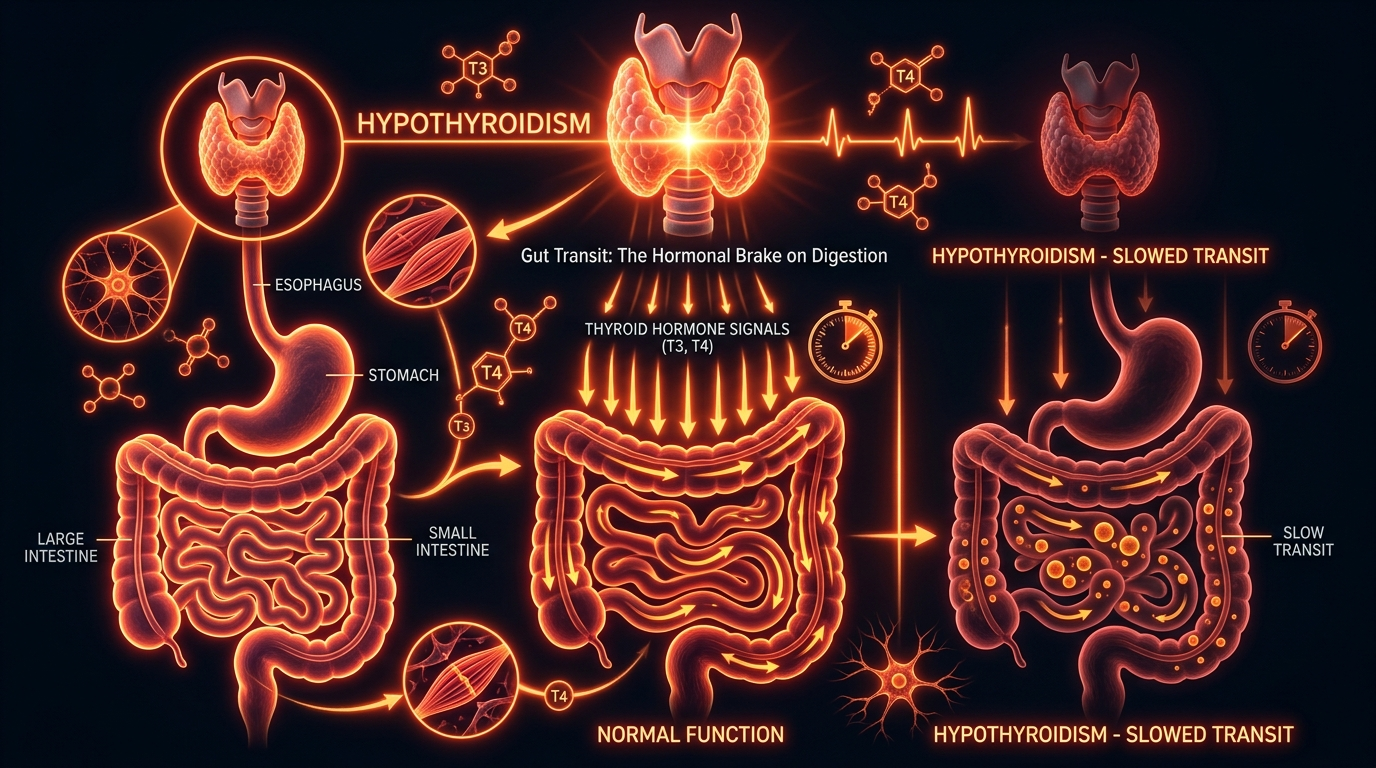
Hypothyroidism and Gut Transit: The Hormonal Brake on Digestion
Thyroid hormones are essential for the metabolic activity of every cell, including the smooth muscles of the gut. Low thyroid function directly translates to slow transit, making SIBO an almost inevitable consequence of untreated hypothyroidism.
Overview
In the intricate architecture of human physiology, no system operates in isolation. However, the prevailing clinical paradigm frequently treats the endocrine system and the gastrointestinal tract as disparate entities, managed by different specialists with little cross-pollination of data. This reductionist approach has led to a silent epidemic: the chronic suppression of digestive motility due to thyroid insufficiency. To understand the gut, one must first understand the metabolic thermostat that governs every cellular action in the body. The thyroid gland, through the secretion of triiodothyronine (T3) and thyroxine (T4), dictates the rate at which life itself proceeds. When this hormonal signal wanes—a state known as hypothyroidism—the body enters a protective, low-energy mode. One of the primary casualties of this metabolic slowdown is the Migrating Motor Complex (MMC), the "housekeeping wave" of the small intestine.
The relationship is not merely influential; it is foundational. Hypothyroidism acts as a hormonal brake on the entire digestive process. When thyroid hormones are suboptimal, the smooth muscles of the gastrointestinal tract lose their contractile vigour, leading to a profound state of stasis. This is not merely an inconvenience of "constipation"; it is a systemic failure that facilitates the overgrowth of pathogenic bacteria, the malabsorption of vital nutrients, and the compromise of the intestinal barrier. For the millions of individuals currently diagnosed with Small Intestinal Bacterial Overgrowth (SIBO) or Irritable Bowel Syndrome (IBS), the missing link is almost invariably an under-functioning thyroid—even when "standard" blood tests suggest otherwise.
In the United Kingdom, Levothyroxine (synthetic T4) is consistently among the top three most prescribed medications, yet over 15% of patients on this monotherapy continue to report unresolved gastrointestinal symptoms, suggesting a failure in both diagnosis and therapeutic application.
This article serves as a comprehensive interrogation of the biochemical axis between the thyroid and the gut. We will explore how metabolic insufficiency creates a permissive environment for SIBO, why environmental toxins in the British landscape are exacerbating this crisis, and why the mainstream medical narrative regarding "normal" thyroid levels is fundamentally flawed.
##
The Biology — How It Works

Energy Blend Supports
Energy Blend is a comprehensive formula designed to fuel your body at a cellular level, promoting sustained physical stamina and mental clarity without synthetic spikes. It targets fundamental metabolic pathways to ensure your nervous system and hormonal activity remain balanced and resilient.
Vetting Notes
Pending
To comprehend why the gut stops moving when the thyroid falters, we must examine the Enteric Nervous System (ENS) and the muscular layers of the alimentary canal. The gastrointestinal tract is a tube of smooth muscle, and muscle contraction is an energetically expensive process. The movement of food, known as peristalsis, and the subsequent cleaning waves of the MMC require a constant supply of adenosine triphosphate (ATP), the body’s primary energy currency.
Thyroid hormones, specifically the active form T3, are the primary regulators of mitochondrial biogenesis and function. Every cell in the ENS possesses receptors for T3. When T3 binds to these receptors, it stimulates the transcription of genes responsible for energy production and muscle fibre activation. In the absence of sufficient T3, the threshold for activation in the smooth muscles of the oesophagus, stomach, and intestines is raised. The result is "delayed gastric emptying" and "slow transit time."
The Migrating Motor Complex is particularly sensitive to thyroid status. The MMC is a distinct pattern of electromechanical activity that occurs in the stomach and small intestine during periods of fasting (usually every 90 to 120 minutes). It acts as a biological broom, sweeping undigested food particles and bacteria down into the colon. Without the "spark" of thyroid hormone, the MMC becomes weak, infrequent, or absent. When this broom stops sweeping, the small intestine—which should be relatively sterile—becomes a stagnant pond. This stagnation is the biological precursor to SIBO.
Furthermore, thyroid hormones influence the production of gastric acid (HCl) in the stomach and bile in the gallbladder. Low thyroid function leads to hypochlorhydria (low stomach acid). Since stomach acid is a primary disinfectant, its absence allows bacteria ingested with food to survive and colonise the upper GI tract. Similarly, T3 is required for the synthesis of bile acids and the contraction of the gallbladder. Hypothyroidism leads to "sludgy" bile and gallstones, further impairing the digestion of fats and the antimicrobial environment of the small intestine.
##
Mechanisms at the Cellular Level
At the sub-cellular level, the impact of hypothyroidism on gut transit is a matter of ion transport and membrane potential. The contraction of smooth muscle cells in the gut depends on the sodium-potassium pump (Na+/K+-ATPase). This pump maintains the electrical gradient across the cell membrane, allowing the cell to "fire" and contract.
"The Role of T3 in Ion Transport:"
T3 directly increases the expression and activity of the Na+/K+-ATPase pump. In a hypothyroid state, the activity of these pumps drops significantly. This leads to a state of cellular "sluggishness" where the smooth muscle cells of the gut become less responsive to the signals from the nervous system. Even if the brain is sending the signal to digest, the muscles lack the electrical potential to respond effectively.
"Mitochondrial Respiration and ATP:"
The gut is one of the most metabolically active organs in the body. The constant turnover of the intestinal lining (every 3–5 days) and the mechanical work of digestion require massive amounts of ATP. Thyroid hormones increase the consumption of oxygen in the mitochondria. When thyroid levels are low, oxygen consumption drops, and ATP production falls. Without ATP, the myenteric plexus—the network of nerves that coordinates gut movement—cannot maintain the rhythm of digestion.
"The Calcium Connection:"
Muscle contraction is also dependent on the flow of calcium ions. Research has shown that thyroid hormones regulate the expression of proteins involved in calcium handling, such as phospholamban and the sarco/endoplasmic reticulum Ca2+-ATPase (SERCA). A deficiency in thyroid hormone disrupts the sequestration of calcium, meaning that even when a muscle does contract, it cannot relax and reset efficiently, leading to "dysmotility"—a chaotic, ineffective movement of the gut wall that fails to propel contents forward.
Key Fact: Studies have demonstrated that patients with clinical hypothyroidism have a transit time that is, on average, 40% slower than euthyroid (normal) individuals, directly correlating with the severity of their T3 deficiency.
##
Environmental Threats and Biological Disruptors
The modern world is increasingly hostile to thyroid health, particularly in the United Kingdom. We are witnessing a confluence of environmental factors that act as biological disruptors, severing the communication between the thyroid and the gut.
The Halogen Displacement Theory
The thyroid gland requires iodine to produce hormones. However, iodine belongs to the halogen group on the periodic table, which also includes fluorine, chlorine, and bromine. These elements possess a similar molecular structure and can compete with iodine for uptake in the thyroid gland.
- —Fluoride: In many parts of the UK, fluoride is added to the public water supply or occurs naturally at high levels. Fluoride is a known goitrogen; it inhibits the thyroid's ability to absorb iodine and can damage the follicular cells of the gland.
- —Bromide: Found in "flour improvers" in many British baked goods (though less common than in the US, it is still present in processed foods and pesticides), bromide is another halogen that displaces iodine, leading to the production of "dud" thyroid hormones that are biologically inactive.
- —Chlorine: Present in tap water and swimming pools, chlorine further contributes to this halogen burden, making it increasingly difficult for the average Briton to maintain sufficient iodine levels for thyroid synthesis.
Glyphosate and the Gut Barrier
The widespread use of glyphosate-based herbicides in UK agriculture has devastating effects on the gut-thyroid axis. Glyphosate interferes with the shikimate pathway in our gut bacteria. While humans don't have this pathway, our beneficial microbes do. By decimating the "good" bacteria, glyphosate allows for the overgrowth of ammonia-producing species, which directly interferes with the conversion of T4 to T3 (which happens largely in the liver and the gut). Furthermore, glyphosate is a potent chelator, stripping the body of minerals like zinc and selenium—both of which are essential co-factors for thyroid hormone production and conversion.
Endocrine Disruptors (EDCs)
The ubiquity of Bisphenol A (BPA) and phthalates in food packaging and personal care products provides a constant "background noise" of oestrogenic signalling. High levels of oestrogen increase Thyroid Binding Globulin (TBG), the protein that carries thyroid hormone through the blood. When TBG is high, the hormones are "locked up" and cannot enter the cells to do their work. This creates a "cellular hypothyroidism" where blood levels might look normal, but the gut tissues are starving for T3.
##
The Cascade: From Exposure to Disease
The progression from environmental exposure to full-blown SIBO and hypothyroidism is a predictable, albeit tragic, cascade. It begins with the suppression of the thyroid gland, but it ends in a self-perpetuating cycle of systemic inflammation.
- —Metabolic Descent: Environmental toxins and chronic stress (which raises cortisol, further inhibiting T4 to T3 conversion) lead to a drop in systemic T3 levels.
- —The Brake is Applied: As T3 drops, the MMC slows down. The transit time of the small intestine increases from the healthy 2-4 hours to 8, 12, or even 24 hours.
- —Bacterial Encroachment: Bacteria from the large intestine (colon) begin to migrate upward into the stagnant small intestine. This is the definition of SIBO.
- —Fermentation and Gas: These bacteria ferment undigested fibres and sugars, producing hydrogen and methane gas. Methane, in particular, has been shown to act as a local neuromuscular inhibitor, further slowing transit. This creates a feedback loop: slow transit causes SIBO, and SIBO (methane) causes even slower transit.
- —Endotoxaemia: The overgrowth of bacteria leads to the production of Lipopolysaccharides (LPS), also known as endotoxins. LPS is a highly inflammatory component of bacterial cell walls. When the gut is stagnant, the intestinal lining becomes "leaky," allowing LPS to enter the bloodstream.
- —The Final Blow to the Thyroid: Systemic LPS triggers the immune system and increases the production of inflammatory cytokines like TNF-alpha and IL-6. These cytokines directly inhibit the deiodinase enzymes (D1 and D2) that convert T4 into the active T3. The body effectively shuts down its own thyroid conversion to "save" energy during an inflammatory crisis.
This is the "Hormonal Brake" in full effect. The patient is now trapped in a cycle where their gut issues are suppressing their thyroid, and their suppressed thyroid is preventing their gut from healing.
##
What the Mainstream Narrative Omits
The failure of modern medicine to address the thyroid-gut connection stems from an over-reliance on a single, flawed metric: Thyroid Stimulating Hormone (TSH). The mainstream narrative suggests that if TSH is within the "normal" range (usually 0.5 to 4.5 mIU/L), the thyroid is functioning perfectly. This is a scientific fallacy of the highest order.
"The TSH Fallacy:"
TSH is a pituitary hormone, not a thyroid hormone. It measures what the brain *thinks* about the thyroid, not what is happening at the cellular level in the gut. A person can have a "normal" TSH while suffering from profound Type 2 Hypothyroidism—a state where the hormone is not being converted or used properly by the tissues. In many patients, the "reference range" is so broad that they can be clinically symptomatic for years before their TSH finally trips the alarm.
"The T4-Only Monopoly:"
The standard treatment in the NHS is Levothyroxine (T4). The assumption is that the body will naturally convert this T4 into the active T3. However, this conversion requires a healthy liver, a healthy gut, and an absence of chronic stress—conditions that are rarely met in someone suffering from SIBO. By providing only T4, doctors are giving the patient "unrefined fuel" that they cannot burn. Without T3, the gut transit remains slow, the SIBO persists, and the patient is told their symptoms are "psychosomatic" or "just IBS."
"The Dismissal of Subclinical Hypothyroidism:"
Mainstream guidelines often suggest "watchful waiting" for patients with slightly elevated TSH but normal T4. During this waiting period, the slow transit time is already wreaking havoc on the gut microbiome. By the time the patient qualifies for medication under current NHS protocols, they may have developed advanced SIBO, malabsorption syndromes, and autoimmune triggers (like Hashimoto's disease) caused by the chronic inflammation of a leaky gut.
UK Statistics: It is estimated that up to 1 in 10 women in the UK have some form of thyroid insufficiency, yet the prevalence of gastrointestinal complaints in this demographic is significantly higher, suggesting a massive under-diagnosis of the thyroid-gut link.
##
The UK Context
The British patient faces unique challenges when navigating the gut-thyroid axis. The structure of the NHS, while providing essential care, often lacks the nuance required for complex endocrine-metabolic disorders.
"The Postcode Lottery of Testing:"
In many NHS trusts, GPs are restricted from ordering Free T3 or Reverse T3 tests unless the TSH is severely abnormal. This means the most metabolically active hormone (T3) and the hormone that acts as a "blocker" (Reverse T3) are never even seen. Without these markers, the "Hormonal Brake" remains invisible.
"Iodine Deficiency in the British Isles:"
Unlike the United States, the UK has never implemented a mandatory salt iodisation programme. Historically, Britons received iodine through dairy products (due to iodine-based cleaners used in the dairy industry). As plant-based milk alternatives have surged in popularity, iodine intake has plummeted. A study by the *Lancet* found that the UK is now one of the top ten iodine-deficient nations in the developed world. Without iodine, the thyroid cannot even begin the process of hormone synthesis, leading to the metabolic stagnation discussed throughout this article.
"The "IBS" Trash-Can Diagnosis:"
In the UK, nearly 15-20% of the population is diagnosed with IBS at some point. Too often, "IBS" is used as a "trash-can diagnosis"—a label applied when the doctor doesn't know what is wrong. Because the TSH is "normal," the underlying thyroid-driven dysmotility is ignored, and the patient is prescribed "fibre" (which often worsens SIBO) or "antispasmodics" (which further slow the gut), exacerbating the very problem they aim to solve.
##
Protective Measures and Recovery Protocols
Healing the gut-thyroid axis requires a dual-pronged approach: one must release the "Hormonal Brake" by optimising thyroid function and simultaneously clear the "traffic jam" in the gut.
1. Optimising Thyroid Conversion
To get the gut moving, we must ensure T3 is reaching the enteric smooth muscles.
- —Selenium and Zinc: These minerals are the essential co-factors for the deiodinase enzymes. In the UK’s selenium-depleted soils, supplementation is often necessary.
- —Iodine Replenishment: After testing (such as a 24-hour urine loading test), judicious iodine supplementation, often accompanied by companion nutrients, can "restart" hormone production.
- —Red Light Therapy: Emerging research suggests that Photobiomodulation (red and near-infrared light) applied to the thyroid gland can reduce inflammation and increase T4-to-T3 conversion.
2. Addressing the Environmental Burden
- —Water Filtration: Using a high-quality filter that specifically removes fluoride and chlorine is non-negotiable for thyroid recovery in the UK.
- —The Halogen Cleanse: Increasing iodine intake can help "push out" bromide and fluoride from the receptors, though this must be done carefully to avoid a "detox flare."
3. Restoring Gut Motility
- —Natural Prokinetics: While the thyroid is being optimised, motility agents can provide temporary relief. Ginger, 5-HTP, and MotilPro (containing acetyl-L-carnitine) can help stimulate the MMC.
- —The Meal Spacing Rule: To allow the MMC to function, one must stop grazing. A minimum of 4-5 hours between meals and a 12-hour overnight fast is essential to allow the "hormonal brake" to be temporarily lifted.
- —The Role of Carbohydrates: Low-carb and ketogenic diets are currently popular but can be disastrous for thyroid patients. The body requires glucose and insulin to convert T4 to T3. A moderate intake of "safe" starches (like white rice or well-cooked root vegetables) is often necessary to support the metabolic rate.
4. Advanced Clinical Intervention
For those whose T4-monotherapy has failed, seeking a practitioner who will prescribe T3-containing medications (like Liothyronine or Natural Desiccated Thyroid) can be life-changing. Although difficult to obtain on the NHS, these "active" hormones bypass the conversion issues and directly stimulate the gut's smooth muscles, often resolving years of SIBO in a matter of weeks.
##
Summary: Key Takeaways
- —The Thyroid is the Engine: Thyroid hormones (specifically T3) are the primary drivers of the Migrating Motor Complex (MMC). Without them, the gut cannot sweep itself clean.
- —The Hormonal Brake: Hypothyroidism causes a profound slowdown in gastric emptying and intestinal transit, making SIBO an almost inevitable secondary condition.
- —The SIBO Feedback Loop: Slow transit leads to bacterial overgrowth (SIBO). These bacteria produce gases (methane) and toxins (LPS) that further suppress thyroid function, creating a vicious cycle of metabolic and digestive decline.
- —The Mainstream Failure: Relying solely on TSH and T4-monotherapy leaves millions of patients in a state of "functional hypothyroidism" where their blood looks fine, but their gut is stagnant.
- —The UK Environment: Fluoridated water, iodine-depleted soils, and a lack of comprehensive testing within the NHS contribute to a "perfect storm" for thyroid-gut dysfunction in the British population.
- —Recovery Requires T3: To truly heal the gut, one must optimise cellular T3 levels. This requires mineral support, environmental detoxification, and, in many cases, a shift away from standard T4-only medications.
The road to gastrointestinal health does not begin in the gut—it begins in the neck, with the butterfly-shaped gland that dictates the rhythm of life. Until we address the hormonal brake, every probiotic, antibiotic, and restrictive diet will remain a temporary sticking plaster on a systemic metabolic wound. True resolution of SIBO and chronic digestive distress requires a return to biological fundamentals: the restoration of metabolic energy. Only when the thyroid "spark" is reignited can the gut truly begin to move again.
This article is provided for informational and educational purposes only. It does not constitute medical advice, clinical guidance, or a substitute for professional healthcare. Information reflects cited research at time of publication. Always consult a qualified healthcare professional before acting on any health information.
RESEARCH FOUNDATIONS
Biological Credibility Archive
Hypothyroidism is significantly associated with Small Intestinal Bacterial Overgrowth (SIBO) because of reduced gastrointestinal motor activity and delayed transit.
Low thyroid hormone levels impair the electrical activity of the gut, resulting in prolonged esophageal transit and delayed gastric emptying.
The bidirectional gut-thyroid axis shows that slowed intestinal transit in hypothyroid patients alters the composition of the microbiome and increases the risk of dysbiosis.
Thyroid hormones are essential regulators of the enteric nervous system and smooth muscle contraction, directly influencing the frequency of the migratory motor complex.
Levothyroxine replacement therapy in patients with hypothyroidism has been shown to normalize gastrointestinal transit time and alleviate chronic constipation.
Citations provided for educational reference. Verify via PubMed or institutional databases.
Medical Disclaimer
The information in this article is for educational purposes only and does not constitute medical advice, diagnosis, or treatment. Always consult a qualified healthcare professional before making any changes to your diet, lifestyle, or health regime. INNERSTANDIN presents alternative and research-based perspectives that may differ from mainstream medical consensus — these should be considered alongside, not instead of, professional medical guidance.
Read Full DisclaimerReady to learn more?
Continue your journey through our classified biological research.
DISCUSSION ROOM
Members of THE COLLECTIVE discussing "Hypothyroidism and Gut Transit: The Hormonal Brake on Digestion"
SILENT CHANNEL
Be the first to discuss this article. Your insight could help others understand these biological concepts deeper.
THE ARSENAL
Based on SIBO & Small Intestine Health — products curated by our research team for educational relevance and biological support.

Magnesium Blend – The Most Important Mineral
Energy Blend Supports

Lugol’s Iodine – Hormonal Issues, Menopause, Immune System, Brain Fog, Memory, Thyroid, Dry Skin
INNERSTANDING may earn a commission on purchases made through these links. All products are selected based on rigorous educational relevance to our biological research.
RABBIT HOLE
Follow the biological thread deeper