than those without the condition. Statistics from Public Health England reveal that there are over 170,000 active diabetic foot ulcers at any given time, yet fewer than 5% of these patients ever receive access to Hyperbaric Oxygen Therapy."
The Future of Wound Management
We are moving toward a period of "Biological Realignment." The "unhealable" wound is a misnomer; it is simply a wound that has been denied the requisite environment for repair. By harnessing the laws of physics to overcome the limitations of biology, HBOT offers a bridge back to homeostasis.
The evidence is clear: when we saturate the body with the very element that fuels life, under the necessary pressure to bypass systemic blockages, the "impossible" becomes inevitable. The challenge remains not in the science, but in the implementation—moving HBOT from the fringes of "alternative" medicine into its rightful place at the core of regenerative practice.
Key Summary of Benefits:
- —Immediate Reversal of Hypoxia: Provides life-saving oxygen to tissue that is physically cut off from the blood supply.
- —Bactericidal and Bacteriostatic Effects: Directly kills anaerobic bacteria and enhances the effectiveness of white blood cells and antibiotics.
- —Cytokine Modulation: Reduces pro-inflammatory cytokines (IL-1, IL-6, TNF-alpha) while increasing growth factors.
- —Stem Cell Proliferation: Forces the body to release its own regenerative cells into the bloodstream.
- —Oedema Reduction: High pressure causes vasoconstriction in healthy tissue while maintaining oxygenation, which helps "squeeze" excess fluid out of the wound site, improving local circulation.
Conclusion
Hyperbaric Oxygen Therapy is the ultimate "truth-exposing" modality. It exposes the fallacy that the body is a fragile machine destined for decay. Instead, it reveals the body as a self-correcting system that simply requires the correct inputs—pressure, purity, and oxygen—to overcome the environmental and physiological insults of the modern age. For the thousands in the UK facing the trauma of chronic wounds and potential amputation, HBOT is not just a therapy; it is an essential reclamation of biological sovereignty.
This article is provided for informational and educational purposes only. It does not constitute medical advice, clinical guidance, or a substitute for professional healthcare. Information reflects cited research at time of publication. Always consult a qualified healthcare professional before acting on any health information.
RESEARCH FOUNDATIONS
Biological Credibility Archive
Citations provided for educational reference. Verify via PubMed or institutional databases.
Medical Disclaimer
The information in this article is for educational purposes only and does not constitute medical advice, diagnosis, or treatment. Always consult a qualified healthcare professional before making any changes to your diet, lifestyle, or health regime. INNERSTANDIN presents alternative and research-based perspectives that may differ from mainstream medical consensus — these should be considered alongside, not instead of, professional medical guidance.
Read Full DisclaimerReady to learn more?
Continue your journey through our classified biological research.
DISCUSSION ROOM
Members of THE COLLECTIVE discussing "Healing the Unhealable: The Efficacy of HBOT in Chronic Wound Management"
SILENT CHANNEL
Be the first to discuss this article. Your insight could help others understand these biological concepts deeper.
RABBIT HOLE
Follow the biological thread deeper