Hydrogen Sulfide SIBO: The Biology of the Third Gas
Unlike methane or hydrogen, hydrogen sulfide overgrowth is characterized by distinct systemic symptoms like brain fog and sulfur-smelling gas. This variant requires a specific nutritional and antimicrobial approach to resolve.
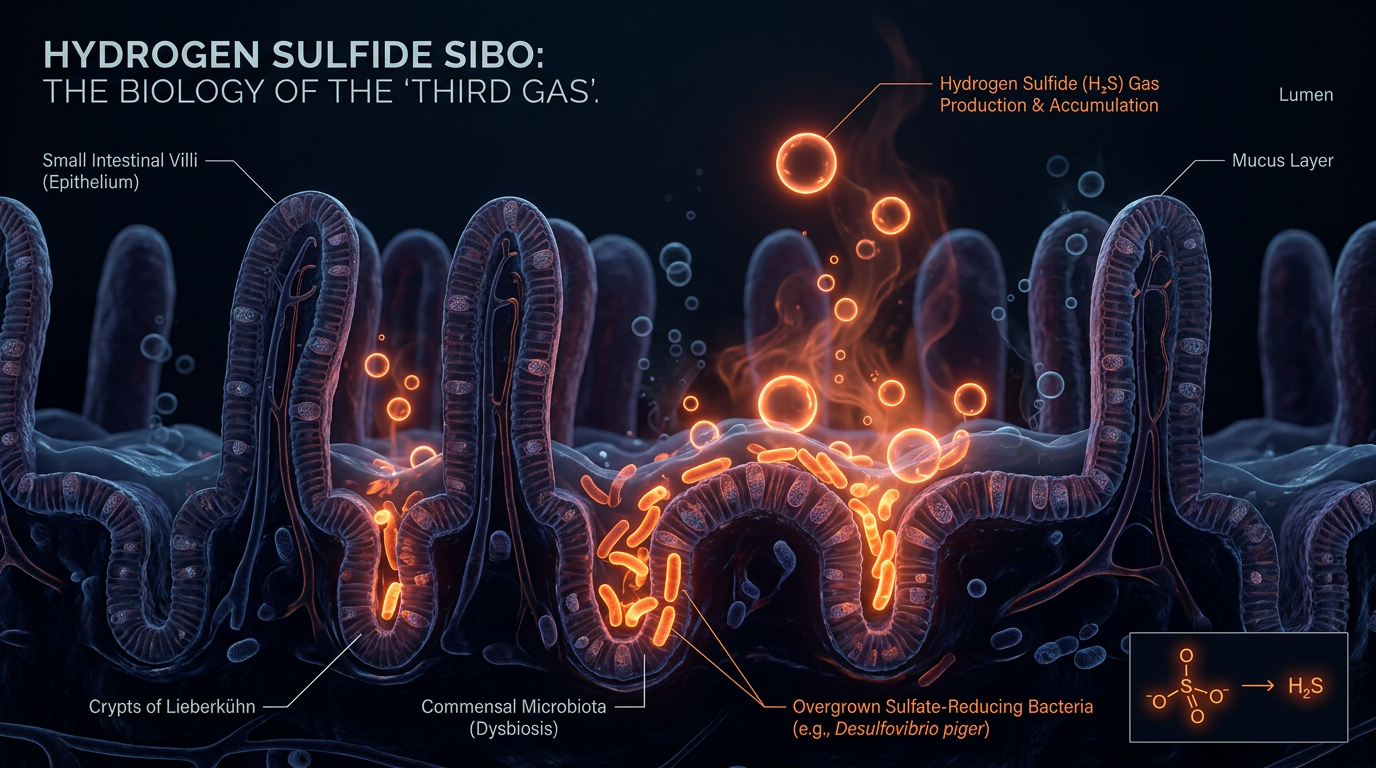
# Hydrogen Sulfide SIBO: The Biology of the Third Gas
Overview
The landscape of gastroenterology is undergoing a radical shift, one that moves beyond the simplistic "fibre and probiotics" paradigm toward a granular understanding of microbial metabolism. For decades, Small Intestinal Bacterial Overgrowth (SIBO) was diagnosed via breath tests that measured only two gases: hydrogen and methane. This left a vast cohort of patients—those presenting with the classic "rotten egg" flatulence, profound neurological fatigue, and systemic hypersensitivity—in a diagnostic vacuum. These patients were often dismissed as having "atypical" IBS or psychogenic disorders. We now know that they were suffering from the overproduction of Hydrogen Sulfide (H2S), the "Third Gas."
Hydrogen sulfide is a Janus-faced molecule. In physiological amounts, it acts as a critical gasotransmitter, regulating vascular tone, cellular signaling, and cytoprotection. However, when the microbial ecosystem of the small intestine shifts toward an overrepresentation of sulfate-reducing bacteria (SRB), H2S becomes a potent metabolic poison. Unlike hydrogen (which is inert) or methane (which primarily slows motility), H2S is chemically reactive and highly diffusible. It does not merely stay in the gut; it translocates, entering the bloodstream and inhibiting the very machinery of cellular respiration.
This article serves as an exhaustive investigation into the biological underpinnings of Hydrogen Sulfide SIBO. We will dissect how certain microbes hijack the sulfur cycle, why modern environmental factors have primed the British population for this specific dysbiosis, and why the standard SIBO treatment protocols often exacerbate the condition. This is not merely a digestive issue; it is a systemic mitochondrial crisis initiated in the lumen of the small bowel.
##
The Biology — How It Works
To understand H2S SIBO, one must first understand the sulfur cycle within the human body. Sulfur is the third most abundant mineral in the body, essential for the synthesis of glutathione (our master antioxidant), the formation of connective tissue, and the detoxification pathways of the liver. We obtain sulfur primarily through protein (amino acids like methionine and cysteine) and inorganic sulfates found in water and cruciferous vegetables.
In a healthy state, the majority of sulfur is absorbed in the upper gastrointestinal tract or utilised by the host. However, in H2S SIBO, a specific class of microbes known as Sulfate-Reducing Bacteria (SRB) proliferates in the small intestine—an area that should be relatively sparsely populated. The primary culprits are species such as *Desulfovibrio piger*, *Desulfovibrio fairfieldensis*, and *Bilophila wadsworthia*. These organisms do not ferment carbohydrates in the way *E. coli* or *Klebsiella* do. Instead, they perform dissimilatory sulfate reduction.
These bacteria use hydrogen (produced by other fermenting bacteria) as an electron donor to reduce sulfate into hydrogen sulfide gas. This creates a competitive ecological niche. If you have a high population of SRB, they effectively "mop up" the hydrogen produced by other microbes to fuel their own H2S production. This explains why many patients return "flatline" results on traditional breath tests; the hydrogen is being produced, but it is immediately consumed by SRB to create H2S, which, until recently, was not measured by standard clinical equipment.
The presence of *Bilophila wadsworthia* is particularly concerning. This organism thrives in the presence of bile. High-fat diets, particularly those high in saturated animal fats, trigger an increase in taurine-conjugated bile acids. *B. wadsworthia* can deconjugate these bile acids to release sulfur, providing itself with an endless fuel source. This creates a vicious cycle where the body’s own digestive secretions are repurposed to feed a pathobiont that generates a neurotoxic byproduct.
##
Mechanisms at the Cellular Level
The pathogenicity of H2S SIBO lies in the molecule’s affinity for metal-containing enzymes. At the heart of every human cell lies the mitochondria, responsible for generating ATP (energy) through the electron transport chain. Hydrogen sulfide is a known inhibitor of Cytochrome c oxidase (Complex IV), the final enzyme in the mitochondrial respiratory chain. In this regard, excess H2S functions similarly to cyanide or carbon monoxide, albeit at a lower, chronic dosage.
When H2S levels rise systemically, the patient enters a state of "metabolic hypoxia." Oxygen is available in the blood, but the cells cannot effectively use it to produce energy. This is the biological reality behind the "brain fog" and "heavy limb" fatigue reported by sufferers. The brain, being the most metabolically active organ, is the first to feel this deficit, leading to cognitive impairment, memory lapses, and "neuro-inflammation."
Furthermore, H2S has a profound effect on the intestinal barrier. The gut is lined with a protective mucus layer made of mucins, which are heavily cross-linked by disulfide bonds. These bonds are essential for the structural integrity of the mucus. Excess hydrogen sulfide can break these disulfide bonds, effectively "liquefying" the protective mucus layer. This exposes the underlying epithelial cells to toxins, undigested food particles, and lipopolysaccharides (LPS), leading to hyper-permeability, or "Leaky Gut."
UK FACT: Chronic fatigue syndromes and undiagnosed gut disorders cost the UK economy an estimated £3.3 billion annually in lost productivity. A significant portion of these "mystery" cases likely stem from unaddressed H2S-mediated mitochondrial dysfunction.
At the level of the enteric nervous system, H2S is a potent vasodilator and muscle relaxant. While methane causes constipation by slowing transit, H2S often (though not always) accelerates it, leading to urgency and diarrhoea. However, its most insidious effect is on the visceral nerves, where it lowers the pain threshold, resulting in the "exquisite" bloating and hypersensitivity characteristic of the condition.
##
Environmental Threats and Biological Disruptors
Why are we seeing a surge in H2S SIBO now? The answer lies in the confluence of modern agricultural practices and the degradation of our detoxification enzymes. The enzyme Sulfite Oxidase (SUOX) is responsible for converting toxic sulfite into usable sulfate. This enzyme requires molybdenum as a cofactor. Due to intensive farming practices in the UK and Western Europe, soil molybdenum levels have been depleted, leading to a population that is subclinically deficient in this crucial trace mineral. Without enough molybdenum, the body cannot "clear" the sulfur intermediates, allowing them to accumulate and feed the SRB.
Another significant disruptor is the widespread use of glyphosate (Roundup). While the mainstream narrative suggests glyphosate is safe for humans because we lack the shikimate pathway, this ignores our microbiome. Glyphosate preferentially kills beneficial, "good" bacteria like *Lactobacillus* and *Bifidobacterium*, while many sulfate-reducing bacteria are resistant to it. Furthermore, glyphosate interferes with the body's ability to produce heme, which is a core component of the Cytochrome c oxidase enzyme mentioned earlier. This creates a "double hit": the environment promotes the overgrowth of H2S-producing bacteria while simultaneously weakening the host's ability to resist the toxic effects of the gas.
We must also consider the role of heavy metals. Lead, mercury, and arsenic have a high affinity for sulfur groups. When the body is burdened by heavy metals, it often "sequesters" sulfur to buffer these toxins. This alters the internal sulfur pull, creating a metabolic environment where inorganic sulfur is more available in the intestinal lumen, providing a feast for *Desulfovibrio*.
##
The Cascade: From Exposure to Disease
The progression of H2S SIBO is rarely confined to the gut. It typically follows a predictable "cascade" that begins with a trigger—often a bout of food poisoning (Post-Infectious SIBO), a period of high stress, or a course of broad-spectrum antibiotics—and ends in systemic multi-organ dysfunction.
- —The Colonisation Phase: The initial trigger disrupts the migrating motor complex (MMC), the "inter-digestive housekeeper" of the small intestine. Stagnation occurs, allowing bacteria from the large intestine to migrate upward.
- —The Sulfur Shift: If the individual’s diet is high in sulfur (common in health-conscious circles consuming large amounts of kale, broccoli, and whey protein) or if they have genetic predispositions (like CBS or SUOX mutations), the SRB find a foothold.
- —The Mucosal Breach: H2S begins to degrade the mucus lining. Secretory IgA (the gut’s first-line immune defence) drops. The "gates" of the gut open.
- —Systemic Diffusion: H2S gas and LPS enter the portal vein. The liver is overwhelmed. H2S enters systemic circulation, crossing the blood-brain barrier.
- —The Mast Cell Response: This is a crucial and often overlooked step. Excess H2S is a potent trigger for Mast Cell Activation Syndrome (MCAS). Mast cells, located near nerves and blood vessels, degranulate in response to the perceived threat of H2S, releasing histamine, leukotrienes, and pro-inflammatory cytokines.
This cascade explains why a patient with H2S SIBO doesn't just have a stomach ache; they have "histamine intolerance," "POTS" (Postural Orthostatic Tachycardia Syndrome), skin rashes, and severe anxiety. The "Third Gas" acts as the master key that unlocks a door to a wide array of seemingly unrelated systemic illnesses.
##
What the Mainstream Narrative Omits
The current medical approach to IBS and SIBO is fundamentally reductive. In the UK, the standard NHS pathway for a patient with these symptoms usually involves a Celiac test, a calprotectin stool test (to rule out IBD), and perhaps a basic breath test if the CCG (Clinical Commissioning Group) funds it. When these return negative, the patient is told they have "IBS" and is prescribed an SSRI or a low-FODMAP diet.
This narrative is dangerously incomplete for several reasons:
- —The Methane/Hydrogen Bias: Most labs only measure H2 and CH4. A patient with 0 ppm of hydrogen and 0 ppm of methane is told they are "clear," when in reality, they have a massive H2S overgrowth that is consuming all the hydrogen. This "flatline" result is a clinical red flag for H2S, yet it is interpreted as "normal."
- —The Low-FODMAP Fallacy: The low-FODMAP diet is the gold standard for IBS. However, many "low-FODMAP" foods are high in sulfur (e.g., eggs, beef, kale, cabbage). A patient who diligently follows the low-FODMAP diet may actually be feeding their H2S SIBO, leading to a paradoxical worsening of symptoms.
- —The Antibiotic Error: Rifaximin is the primary antibiotic for SIBO. While effective for hydrogen-dominant cases, it often fails in H2S cases because it does not target *Desulfovibrio* or *Bilophila* effectively. Without adding a "biofilm buster" or a bismuth-based compound, the bacteria remain protected in their sulfur-rich niches.
- —The Genetic Component: Mainstream gastroenterology almost entirely ignores the role of the CBS (Cystathionine Beta-Synthase) gene. Individuals with "upregulated" CBS genes process sulfur into the transsulfuration pathway too quickly, leading to an internal surplus of sulfites and ammonia, which further fuels the growth of H2S bacteria.
ALARMING REALITY: It takes an average of 6.5 years and visits to 5 different specialists before a SIBO patient receives an accurate diagnosis in the UK. During this time, the systemic damage from H2S-induced mitochondrial inhibition can become chronic.
##
The UK Context
The United Kingdom presents a unique set of challenges regarding H2S SIBO. Firstly, the "Great British Diet" has undergone a massive shift. We have moved from traditional, diverse seasonal eating to a diet that is either heavily processed or, among the "health-conscious," obsessively focused on a narrow range of "superfoods" like kale, cauliflower, and eggs—all high-sulfur triggers.
Secondly, the UK's water supply in certain regions is high in inorganic sulfates. For an individual with an already compromised microbiome, drinking two litres of "hard" tap water daily can provide the exact substrate needed for *Desulfovibrio* to flourish.
There is also the issue of the NHS backlog. Post-pandemic, the waiting times for gastroenterology consultations have skyrocketed. This has led to a rise in "self-treating," where patients buy probiotics off the shelf. Most commercial probiotics contain *Lactobacillus* or *Bifidobacterium* strains that can actually produce more hydrogen, which in turn feeds the H2S-producing bacteria. Without access to the Trio-Smart breath test (the only test currently capable of measuring all three gases), British patients are essentially flying blind.
Furthermore, the UK's regulatory environment for supplements is different from the US. Certain key tools for H2S management, like specific forms of bismuth or high-dose molybdenum, are harder to source or require more nuanced clinical guidance. This has created a "health gap" where only those who can afford private functional medicine testing and international supplements can find relief.
##
Protective Measures and Recovery Protocols
Resolving H2S SIBO requires a "bottom-up" and "top-down" approach. You cannot simply kill the bacteria; you must change the internal terrain that allowed them to thrive.
1. The Bismuth-Thiol Approach
H2S-producing bacteria live in robust biofilms—slimy protective layers that shield them from the immune system and antibiotics. Bismuth (as found in products like Pepto-Bismol, though specific compounded forms like Bismuth Subnitrate are preferred) has a unique affinity for hydrogen sulfide. It binds to the gas, neutralising it, and simultaneously penetrates the biofilm.
- —Protocol: High-dose bismuth, often combined with "thiol-complexing" agents (like ALA or DMSA under strict supervision), can effectively "starve" and expose the SRB.
2. Dietary Modulation: The Low-Thiol Diet
Unlike the standard SIBO diet, H2S recovery often necessitates a Low-Sulfur/Low-Thiol diet for a period of 4–6 weeks.
- —Eliminate: Garlic, onions, cruciferous vegetables (broccoli, kale, sprouts), eggs, dairy, and high-sulfur meats (beef, pork).
- —Emphasise: Low-sulfur proteins (white fish, chicken breast), squash, carrots, white rice, and peeled cucumbers.
- —The Goal: Reduce the "fuel" (sulfur) to a level where the microbial population can be rebalanced.
3. Enzymatic Support
To help the host process sulfur, we must support the SUOX and CBS pathways.
- —Molybdenum: 150mcg to 500mcg daily is critical. This mineral acts as the "key" to the enzyme that turns toxic sulfite into harmless sulfate.
- —B2 (Riboflavin) and B12 (Hydroxocobalamin): These are essential cofactors for the methylation and transsulfuration pathways that manage sulfur load.
- —Magnesium Sulfate (Epsom Salts) Paradox: While H2S patients have too much sulfur in the *gut*, they are often deficient in *systemic* sulfate because it is being "stolen" by bacteria. Transdermal magnesium sulfate can bypass the gut and provide the body with the sulfate it needs for detoxification without feeding the SIBO.
4. Antimicrobial Strategy
Once the biofilm is weakened and the diet is controlled, specific botanicals can be used. Uva Ursi and Silver hydrosol have shown efficacy against *Desulfovibrio* species. High-dose Oregano oil can be effective but must be used with caution as it can further irritate an already "leaky" gut lining.
5. Prokinetic Stimulation
The migrating motor complex must be restarted. Without "flushing" the small intestine, the bacteria will simply regrow. Natural prokinetics such as Ginger root and Artichoke extract, taken on an empty stomach, are essential for long-term remission.
##
Summary: Key Takeaways
Hydrogen Sulfide SIBO represents the next frontier in our understanding of the gut-brain axis. It is a condition where the "Third Gas" acts as a bridge between microbial dysbiosis and systemic mitochondrial failure. The "rotten egg" gas is not merely a social inconvenience; it is a clinical marker of a body losing its ability to manage one of life’s most essential elements: sulfur.
- —Recognition is the first step. If a patient has SIBO symptoms but a "negative" or "flatline" breath test, H2S must be suspected.
- —The mechanism is toxic. H2S inhibits mitochondrial respiration, leading to the profound fatigue and "brain fog" that distinguishes this variant from hydrogen or methane SIBO.
- —Environment matters. Depleted soil minerals (molybdenum) and agricultural chemicals (glyphosate) have created a "perfect storm" for sulfur-reducing bacteria.
- —Standard diets fail. The low-FODMAP diet can worsen H2S SIBO. A targeted low-sulfur approach is often required for the initial phase of healing.
- —The UK faces a crisis. The lack of advanced diagnostic testing within the NHS means thousands are languishing with "IBS" while their cellular health erodes.
For the researcher and the clinician, H2S SIBO is a reminder that the human body is an integrated chemical system. We are not just "what we eat," but what our bacteria do with what we eat. Resolving the "Third Gas" requires more than just an antibiotic; it requires a restoration of the delicate balance between the host, the microbe, and the environment. This is the path to "Innerstanding"—a deep, biological reconciliation that returns the body to its natural state of vitality.
This article is provided for informational and educational purposes only. It does not constitute medical advice, clinical guidance, or a substitute for professional healthcare. Information reflects cited research at time of publication. Always consult a qualified healthcare professional before acting on any health information.
RESEARCH FOUNDATIONS
Biological Credibility Archive
The development of a novel four-gas breath test enables the clinical quantification of hydrogen sulfide, establishing it as a distinct biomarker for SIBO-related diarrhea.
Sulfate-reducing bacteria compete with methanogens for hydrogen substrates, fundamentally altering the metabolic gas profile of the intestinal microbiome.
Elevated breath hydrogen sulfide levels are significantly correlated with specific gastrointestinal symptoms, distinguishing hydrogen sulfide SIBO from hydrogen or methane variants.
The intestinal abundance of sulfur-reducing microbes is directly influenced by dietary sulfur intake, which modulates the production of hydrogen sulfide in the gut lumen.
Hydrogen sulfide acts as a critical gaseous signaling molecule in the gut, where its overproduction can lead to impaired cellular respiration and mitochondrial dysfunction.
Citations provided for educational reference. Verify via PubMed or institutional databases.
Medical Disclaimer
The information in this article is for educational purposes only and does not constitute medical advice, diagnosis, or treatment. Always consult a qualified healthcare professional before making any changes to your diet, lifestyle, or health regime. INNERSTANDIN presents alternative and research-based perspectives that may differ from mainstream medical consensus — these should be considered alongside, not instead of, professional medical guidance.
Read Full DisclaimerReady to learn more?
Continue your journey through our classified biological research.
DISCUSSION ROOM
Members of THE COLLECTIVE discussing "Hydrogen Sulfide SIBO: The Biology of the Third Gas"
SILENT CHANNEL
Be the first to discuss this article. Your insight could help others understand these biological concepts deeper.
THE ARSENAL
Based on SIBO & Small Intestine Health — products curated by our research team for educational relevance and biological support.

Magnesium Blend – The Most Important Mineral

Clean Slate – Detoxes thousands of chemicals,heavy metals, pesticides, allergens, mold spores and fungus

Vegan Essential Amino Acids – Plant-Powered Protein Building
INNERSTANDING may earn a commission on purchases made through these links. All products are selected based on rigorous educational relevance to our biological research.
RABBIT HOLE
Follow the biological thread deeper