Why the NHS Reliance on TSH Testing Leaves Millions Hypothyroid
Standard thyroid screening in the UK often misses subclinical or cellular hypothyroidism by relying solely on Thyroid Stimulating Hormone (TSH). This article explores why current reference ranges are insufficient and what markers are required for an accurate diagnosis.
# Why the NHS Reliance on TSH Testing Leaves Millions Hypothyroid
Overview
In the clinical landscape of the United Kingdom, a silent crisis is unfolding within the consulting rooms of General Practitioners from Cornwall to the Highlands. Millions of individuals—predominantly women—present with a debilitating constellation of symptoms: chronic fatigue that no amount of sleep can rectify, unexplained weight gain, cognitive "brain fog" that disrupts professional life, thinning hair, and a pervasive sensitivity to cold. Yet, after a routine blood test, these patients are summarily dismissed with a clean bill of health. The verdict is almost always the same: "Your results are within the normal range."
The "normal range" in question refers almost exclusively to Thyroid Stimulating Hormone (TSH). For decades, the National Health Service (NHS) has utilised TSH as the "gold standard" and often the sole marker for screening thyroid dysfunction. This reliance is not merely a clinical preference; it is a systemic bottleneck enforced by NICE (National Institute for Health and Care Excellence) guidelines and internal laboratory "reflex" protocols that prevent further testing if TSH falls within a broad, historically arbitrary window.
At INNERSTANDING, we recognise this as a profound failure of biological logic. By treating TSH as the definitive proxy for thyroid health, the medical establishment ignores the complex, multi-stage journey of thyroid hormone from the gland to the nucleus of every cell in the human body. This article will expose why the TSH-only model is a relic of 20th-century reductionism that fails to account for cellular hypothyroidism, conversion disorders, and the autoimmune realities of Hashimoto’s Disease. We are witnessing a systemic dismissal of patient experience in favour of administrative efficiency and cost-cutting, leaving a significant portion of the British population trapped in a state of metabolic bankruptcy.
Over 90% of all thyroid prescriptions in the UK are for Levothyroxine (synthetic T4), yet surveys suggest that approximately 15% of patients on this "standard of care" continue to suffer from persistent hypothyroid symptoms despite having "perfect" TSH levels.
##
##
The Biology — How It Works

Lugol’s Iodine – Hormonal Issues, Menopause, Immune System, Brain Fog, Memory, Thyroid, Dry Skin
A high-potency 12% Lugol’s Iodine solution designed to support thyroid health, metabolic energy, and cognitive clarity. This traditional aqueous blend provides both iodine and potassium iodide to ensure your body has the essential elements needed for hormonal balance and healthy skin.
Vetting Notes
Pending
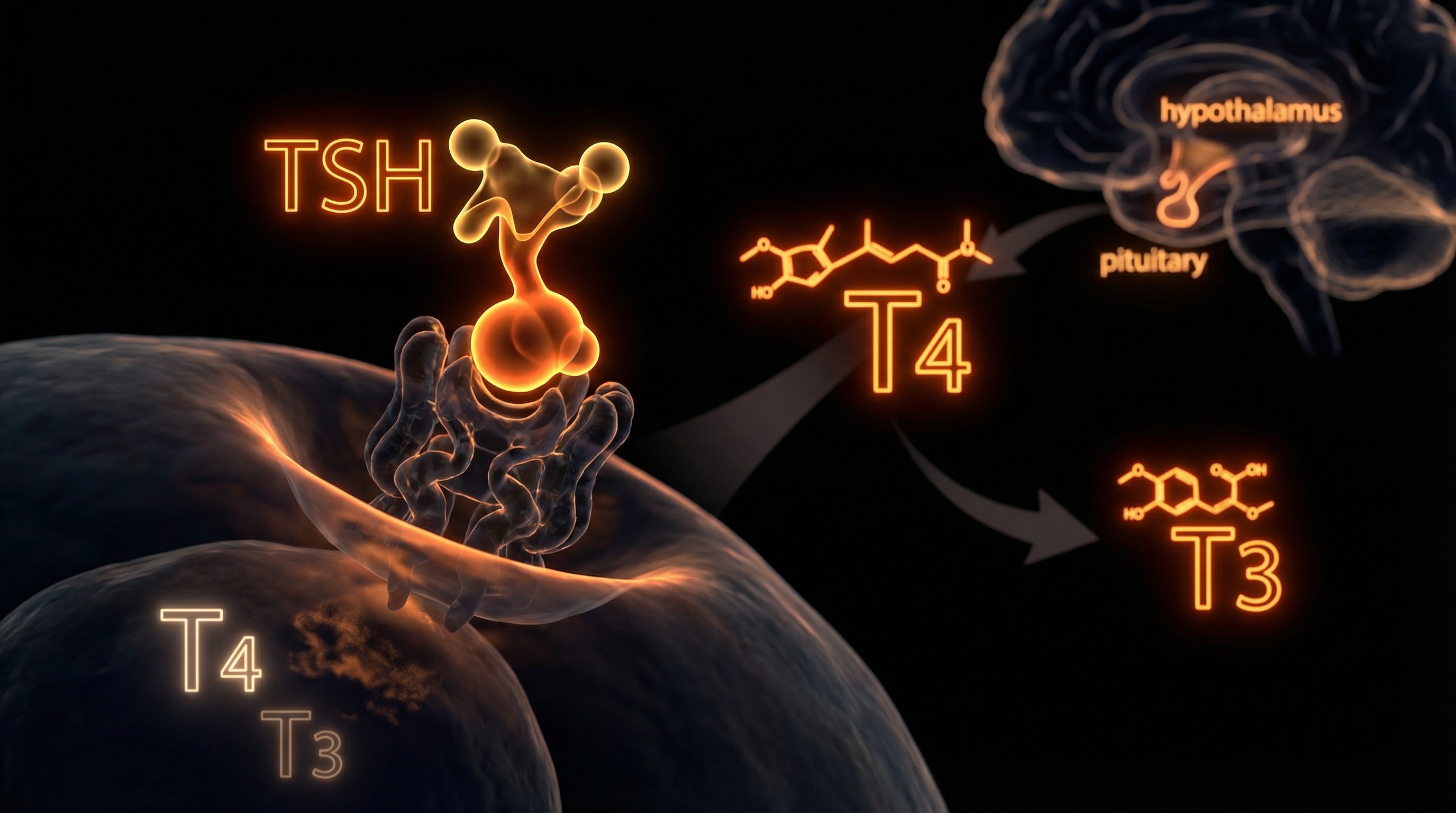
To understand why TSH is an insufficient marker, we must first master the hierarchy of the Hypothalamic-Pituitary-Thyroid (HPT) axis. The process begins in the hypothalamus, which releases Thyrotropin-Releasing Hormone (TRH). This signals the anterior pituitary gland to produce Thyroid Stimulating Hormone (TSH). TSH then travels to the thyroid gland, a butterfly-shaped organ in the neck, commanding it to produce two primary hormones: Thyroxine (T4) and Triiodothyronine (T3).
The thyroid produces approximately 80-90% T4 and only 10-20% T3. T4 is biologically inactive; it is effectively a pro-hormone, a storage vessel. For the body to function, T4 must be converted into T3, which is the active form that drives metabolic rate, body temperature, and cellular repair. This conversion primarily occurs in the liver, kidneys, and peripheral tissues through the removal of one iodine atom.
The Pituitary Is Not the Body
The fundamental flaw in the NHS model is the assumption that the pituitary gland’s perception of thyroid hormone levels reflects the reality in the rest of the body. The pituitary gland is unique; it possesses specific transporters and enzymes that make it far more sensitive to T4 levels than other tissues like the heart, brain, or muscles.
A patient may have a "normal" TSH (indicating the pituitary is satisfied), while their peripheral tissues are starving for active T3. This state is known as Tissue-Level Hypothyroidism. By only measuring TSH, the NHS is essentially checking the thermostat in the hallway (the pituitary) to determine if the radiator in the bedroom (the cells) is working. If the thermostat is satisfied, the system assumes the whole house is warm, even if the patient is biologically freezing.
The Critical Role of Free Hormones
Standard NHS testing often overlooks the distinction between "Total" and "Free" hormones. Most thyroid hormone in the blood is bound to proteins (such as Thyroid-Binding Globulin or TBG), rendering it inactive. Only the "Free" portions (Free T4 and Free T3) are available to enter the cells. Factors common in the UK population—such as high oestrogen levels from the contraceptive pill or HRT—can increase binding proteins, leaving a patient with "normal" total levels but insufficient "free" active hormone.
##
##
Mechanisms at the Cellular Level
The true action of thyroid hormone happens inside the cell, specifically within the mitochondria and the nucleus. This is where the mainstream narrative completely breaks down. Even if a patient has sufficient T4 in their bloodstream, several "gatekeeper" mechanisms can prevent that hormone from ever exerting its biological effect.
The Deiodinase System: The Internal Switches
The conversion of T4 to T3 is governed by a group of enzymes called Deiodinases (D1, D2, and D3). These are selenium-dependent enzymes that act as local switches:
- —D1 and D2 convert T4 into the active T3.
- —D3 is the "off-switch," converting T4 into Reverse T3 (rT3), an isomer that is biologically inactive and actually blocks the T3 receptors.
In states of chronic stress, illness, or nutrient deficiency, the body purposefully upregulates D3. This is a survival mechanism designed to slow the metabolism during "famine" or "injury." However, in the modern British environment, this "famine" signal is triggered by chronic work stress, processed diets, and environmental toxins. The result is a high level of rT3.
Reverse T3 (rT3) acts as a competitive inhibitor; it sits in the cellular receptor like a broken key in a lock, preventing active T3 from entering. The NHS almost never tests for rT3, meaning they are blind to this cellular "braking system."
Transport and Nuclear Signalling
Once T3 is in the vicinity of a cell, it must be transported across the cell membrane by specific carrier proteins, such as MCT8 (Monocarboxylate Transporter 8). Genetic variations or inflammatory cytokines can impair these transporters.
Inside the cell, T3 must bind to Thyroid Hormone Receptors (TR) in the nucleus. This binding triggers the transcription of DNA, essentially telling the cell to produce energy (ATP), consume oxygen, and perform its specific function. If there is Systemic Inflammation (indicated by high C-Reactive Protein), these receptors become desensitised. You can flood the blood with Levothyroxine, but if the receptors are deaf to the signal, the patient remains symptomatic. This is Thyroid Hormone Resistance, a condition entirely ignored by standard NHS protocols.
##
##
Environmental Threats and Biological Disruptors
The thyroid gland is the body’s "sentinel," highly sensitive to environmental changes. In the UK, we are exposed to a cocktail of chemicals that directly interfere with thyroid physiology, many of which are poorly regulated or legacy issues from our industrial past.
The Halogen Competition
The thyroid requires Iodine to produce T4 and T3. However, iodine belongs to the Halogen group on the periodic table, which also includes Fluorine, Chlorine, and Bromine. Because these elements have similar atomic structures, they compete for the same receptors in the thyroid gland.
- —Fluoride: Many regions in the UK (such as the West Midlands and parts of the North East) have fluoridated water. Fluoride is a known goitrogen that can displace iodine and inhibit the enzymes required for hormone synthesis.
- —Chlorine: Present in almost all UK tap water and swimming pools, chlorine further competes for iodine uptake.
- —Bromine: Found in "potassium bromate," an additive used in some commercial breads (though restricted, it persists in various food-grade plastics and flame retardants), bromine is a potent thyroid disruptor.
Endocrine Disrupting Chemicals (EDCs)
The UK’s Environment Agency has flagged numerous Persistent Organic Pollutants (POPs) in our waterways. Chemicals like PFAS (the "forever chemicals" used in non-stick cookware and waterproof clothing) and Bisphenol A (BPA) from plastics are known to interfere with thyroid hormone transport proteins. These chemicals do not just "toxify" the body; they structurally mimic hormones, docking into receptors and sending false signals or blocking legitimate ones.
Heavy Metals
Exposure to Mercury (often from "silver" dental amalgams still prevalent in older UK generations) and Cadmium (from industrial pollution and cigarette smoke) is particularly damaging. Mercury has an incredibly high affinity for Selenium. By binding to selenium, it robs the body of the raw material needed to produce the Deiodinase enzymes. Without selenium, you cannot convert T4 to T3, regardless of how "normal" your TSH looks.
##
##
The Cascade: From Exposure to Disease
The progression from environmental exposure to clinical disease is rarely overnight. It is a slow, erosive cascade that begins with oxidative stress.
The Inflammation Loop
When the thyroid is under siege from halogens or heavy metals, it produces Reactive Oxygen Species (ROS). Under normal circumstances, an enzyme called Thyroid Peroxidase (TPO) uses hydrogen peroxide to "glue" iodine onto a protein called Thyroglobulin to make hormones. However, if the body lacks antioxidants (like glutathione or selenium), this hydrogen peroxide leaks, damaging the thyroid tissue itself.
This damage exposes internal thyroid proteins to the immune system. The immune system, seeing these damaged proteins as foreign invaders, begins to produce Antibodies (TPOAb and TgAb). This is the beginning of Hashimoto’s Thyroiditis, the leading cause of hypothyroidism in the UK.
The Gut-Thyroid Axis
In the UK, the prevalence of intestinal permeability, or "leaky gut," is skyrocketing due to a diet high in ultra-processed foods and the overuse of antibiotics and NSAIDs (like Ibuprofen). When the gut lining is compromised, undigested food particles and bacterial endotoxins (Lipopolysaccharides or LPS) enter the bloodstream. LPS is a potent trigger for systemic inflammation, which directly suppresses the conversion of T4 to T3 in the liver. Furthermore, approximately 20% of T4 to T3 conversion happens in the gut, facilitated by healthy gut bacteria. If the microbiome is dysbiotic (imbalanced), this 20% of potential energy is lost.
Biological Fact: Chronic gut inflammation increases the production of Cortisol. High cortisol levels further inhibit the D1 enzyme and stimulate the D3 enzyme, creating a "perfect storm" of low T3 and high rT3.
##
##
What the Mainstream Narrative Omits
The NHS narrative suggests that hypothyroidism is a simple "on/off" switch controlled by the pituitary. If TSH is high, the switch is "off," and you need pills. If TSH is low or normal, the switch is "on," and you are fine. This binary view omits three critical realities:
1. The Reference Range Fallacy
The "normal" range for TSH in the UK is typically between 0.4 and 4.5 or 5.0 mU/L. This range is based on a statistical average of the population. However, the "population" includes many people with undiagnosed thyroid issues. Functional medicine and many international endocrinology associations suggest that a healthy TSH (the "optimal" range) is actually between 0.5 and 2.0 mU/L. A person with a TSH of 4.2 is often told they are "normal," yet they may be functioning at only 50% of their metabolic capacity.
2. The Failure to Test Antibodies
The NHS rarely tests for TPO or Tg antibodies unless a patient already has an abnormal TSH. This is a catastrophic oversight. Autoimmune destruction of the thyroid can begin decades before the TSH ever rises. A patient can have "perfect" TSH and T4, but if their antibodies are in the hundreds, their immune system is actively dismantling their thyroid gland. This causes "swinging" symptoms—episodes of anxiety and palpitations followed by crashes into fatigue—as the dying gland leaks bursts of hormone into the blood.
3. The Nutritional Gap
The UK is technically "iodine sufficient" on paper, but this is largely due to the fortification of cow’s milk. With the rise of veganism and plant-based milks (which are often not fortified with iodine or selenium), we are seeing a resurgence of iodine deficiency. Furthermore, UK soils are notoriously depleted of Selenium, a mineral essential for the protection of the thyroid and the conversion of its hormones. The NHS does not routinely screen for these nutritional co-factors, treating the thyroid as if it operates in a vacuum.
##
##
The UK Context
Why is the UK specifically struggling with this diagnostic bottleneck? The answer lies in the structure and funding of the NHS.
NICE Guidelines and Financial Gatekeeping
NICE guidelines are designed to provide cost-effective care for a population of 67 million. Measuring TSH is cheap (pennies per test). Measuring Free T3, Reverse T3, and Antibodies is expensive (pounds per test). When multiplied by millions of patients, the cost is significant. Therefore, labs are instructed to use Reflex Testing: they only test T4 if TSH is outside the range, and they almost never test T3.
This creates a "Catch-22." A GP cannot diagnose T3-conversion issues because they aren't allowed to order the test, and they aren't allowed to order the test because the TSH is normal.
The 10-Minute Appointment
Thyroid health is complex and requires a holistic view of diet, stress, environmental exposure, and family history. The standard 10-minute GP appointment is insufficient for this level of investigation. It is far easier for a time-pressured clinician to rely on a computer-generated "Normal" result than to investigate the nuances of cellular hormone resistance.
The Levothyroxine Monoculture
In the UK, the only widely available treatment on the NHS is Levothyroxine (synthetic T4). Natural Desiccated Thyroid (NDT) or Liothyronine (synthetic T3) are virtually impossible to get on a standard prescription due to their higher cost and the medical establishment's outdated fears regarding T3's effect on the heart. By only having one tool (T4), the system has a vested interest in only recognising one problem (T4 deficiency as reflected by high TSH).
##
##
Protective Measures and Recovery Protocols
If you suspect you are part of the "missed millions," you cannot wait for the system to change. You must take an active role in your biological advocacy.
1. Demand a Full Panel (or Go Private)
To get a true picture of thyroid health, you require more than a TSH test. You must insist on, or privately procure, a panel that includes:
- —TSH
- —Free T4
- —Free T3 (The most important marker for how you actually feel)
- —Reverse T3 (To check for conversion "braking")
- —TPO and Tg Antibodies (To rule out Hashimoto's)
- —Vitamin D, B12, Ferritin (Iron), and Folate (These are critical for thyroid hormone transport and utilization)
2. Optimise Nutrient Co-factors
The enzymes that manage your thyroid hormones are "worker bees" that need specific tools:
- —Selenium (200mcg/day): Critical for T4 to T3 conversion and reducing TPO antibodies. (Brazil nuts are a good source, but levels vary by soil).
- —Iodine: Be cautious. While necessary, taking high-dose iodine if you have Hashimoto's can "fuel the fire" of autoimmunity. Always test levels via a urinary loading test first.
- —Zinc and Magnesium: Essential for the TRH/TSH signalling process.
- —Iron: If your Ferritin is below 70-90 ng/mL, your body cannot effectively use thyroid hormone. Many UK women are "within range" for iron but functionally deficient for thyroid health.
3. Environmental Mitigation
- —Water Filtration: Use a high-quality filter (like a Berkey or a reverse osmosis system) that specifically removes Fluoride and Chlorine.
- —Goitrogen Awareness: Avoid large amounts of raw cruciferous vegetables (kale, broccoli) if you have an iodine deficiency, as they contain goitrogenic compounds. Cooking these vegetables neutralises most of the effect.
- —Detoxify the Home: Switch to "fragrance-free" and "paraben-free" personal care products to reduce the burden of endocrine disruptors.
4. Stress and Cortisol Management
Since high cortisol triggers the conversion of T4 into the "dead-end" Reverse T3, stress management is not a luxury; it is a metabolic necessity. This includes prioritising circadian rhythm (morning sunlight exposure) and reducing the intake of stimulants like caffeine, which can mimic stress signals to the HPT axis.
##
##
Summary: Key Takeaways
The current NHS approach to thyroid health is a failure of modern medicine to integrate known biochemical truths. By relying on a single, upstream marker (TSH), the system ignores the downstream reality of cellular function.
- —TSH is a pituitary hormone, not a thyroid hormone. It does not reflect the concentration of active T3 in your brain, heart, or liver.
- —The "Normal Range" is not the "Optimal Range." Being at the high end of the TSH range or the low end of the T3 range is a recipe for chronic illness.
- —Conversion is key. If you take Levothyroxine (T4) but cannot convert it to T3, you will remain symptomatic. This is often due to inflammation, nutrient deficiencies, or high stress (rT3).
- —Autoimmunity must be screened. Hashimoto’s can exist for years with a normal TSH, slowly destroying the gland while the patient suffers.
- —Environmental toxins matter. Fluoride, bromide, and endocrine disruptors are actively competing with your thyroid hormones.
The "Normal" result is the end of the conversation for the NHS, but it should be the beginning of the investigation for you. We must move beyond the TSH-only model to a comprehensive, cellular-focused understanding of thyroid health. Only then can the millions currently suffering in the shadows of the "normal range" reclaim their energy, their cognitive function, and their lives. The truth is not in the lab report; the truth is in your biology.
This article is provided for informational and educational purposes only. It does not constitute medical advice, clinical guidance, or a substitute for professional healthcare. Information reflects cited research at time of publication. Always consult a qualified healthcare professional before acting on any health information.
RESEARCH FOUNDATIONS
Biological Credibility Archive
Citations provided for educational reference. Verify via PubMed or institutional databases.
Medical Disclaimer
The information in this article is for educational purposes only and does not constitute medical advice, diagnosis, or treatment. Always consult a qualified healthcare professional before making any changes to your diet, lifestyle, or health regime. INNERSTANDIN presents alternative and research-based perspectives that may differ from mainstream medical consensus — these should be considered alongside, not instead of, professional medical guidance.
Read Full DisclaimerReady to learn more?
Continue your journey through our classified biological research.
DISCUSSION ROOM
Members of THE COLLECTIVE discussing "Why the NHS Reliance on TSH Testing Leaves Millions Hypothyroid"
SILENT CHANNEL
Be the first to discuss this article. Your insight could help others understand these biological concepts deeper.
THE ARSENAL
Based on NHS Misdiagnosis Patterns — products curated by our research team for educational relevance and biological support.
Lugol’s Iodine – Hormonal Issues, Menopause, Immune System, Brain Fog, Memory, Thyroid, Dry Skin
Rejuvenation Pack – Essential Vitamins and Minerals for Health Restoration
INNERSTANDING may earn a commission on purchases made through these links. All products are selected based on rigorous educational relevance to our biological research.
RABBIT HOLE
Follow the biological thread deeper