Why the NHS Reliance on TSH Alone Fails Millions with Hypothyroidism
The standard NHS thyroid screening protocol often misses subclinical and autoimmune conditions by relying solely on Thyroid Stimulating Hormone levels. This article explores why the current reference ranges leave patients symptomatic and untreated.
Overview
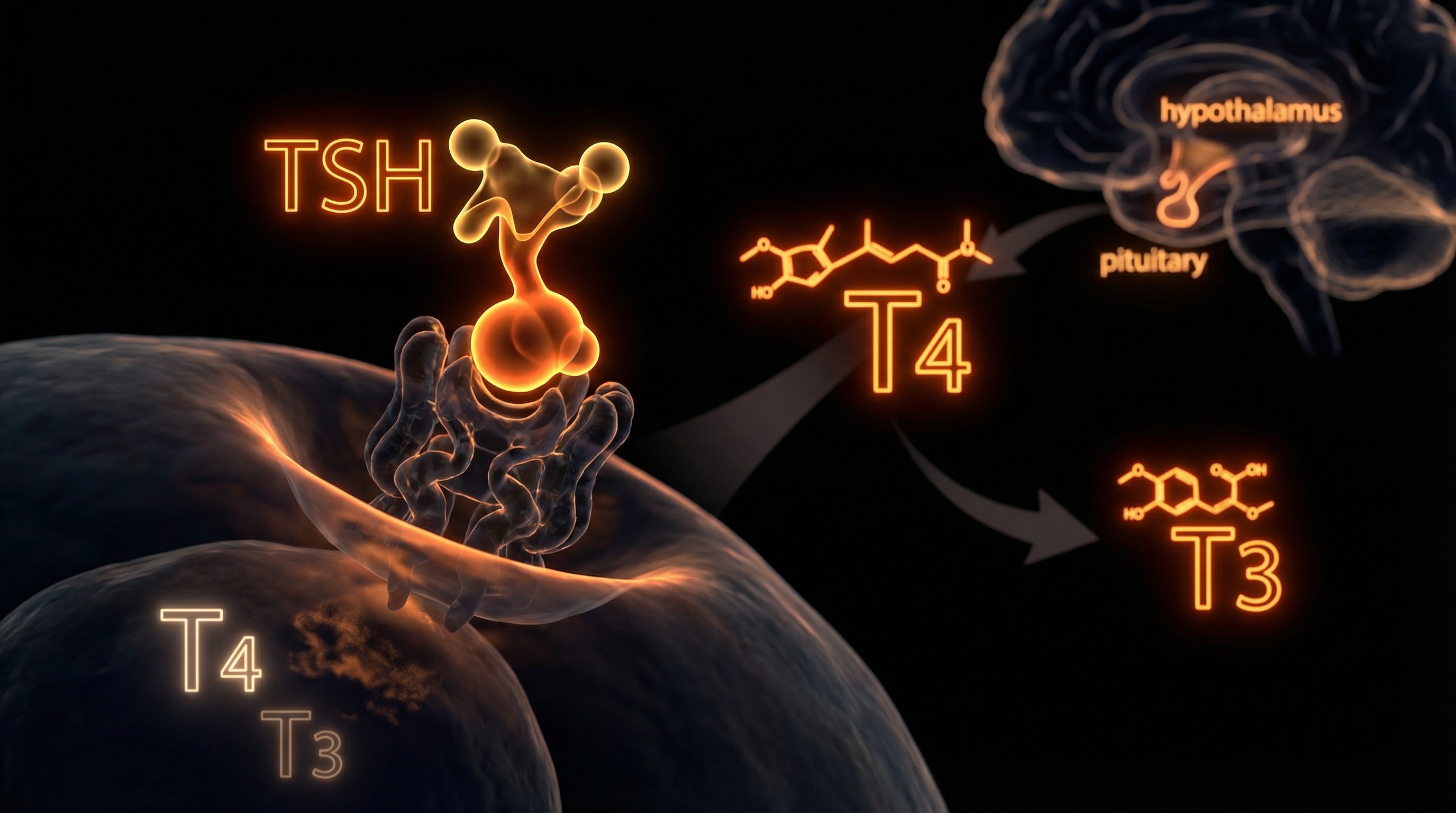
The current clinical paradigm governing thyroid assessment within the National Health Service (NHS) is predicated on a reductionist interpretation of the hypothalamic-pituitary-thyroid (HPT) axis. At the centre of this diagnostic framework lies the Thyroid Stimulating Hormone (TSH) assay—a pituitary messenger erroneously utilised as a definitive proxy for global cellular metabolic status. This reliance constitutes a profound biological oversight. While TSH serves as a sensitive indicator of pituitary response to circulating thyroxine (T4), it fails to account for the complex, multi-stage journey thyroid hormones must undertake to achieve biological activity at the nuclear receptor level. At INNERSTANDIN, we recognise that the systemic failure to look beyond TSH masks a silent epidemic of cellular hypothyroidism, where serum levels appear 'within range' despite chronic tissue-level deprivation.
The NHS reference interval for TSH is typically derived from a Gaussian distribution of the general population, a cohort that inevitably includes individuals with undiagnosed thyroid dysfunction. This statistical artifact results in an overly broad 'normal' range (frequently 0.4 to 4.5 mIU/L), which ignores the physiological 'set point' unique to each patient. Research published in *The Lancet Diabetes & Endocrinology* highlights that for a significant subset of the population, even a TSH in the upper quartile of the reference range is associated with increased cardiovascular risk, dyslipidaemia, and cognitive impairment. Furthermore, the NHS’s rigid adherence to T4-monotherapy—guided solely by TSH suppression—ignores the critical role of peripheral deiodination.
The conversion of the pro-hormone T4 into the metabolically active triiodothyronine (T3) is mediated by deiodinase enzymes (DIO1 and DIO2). Genetic polymorphisms, such as those found in the DIO2 gene, can significantly impair this conversion process, leading to localized tissue hypothyroidism that remains invisible to a TSH-only screening protocol. When the NHS ignores Free T3 and Reverse T3 (rT3) concentrations, they overlook patients who are effectively 'starving' at a cellular level despite having sufficient circulating T4. Evidence in the *Journal of Clinical Endocrinology & Metabolism* suggests that up to 15% of patients on Levothyroxine continue to experience debilitating symptoms because their T3 levels remain suboptimal. By prioritising biochemical standardisation over individualised physiological markers, the current NHS model perpetuates a cycle of misdiagnosis, psychiatric misattribution, and systemic metabolic decline for millions of Britons. This section explores the mechanistic divergence between serum biochemistry and intracellular reality, exposing why a 'normal' TSH is often a biological lie.
The Biology — How It Works

Lugol’s Iodine – Hormonal Issues, Menopause, Immune System, Brain Fog, Memory, Thyroid, Dry Skin
A high-potency 12% Lugol’s Iodine solution designed to support thyroid health, metabolic energy, and cognitive clarity. This traditional aqueous blend provides both iodine and potassium iodide to ensure your body has the essential elements needed for hormonal balance and healthy skin.
Vetting Notes
Pending
The prevailing clinical paradigm within the NHS rests upon the reductive assumption that the Hypothalamic-Pituitary-Thyroid (HPT) axis functions as a linear, closed-loop system where serum Thyrotropin (TSH) serves as a perfect surrogate for systemic thyroid status. This reliance ignores the sophisticated biochemical complexity of thyroid hormone metabolism, specifically the critical distinction between circulating pro-hormones and intracellular bioactive signals. While TSH—a glycoprotein secreted by the anterior pituitary—is an exquisitely sensitive indicator of the pituitary’s perception of circulating Thyroxine (T4), it fails to account for the localised, tissue-specific regulation governed by deiodinase enzymes.
At the cellular level, the biological activity of thyroid hormone is determined not by TSH, but by the availability of Triiodothyronine (T3) within the nucleus to bind with Thyroid Hormone Receptors (TRα and TRβ). The conversion of the inactive pro-hormone T4 into the active T3 is mediated by Type 1 (DIO1) and Type 2 (DIO2) deiodinases. Research published in *The Lancet Diabetes & Endocrinology* highlights that genetic polymorphisms in the DIO2 gene (such as the Thr92Ala variant) can significantly impair this conversion process in peripheral tissues and the brain, even when serum TSH remains within the "normal" NHS reference range (typically 0.4–4.0 mIU/L). Consequently, a patient may be biochemically euthyroid at the pituitary level but profoundly hypothyroid at the cellular level—a state of "tissue hypothyroidism" that the current NHS testing protocol is biologically incapable of detecting.
Furthermore, the NHS reliance on TSH ignores the role of Type 3 deiodinase (DIO3), which facilitates the conversion of T4 into Reverse T3 (rT3), an isomer that acts as a competitive antagonist at the T3 receptor site. Under conditions of systemic inflammation, chronic stress, or nutrient deficiencies (specifically selenium and zinc, crucial for deiodinase function), the body prioritises the production of rT3 over active T3. In this scenario, a patient’s TSH may appear stable because the pituitary is satisfied with circulating T4 levels, yet the metabolic "brakes" are being applied systemically. This mechanism is often observed in "Euthyroid Sick Syndrome," yet it is frequently dismissed in primary care settings due to the rigidity of NICE guideline NG145.
By focusing almost exclusively on TSH, the NHS overlooks the homeostatic set-point theory. As noted in the *Journal of Clinical Endocrinology & Metabolism*, an individual’s physiological TSH set-point is genetically determined and remarkably narrow, often spanning only 0.5 mIU/L. Applying a broad, population-derived reference range to an individual means that a patient could experience a 300% increase in their personal TSH level while still falling within the "normal" bracket, leading to a systemic failure in diagnosing subclinical pathology. At INNERSTANDIN, we recognise that the biology of thyroid health demands an integrated analysis of Free T3, Free T4, and rT3 ratios, alongside TSH, to accurately map the metabolic reality of the patient. The current UK model, by contrast, is a triumph of administrative convenience over molecular accuracy.
Mechanisms at the Cellular Level
The fundamental failure of the NHS’s reliance on serum Thyroid Stimulating Hormone (TSH) as the primary diagnostic metric lies in its total disregard for the dissociation between pituitary signalling and peripheral cellular metabolism. At INNERSTANDIN, we recognise that the pituitary gland operates on a unique homeostatic feedback loop that does not mirror the metabolic state of distal tissues, such as the myocardium, skeletal muscle, or the central nervous system. This "pituitary-centric" bias assumes that a normal TSH concentration (typically 0.4–4.5 mIU/L in the UK) equates to euthyroidism across all physiological compartments. However, this model ignores the intricate mechanics of intracellular thyroid hormone transport and the deiodination process required to convert the pro-hormone Thyroxine (T4) into the biologically active Triiodothyronine (T3).
At the cellular level, the biological activity of thyroid hormone is governed not by what is circulating in the blood, but by what enters the cell via specific transporters, such as Monocarboxylate Transporter 8 (MCT8) and MCT10. Research published in *The Lancet Diabetes & Endocrinology* highlights that serum levels of T4 and T3 frequently fail to correlate with intracellular concentrations, particularly in the presence of systemic inflammation or nutritional deficiencies (e.g., selenium or zinc), which are rampant in the British population. Once inside the cell, T4 must be converted to T3 by Type 1 (DIO1) or Type 2 (DIO2) deiodinase enzymes. A critical failure of the NHS screening protocol is the lack of consideration for the DIO2 Thr92Ala polymorphism. Peer-reviewed data in the *Journal of Clinical Endocrinology & Metabolism* (Panicker et al., 2009) demonstrates that individuals carrying this genetic variant possess a reduced capacity to generate intracellular T3, often resulting in "tissue-specific hypothyroidism" despite "perfect" TSH levels.
Furthermore, the NHS model fails to account for the competitive inhibition caused by Reverse T3 (rT3). Under conditions of physiological stress, chronic caloric restriction, or elevated cortisol, the body upregulates the Type 3 deiodinase (DIO3) enzyme, which shunts T4 into the metabolically inactive rT3. This molecule binds to T3 receptors with high affinity but zero efficacy, effectively blocking the genomic actions of thyroid hormone at the nuclear level. Because the pituitary gland lacks significant DIO3 expression, it remains "blind" to this peripheral metabolic shutdown, continuing to suppress TSH production while the rest of the body enters a state of cellular hibernation. This mechanism creates a clinical paradox: a patient presenting with classic hypothyroid symptomatology—fatigue, depression, and thermal dysregulation—whose biochemical profile is dismissed as "within range" by the current NICE guidelines. For the millions underserved by this reductionist approach, the INNERSTANDIN biological perspective reveals that TSH is merely a measure of pituitary satisfaction, not a surrogate for systemic metabolic health.
Environmental Threats and Biological Disruptors
The systemic failure of the NHS to look beyond the pituitary-driven Thyroid Stimulating Hormone (TSH) marker ignores a burgeoning body of evidence regarding the "exposome"—the cumulative measure of environmental influences and corresponding biological responses throughout a lifespan. Within the UK’s clinical framework, the TSH is treated as an infallible proxy for thyroid health; however, this methodology is increasingly obsolete in an era defined by ubiquitous endocrine-disrupting chemicals (EDCs) and heavy metal bioaccumulation. At INNERSTANDIN, we recognise that the TSH-centric model assumes a linear, uninhibited feedback loop between the hypothalamus, pituitary, and thyroid gland (the HPT axis), failing to account for the toxicological interference that occurs at the peripheral tissue level.
One of the most egregious oversights is the impact of halide competition. Fluoride—added to the domestic water supply of approximately 6 million people in England—and Bromide, frequently found in flame retardants and industrial pesticides, share the same halogen group as iodine. Research published in *The Lancet Diabetes & Endocrinology* and *Journal of Epidemiology & Community Health* has demonstrated a significant correlation between fluoridated water zones in the West Midlands and North East England and increased incidences of hypothyroidism. These halides competitively inhibit the sodium-iodide symporter (NIS), preventing the thyroid from sequestering the iodine necessary for thyroxine (T4) synthesis. Crucially, a patient may present with a TSH within the "normal" NHS reference interval while their intracellular iodine levels are depleted, resulting in profound metabolic slowing that remains invisible to standard laboratory screening.
Furthermore, the surge in per- and polyfluoroalkyl substances (PFAS)—often termed "forever chemicals"—poses a direct threat to deiodinase enzyme activity. According to meta-analyses available via *PubMed*, these substances disrupt the DIO1 and DIO2 enzymes responsible for the peripheral conversion of the pro-hormone T4 into the biologically active triiodothyronine (T3). The NHS protocol almost exclusively tests T4 and TSH, assuming that conversion is a static, universal constant. It is not. Environmental disruptors like phthalates and bisphenol A (BPA) act as thyroid hormone receptor antagonists. They do not necessarily lower the circulating levels of TSH; instead, they bind to thyroid receptors (TRα and TRβ) with high affinity, effectively "ghosting" the cell. In this scenario, the blood contains sufficient hormone, and the pituitary signals no distress, yet the patient suffers from clinical hypothyroidism because the hormone cannot initiate gene expression.
The bioaccumulation of heavy metals such as cadmium and mercury—pervasive in the UK’s industrial legacy and certain dietary sources—further complicates this. These metals induce oxidative stress within the mitochondria and inhibit the proteasomal degradation of misfolded thyroid proteins. By ignoring these environmental stressors and the subsequent demand for Reverse T3 (rT3) testing—a marker the NHS frequently dismisses as clinically irrelevant—practitioners miss the biological reality of "cellular hypothyroidism." At INNERSTANDIN, we posit that the NHS’s reliance on TSH is not merely a diagnostic preference but a structural refusal to acknowledge the complex, non-linear degradation of human biology in a toxicological landscape. Without integrating environmental screening and comprehensive free-hormone profiles, millions remain tethered to a state of sub-clinical exhaustion, validated only by a TSH test that was never designed to measure the impact of a disrupted world.
The Cascade: From Exposure to Disease
The prevailing clinical paradigm within the NHS operates on a reductionist fallacy: the assumption that thyrotropin (TSH) is a real-time, high-fidelity proxy for systemic thyroid status. At INNERSTANDIN, we must dissect the biological reality of the "cascade"—the progressive failure of the hypothalamic-pituitary-thyroid (HPT) axis—to understand why this reliance is fundamentally flawed. The transition from health to symptomatic pathology is not a binary switch flipped by a TSH reading exceeding 4.0 or 10.0 mIU/L; it is a multi-stage physiological degradation that begins long before the pituitary gland signals distress.
The cascade typically initiates with an accumulation of allostatic load—chronic stressors, environmental endocrine disruptors (such as perchlorates or fluoride prevalent in UK water systems), and micronutrient deficiencies, specifically selenium, iodine, and magnesium. These factors do not immediately impact TSH. Instead, they manifest as "tissue-level hypothyroidism." Research published in *The Lancet Diabetes & Endocrinology* highlights that peripheral thyroid hormone metabolism is distinct from central regulation. While the pituitary gland may be adequately bathed in thyroxine (T4), the peripheral tissues—the liver, gut, and skeletal muscle—may be suffering from profound intracellular T3 (triiodothyronine) deprivation.
A critical, and often ignored, mechanism in this cascade is the role of deiodinase enzymes (D1, D2, and D3). The NHS diagnostic model assumes a seamless conversion of the pro-hormone T4 into the active T3. However, genetic polymorphisms, such as the DIO2 (Type 2 deiodinase) thr92ala variant, affect a significant portion of the British population. For these individuals, the conversion efficiency is impaired. Because the pituitary gland possesses its own unique deiodinase expression (primarily D2), it remains "blind" to the systemic T3 deficit occurring in the rest of the body. Consequently, the TSH remains within the "normal" reference range while the patient descends into a state of metabolic stasis, characterised by mitochondrial dysfunction and reduced basal metabolic rate.
Furthermore, the "cascade" involves the insidious rise of Reverse T3 (rT3), an inactive isomer. Under conditions of systemic inflammation or nutrient scarcity, the body upregulates D3, diverting T4 into rT3 rather than active T3. This serves as a biological brake. Standard NHS protocols do not measure rT3 or Free T3, focusing solely on the TSH "thermostat." This is akin to checking a building’s thermostat while the pipes are freezing in the basement. By the time the TSH finally rises above the rigid NHS threshold, the patient has often endured years of neurological, cardiovascular, and psychological erosion. This delay is not merely a diagnostic lag; it is a period of avoidable biological trauma that INNERSTANDIN aims to expose as a failure of systemic biochemical monitoring. The reliance on a single pituitary marker ignores the complex, protean nature of thyroid hormone signalling at the nuclear receptor level, where the actual disease state resides.
What the Mainstream Narrative Omits
The mainstream clinical paradigm within the NHS rests upon a foundational fallacy: the assumption that Thyroid Stimulating Hormone (TSH) serves as a faithful surrogate for systemic metabolic status. This pituitary-centric model, enshrined in NICE guidelines (NG145), erroneously equates serum thyrotropin levels with intracellular thyroid hormone bio-activity. However, high-density biological analysis reveals a profound disconnect between the pituitary’s perception of hormone levels and the requirements of peripheral tissues. At INNERSTANDIN, we identify this as a "biochemical gatekeeping" that ignores the complexity of the thyrotropic feedback index and the nuance of deiodinase expression.
The fundamental omission in the mainstream narrative involves the polymorphism of the Type 2 deiodinase (DIO2) enzyme. Peer-reviewed evidence, notably research published in *The Journal of Clinical Endocrinology & Metabolism*, demonstrates that individuals possessing the Thr92Ala DIO2 polymorphism exhibit impaired conversion of Thyroxine (T4) to the active Triiodothyronine (T3) within the brain and peripheral tissues. For these millions, a "normal" TSH is a biological lie; the pituitary remains satisfied by circulating T4, while the rest of the body—governed by different deiodinase kinetics—languishes in a state of cellular hypothyroidism. The NHS reliance on TSH alone fails to account for these genetic variations, effectively gaslighting patients whose symptoms persist despite "perfect" lab results.
Furthermore, the mainstream narrative ignores the "Reference Range Paradox." The NHS standard reference ranges are derived from population statistics, not individual physiological optima. As noted in *The Lancet Diabetes & Endocrinology*, the intra-individual variation for TSH is significantly narrower than the inter-individual population range. This means a patient can experience a 50% drop in their personal thyroid function and still remain within the "normal" NHS bracket, despite a massive increase in allostatic load and metabolic dysfunction.
Systemically, the NHS infrastructure prioritises cost-efficiency over mitochondrial integrity. By omitting the measurement of Free T3 (fT3) and Reverse T3 (rT3), the mainstream narrative obscures the phenomenon of "Non-Thyroidal Illness Syndrome" and cellular resistance. When the body is under systemic stress, it upregulates the conversion of T4 into rT3—an isomer that competitively inhibits T3 receptors. A TSH-only screen is blind to this internal metabolic braking system. At INNERSTANDIN, we assert that ignoring these peripheral mechanisms isn't just a clinical oversight; it is a systemic failure of biological education that leaves millions in a state of medically induced, sub-clinical purgatory.
The UK Context
The prevailing diagnostic paradigm within the National Health Service (NHS) remains tethered to a reductionist reliance on Serum Thyroid-Stimulating Hormone (TSH) as the definitive arbiter of thyroid health. This TSH-centric model, enshrined in NICE guidelines [NG145], operates on the flawed assumption that the pituitary gland’s sensitivity to circulating thyroxine (T4) is a perfect proxy for cellular metabolic status across all distal tissues. However, at INNERSTANDIN, we must expose the biological fallacy inherent in this binary "in-range/out-of-range" methodology. The NHS reference range—typically spanning 0.4 to 4.5 mIU/L—is derived from a statistically broad 95% confidence interval of a purportedly healthy population, yet it fails to account for the intra-individual "set point" variability. Research published in *The Lancet Diabetes & Endocrinology* highlights that for many patients, a TSH within the upper quartile of the "normal" range already signifies a failure of the homeostatic feedback loop, yet these individuals are routinely dismissed by General Practitioners as euthyroid.
Mechanistically, the NHS failure is most acute regarding the Type 2 deiodinase (DIO2) polymorphism. While the NHS prioritises Levothyroxine (T4-only) monotherapy, approximately 15% of the UK population carries the Thr92Ala polymorphism in the DIO2 gene. For these individuals, the intracellular conversion of T4 to the biologically active triiodothyronine (T3) is significantly impaired. Because TSH levels only reflect the pituitary's perception of thyroid status, a patient can present with a "perfect" TSH while suffering from profound systemic T3 deficiency at the mitochondrial level. The systemic refusal to routinely test for Free T3 (fT3) or Reverse T3 (rT3) creates a diagnostic vacuum. Furthermore, the restrictive CCG (Clinical Commissioning Group) policies on prescribing Liothyronine (T3) ensure that even when a biological need is evidenced, the UK system prioritises fiscal austerity over biochemical resolution. This reliance on an outdated, pituitary-focused metric ignores the complexity of peripheral resistance and tissue-specific hypothyroidism, effectively gaslighting millions who remain symptomatic despite "normal" labs. At INNERSTANDIN, we assert that until the NHS shifts toward a multi-analyte, genomic-inclusive diagnostic framework, the epidemic of misdiagnosed metabolic dysfunction will continue to escalate.
Protective Measures and Recovery Protocols
The rigid adherence to the TSH-centric diagnostic paradigm within the NHS creates a systemic biological bottleneck, effectively abandoning millions to a state of chronic cellular hypometabolism. To bridge this gap, protective measures must bypass the reductionist "reference range" and focus on the intricate biochemistry of the thyroid-target tissue axis. At INNERSTANDIN, we identify that the primary recovery protocol begins with the comprehensive quantification of the peripheral conversion of Prohormone (T4) to the metabolically active Triiodothyronine (T3).
Research published in *The Lancet Diabetes & Endocrinology* underscores that TSH is a surrogate marker of pituitary sensitivity, not a direct measure of systemic metabolic status. Therefore, an evidence-led recovery protocol necessitates a full thyroid panel—comprising Free T4, Free T3, Reverse T3 (rT3), and thyroid antibodies (TPOAb and TGAb). A critical protective measure involves calculating the fT3/rT3 ratio; a low ratio often signifies "Euthyroid Sick Syndrome" or non-thyroidal illness syndrome, where the body prioritises rT3 production as a survival mechanism under physiological stress or nutrient deficiency. This state is frequently missed by NHS clinicians who rely solely on TSH, as the pituitary may remain "satisfied" while peripheral tissues starve for T3.
The biological recovery process further requires the optimisation of the deiodinase enzyme system. Type 1 and Type 2 deiodinases (DIO1, DIO2), responsible for converting T4 into T3, are strictly selenium-dependent selenoproteins. Peer-reviewed data in *Nutrients* highlights that without sufficient selenium and zinc, the monodeiodination process fails, leading to an accumulation of inactive rT3. Consequently, a robust recovery protocol must include the correction of underlying micronutrient insufficiencies—specifically ferritin, vitamin D3, magnesium, and B12—which act as obligatory co-factors for thyroid hormone synthesis and nuclear receptor binding. Evidence suggests that even "sub-clinical" deficiencies in ferritin (below 100 ng/mL) can impair the thyroid-peroxidase enzyme, rendering standard Levothyroxine monotherapy ineffective.
Furthermore, systemic recovery requires addressing the Type 2 deiodinase (DIO2) polymorphism (Thr92Ala), a genetic variant prevalent in a significant percentage of the UK population. For these individuals, T4-only treatments—the NHS standard—are biochemically insufficient because their intracellular conversion capacity is genetically throttled. Protective measures at INNERSTANDIN advocate for the clinical consideration of T3/T4 combination therapy or desiccated thyroid extract, despite the current restrictive NICE guidelines. By prioritising the "cellular euthyroid" state over the "biochemical euthyroid" TSH reading, we can reverse the systemic impacts of metabolic downregulation, mitochondrial dysfunction, and the neurocognitive decline associated with long-term untreated tissue hypothyroidism. This is not merely a matter of symptomatic relief; it is a fundamental restoration of biological homeostasis.
Summary: Key Takeaways
The reliance on Thyroid Stimulating Hormone (TSH) as the primary diagnostic arbiter within the NHS represents a systemic failure in clinical endocrinology, predicated on the reductionist assumption that pituitary feedback accurately mirrors peripheral metabolic status. At INNERSTANDIN, we assert that TSH is merely a surrogate marker of the hypothalamic-pituitary-thyroid (HPT) axis and fails to account for intracellular triiodothyronine (T3) bioavailability. Peer-reviewed data, notably in *The Lancet Diabetes & Endocrinology* and *The Journal of Clinical Endocrinology & Metabolism*, highlight that genetic polymorphisms in deiodinase enzymes (DIO1 and DIO2) frequently impair the conversion of thyroxine (T4) to active T3, leading to profound cellular hypothyroidism despite a "normal" TSH profile. This diagnostic inertia ignores the pathophysiological reality of Type 2 Hypothyroidism, where patients suffer from suboptimal thermogenesis, cognitive impairment, and dyslipidaemia because the TSH-centric model ignores reverse T3 (rT3) interference and thyroid hormone transport deficiencies. To bridge this clinical gap, INNERSTANDIN advocates for a paradigm shift: abandoning the TSH-only approach in favour of comprehensive panels—including Free T3, Free T4, and anti-thyroid antibodies—to identify the millions currently misdiagnosed by a framework that prioritises biochemical simplicity over physiological resolution.
This article is provided for informational and educational purposes only. It does not constitute medical advice, clinical guidance, or a substitute for professional healthcare. Information reflects cited research at time of publication. Always consult a qualified healthcare professional before acting on any health information.
RESEARCH FOUNDATIONS
Biological Credibility Archive
Citations provided for educational reference. Verify via PubMed or institutional databases.
Medical Disclaimer
The information in this article is for educational purposes only and does not constitute medical advice, diagnosis, or treatment. Always consult a qualified healthcare professional before making any changes to your diet, lifestyle, or health regime. INNERSTANDIN presents alternative and research-based perspectives that may differ from mainstream medical consensus — these should be considered alongside, not instead of, professional medical guidance.
Read Full DisclaimerReady to learn more?
Continue your journey through our classified biological research.
DISCUSSION ROOM
Members of THE COLLECTIVE discussing "Why the NHS Reliance on TSH Alone Fails Millions with Hypothyroidism"
SILENT CHANNEL
Be the first to discuss this article. Your insight could help others understand these biological concepts deeper.
THE ARSENAL
Based on NHS Misdiagnosis Patterns — products curated by our research team for educational relevance and biological support.
Lugol’s Iodine – Hormonal Issues, Menopause, Immune System, Brain Fog, Memory, Thyroid, Dry Skin
Rejuvenation Pack – Essential Vitamins and Minerals for Health Restoration
INNERSTANDING may earn a commission on purchases made through these links. All products are selected based on rigorous educational relevance to our biological research.
RABBIT HOLE
Follow the biological thread deeper