Thyroid Resistance: Why Your TSH Might Be Normal While You Are Not
Thyroid dysfunction is frequently misdiagnosed due to an over-reliance on TSH testing which fails to account for cellular hormone utilization. This article explains the difference between hormone production and conversion, and how to advocate for better testing.

# Thyroid Resistance: Why Your TSH Might Be Normal While You Are Not
Overview
The modern landscape of endocrinology is haunted by a silent, systemic failure—a failure not of the biological organism itself, but of the diagnostic framework used to assess it. Millions of individuals across the United Kingdom and globally are trapped in a biological purgatory: they present with classic symptoms of hypothyroidism—debilitating fatigue, cognitive decline, refractory weight gain, and persistent cold intolerance—yet are dismissed by their clinical practitioners because their Thyroid Stimulating Hormone (TSH) levels fall within the so-called "normal" reference range.
This phenomenon is what we term Thyroid Resistance, or more accurately, Type 2 Hypothyroidism. It represents a state where the thyroid gland may be producing sufficient hormones, but the peripheral tissues and cells are unable to utilise them. The current medical paradigm, dictated largely by cost-efficiency and rigid NICE (National Institute for Health and Care Excellence) guidelines, relies almost exclusively on TSH as the "gold standard" for thyroid health. However, TSH is not a thyroid hormone; it is a pituitary hormone. Relying on it to determine cellular thyroid status is akin to checking the thermostat in the hallway to decide if the oven in the kitchen is hot enough to bake bread.
The reality that the mainstream narrative avoids is that thyroid function is a multi-stage process involving production, transport, conversion, and cellular uptake. A breakdown at any point beyond the production phase results in clinical symptoms of deficiency, even if the "production signal" (TSH) appears perfect. In this comprehensive investigation, we will expose the mechanisms of thyroid resistance, the biological disruptors that cause it, and why the current diagnostic model is fundamentally flawed.
According to various epidemiological studies and clinical observations, up to 15-20% of the population may suffer from subclinical or cellular thyroid dysfunction that remains undetected by standard TSH-only screening protocols.
---
The Biology — How It Works

Lugol’s Iodine – Hormonal Issues, Menopause, Immune System, Brain Fog, Memory, Thyroid, Dry Skin
A high-potency 12% Lugol’s Iodine solution designed to support thyroid health, metabolic energy, and cognitive clarity. This traditional aqueous blend provides both iodine and potassium iodide to ensure your body has the essential elements needed for hormonal balance and healthy skin.
Vetting Notes
Pending
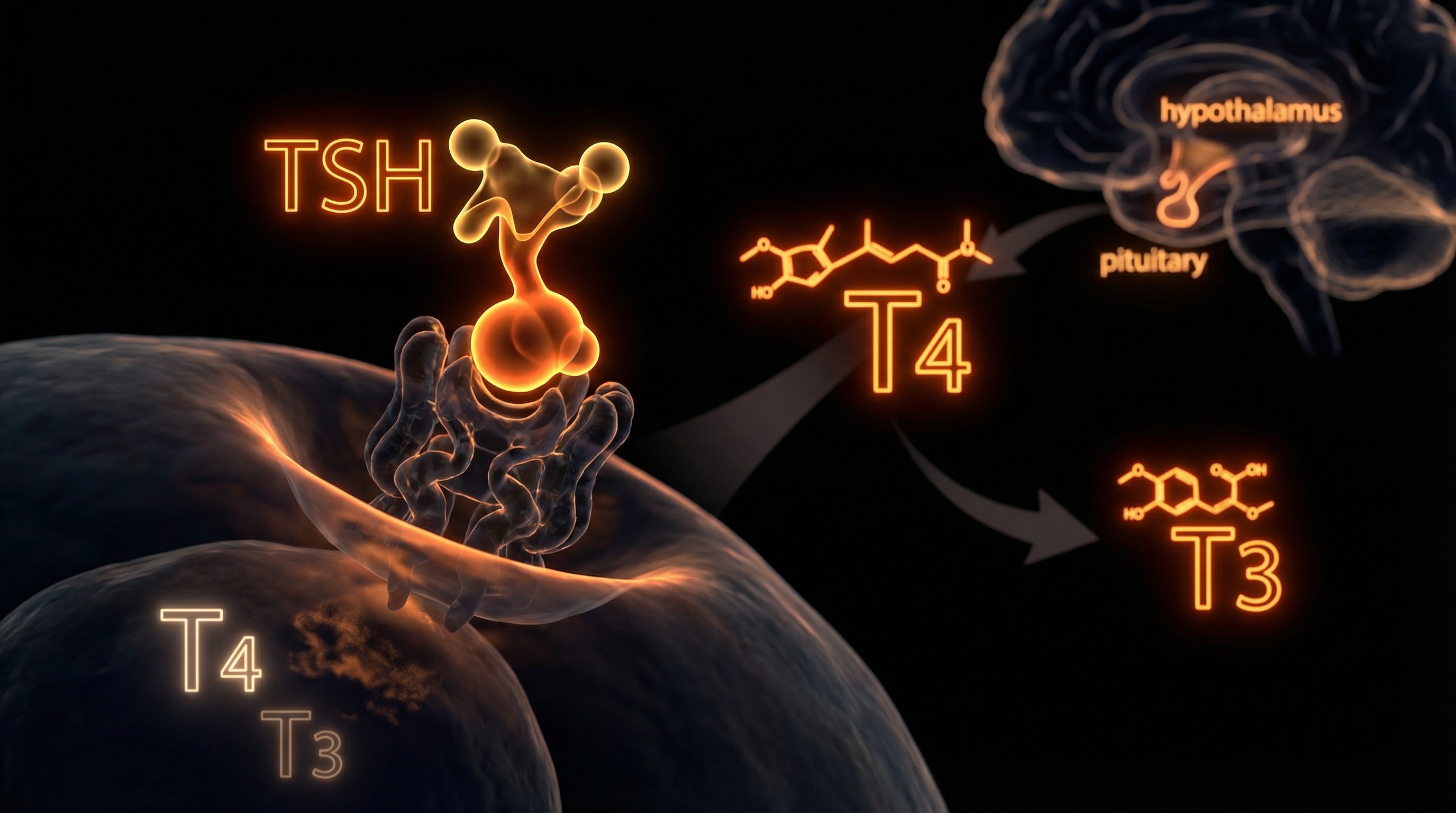
To understand why the system fails, we must first master the intricate dance of the Hypothalamic-Pituitary-Thyroid (HPT) Axis. This is a tightly regulated feedback loop designed to maintain metabolic homeostasis.
The Production Phase
The process begins in the Hypothalamus, which monitors circulating levels of thyroid hormones. When levels are perceived as low, it releases Thyrotropin-Releasing Hormone (TRH). This signals the Anterior Pituitary Gland to secrete Thyroid Stimulating Hormone (TSH). TSH then travels to the thyroid gland (located at the base of the neck), stimulating the production of two primary hormones:
- —Thyroxine (T4): The "pro-hormone." It contains four iodine atoms and is relatively inactive. It makes up about 80-90% of the thyroid's output.
- —Triiodothyronine (T3): The "active hormone." It contains three iodine atoms and is the biological spark plug that drives metabolic rate, body temperature, and cellular repair.
The Transport Phase
Once released into the bloodstream, these hormones do not float freely. Over 99% are bound to carrier proteins, primarily Thyroxine-Binding Globulin (TBG). While bound, they are inactive. Only the "Free" portions—Free T4 (FT4) and Free T3 (FT3)—are available to enter the cells.
The Conversion Phase (The Critical Link)
This is where the mainstream diagnostic model begins to crumble. Because the body produces mostly inactive T4, it must be converted into active T3 in the peripheral tissues—primarily the liver, kidneys, and gut. This conversion is mediated by specific enzymes called Deiodinases.
- —D1 and D2 enzymes strip an iodine atom from T4 to create active T3.
- —D3 enzymes convert T4 into Reverse T3 (rT3)—an isomer that is biologically inactive and acts as a "brake" on the system.
If the conversion of T4 to T3 is impaired, or if T4 is preferentially converted to rT3, a person will experience systemic hypothyroidism regardless of how "normal" their TSH or T4 levels appear.
---
Mechanisms at the Cellular Level
Thyroid resistance occurs when the hormone reaches the cell but cannot execute its function. This is the "Type 2" manifestation of the disease, and it involves the complex machinery of the Thyroid Hormone Receptors (TRs) and the Mitochondria.
The Nuclear Gateway
T3’s primary job is to enter the nucleus of the cell and bind to Thyroid Response Elements (TREs) on the DNA. This binding acts as a genetic switch, "turning on" the transcription of proteins responsible for thermogenesis and energy production. In cases of thyroid resistance, several things can go wrong:
- —Receptor Site Blunting: Just as in insulin resistance, thyroid receptors can become "deaf" to the signal of T3. This can be caused by chronic inflammation, high cortisol, or environmental toxins.
- —The Reverse T3 Blockade: rT3 has a high affinity for T3 receptor sites but lacks the "key" to turn them on. Think of rT3 as a broken key that gets stuck in the lock; the active T3 cannot enter, and the cell remains in a state of metabolic hibernation.
Mitochondrial Bioenergetics
The mitochondria are the "power plants" of the cell, and they are the primary targets for T3. T3 stimulates the production of Adenosine Triphosphate (ATP), the universal energy currency of life. When thyroid signals are blocked at the cellular level:
- —ATP production plummets.
- —The Sodium-Potassium Pump (which consumes a third of our cellular energy) slows down.
- —Body temperature drops (basal metabolic rate decreases).
- —Waste products and cellular debris accumulate because the "cleaning" processes are energy-dependent.
The Deiodinase Disconnect
The pituitary gland uses a specific enzyme (D2 deiodinase) that is highly efficient at converting T4 to T3. However, the rest of the body’s tissues (liver, muscles, brain) rely on a different balance of enzymes. This is the biological "glitch": The pituitary is the last organ to feel the effects of thyroid deficiency.
If you have a conversion issue in your liver, your brain (pituitary) might still be swimming in T3, feeling "fine" and keeping TSH low, while your muscles, heart, and skin are starving for hormone. This is why TSH is an unreliable proxy for total body metabolic status.
---
Environmental Threats and Biological Disruptors
We are living in a world that is increasingly hostile to thyroid physiology. The rise in thyroid resistance is not a genetic accident; it is an environmental consequence. Several "invisible" factors actively sabotage the thyroid at every stage.
The Halogen Competition
On the periodic table, Iodine belongs to the Halogen group. Other halogens include Fluoride, Bromine, and Chlorine. Because they share a similar molecular structure, these toxic halogens compete with iodine for uptake in the thyroid gland and for binding sites on receptors.
- —Fluoride: Ubiquitously added to the water supply in many parts of the UK (under the jurisdiction of local authorities and the Environment Agency), fluoride is a documented thyroid suppressant. It was once used in the mid-20th century as a medication to *treat* hyperthyroidism because of its efficacy in slowing the thyroid down.
- —Bromine (Bromide): Found in "fortified" UK bread as a dough conditioner (potassium bromate) and in flame retardants used in furniture and electronics. Bromide is a potent endocrine disruptor that displaces iodine from the thyroid molecule.
Endocrine Disrupting Chemicals (EDCs)
Our modern environment is saturated with synthetic compounds that mimic or interfere with hormones:
- —Bisphenol A (BPA) and Phthalates: Found in plastics, thermal receipts, and personal care products. These chemicals can bind to thyroid receptors, preventing real T3 from doing its job.
- —PFAS (Per- and Polyfluoroalkyl Substances): Known as "forever chemicals," these are used in non-stick cookware and water-repellent fabrics. They have been linked by the Food Standards Agency (FSA) and global researchers to altered thyroid hormone levels and impaired metabolism.
The Cortisol-Thyroid Axis
In the UK's high-stress, "always-on" culture, chronic elevation of Cortisol (the stress hormone) is a primary driver of thyroid resistance. High cortisol:
- —Inhibits the conversion of T4 to T3.
- —Increases the production of Reverse T3.
- —Decreases the sensitivity of thyroid receptors.
Biological Fact: In a state of chronic stress, the body enters "survival mode." It intentionally slows the metabolism by increasing rT3 to conserve energy for the "fight or flight" response, effectively inducing a state of temporary, protective thyroid resistance.
---
The Cascade: From Exposure to Disease
The progression from environmental exposure to overt disease is a slow, insidious cascade. It rarely happens overnight.
Stage 1: The Compensation Phase
Initially, the body attempts to compensate for environmental stressors. If iodine is low or fluoride is high, the thyroid may slightly enlarge (subclinical goitre) to capture more iodine. TSH may stay within the "normal" range (e.g., 2.0 - 3.0 mIU/L), but the individual begins to feel the first signs of "unexplained" fatigue.
Stage 2: Conversion Failure
As inflammation increases (often due to gut dysbiosis or poor diet), the liver's ability to convert T4 to T3 diminishes. This is where the discrepancy begins. A GP will test TSH and T4, find them "normal," and tell the patient they are depressed or simply "getting older." Meanwhile, the patient's Free T3—the only number that actually matters for energy—is scraping the bottom of the range.
Stage 3: Autoimmune Activation (Hashimoto’s)
When the thyroid gland is under constant stress and dealing with "molecular mimicry" from gluten or environmental toxins, the immune system can become confused. It begins to produce antibodies (such as TPOAb or TGAb) to attack the thyroid tissue. Hashimoto's Thyroiditis is the leading cause of hypothyroidism in the UK. Tragically, the NHS rarely tests for these antibodies until TSH is already significantly elevated, by which point substantial glandular damage has already occurred.
Stage 4: Systemic Metabolic Collapse
Finally, the cellular resistance becomes so severe that the mitochondria can no longer maintain basic functions. This leads to:
- —Hypercholesterolemia: The liver needs T3 to clear LDL cholesterol. "High cholesterol" is often just a symptom of undiagnosed thyroid resistance.
- —Cognitive Decline: The brain is highly dependent on T3 for neurotransmitter production.
- —Cardiovascular Strain: Low T3 weakens the heart muscle's contractility.
---
What the Mainstream Narrative Omits
The refusal to acknowledge thyroid resistance is not merely a scientific oversight; it is a systemic failure rooted in the economics of healthcare and the pharmaceutical industry.
The Reference Range Fallacy
The "normal" range for TSH is calculated based on a statistical average of the population. However, who is having their thyroid tested? Usually, people who are already unwell. By including "unhealthy" people in the average, the range has been stretched far too wide. While the lab range might go up to 4.5 or 5.0 mIU/L, many functional medicine researchers argue that an "optimal" TSH for a healthy person is between 0.5 and 1.5 mIU/L.
The Levothyroxine Monopoly
In the UK, the standard treatment for any thyroid issue is Levothyroxine (synthetic T4). The logic is that the body will simply convert it to T3 as needed. However, if the patient has a conversion issue or thyroid resistance, giving them more T4 is like adding more traffic to a road with a collapsed bridge. It doesn't solve the problem; it often makes it worse by increasing rT3 levels. The more effective treatments—Liothyronine (synthetic T3) or Natural Desiccated Thyroid (NDT)—have been systematically restricted in the UK. Liothyronine was famously subjected to massive price hikes by pharmaceutical companies, leading the NHS to restrict its prescription, leaving thousands of patients without the only medication that worked for them.
The "All in Your Head" Gaslighting
Because the TSH test is treated as infallible, patients with "normal" TSH who still feel unwell are frequently prescribed antidepressants or told to "eat less and move more." This ignores the biological reality that without sufficient cellular T3, it is physiologically impossible to lose weight or maintain a stable mood.
---
The UK Context
The struggle for thyroid health in the United Kingdom is unique due to the centralised nature of the NHS and the specific regulatory environment governed by the MHRA (Medicines and Healthcare products Regulatory Agency).
The Postcode Lottery
Access to comprehensive thyroid testing (Free T3, rT3, and Antibodies) is often a "postcode lottery." In many trusts, the lab will "reflexively" cancel a Free T3 test if the TSH comes back normal, regardless of what the GP requested. This prevents the clinician from ever seeing the full picture of cellular resistance.
Fluoridation and the Environment Agency
Large swathes of the UK, including the West Midlands and parts of the North East, have fluoride added to their drinking water. Unlike most of Europe, which has rejected water fluoridation, the UK government continues this practice. For an individual with a genetic predisposition to thyroid resistance, this daily "dose" of a known goitrogen can be the tipping point into chronic illness.
The NICE Guidelines Constraint
NHS doctors are strictly bound by NICE guidelines, which prioritise "cost-effectiveness" over individualised biochemical markers. These guidelines currently do not support the routine testing of rT3 or the use of T3-containing medications as a first-line or even second-line treatment, despite the biological evidence that T4-only monotherapy fails a significant percentage of the population.
Fact: In 2017, the cost of Liothyronine to the NHS rose from approximately £15 per pack to over £250, leading to a "crackdown" on its use that ignored clinical necessity in favour of budgetary management.
---
Protective Measures and Recovery Protocols
If you suspect you are suffering from thyroid resistance, you must become your own biological advocate. The path to recovery involves bypassing the "standard of care" and addressing the cellular environment.
1. Advanced Diagnostics
Do not settle for a TSH test. You must insist on, or privately source, a full thyroid panel:
- —TSH: (Looking for an optimal 0.5 - 1.5)
- —Free T4 and Free T3: To check conversion efficiency.
- —Reverse T3 (rT3): To check for cellular blocking.
- —Thyroid Antibodies (TPOAb, TGAb): To rule out Hashimoto’s.
- —Vitamin D, B12, Ferritin, and Selenium: These are essential co-factors for thyroid function.
2. Nutritional Fortification
- —Selenium: Essential for the deiodinase enzymes that convert T4 to T3. Two Brazil nuts a day or a 200mcg supplement can significantly improve conversion.
- —Iodine: Crucial, but must be used with caution. If you have Hashimoto's, starting high-dose iodine can "fire up" the autoimmune attack. Always test your levels first.
- —Zinc and Magnesium: Required for receptor sensitivity and ATP production.
- —Avoid Goitrogens and Halogens: Filter your water (using Reverse Osmosis or specialised filters to remove fluoride) and choose organic, bromide-free breads.
3. Healing the Liver and Gut
Since 80% of T4-to-T3 conversion happens outside the thyroid, your liver and gut health are paramount.
- —Reduce alcohol and processed seed oils to lower liver inflammation.
- —Support the microbiome with diverse fibres and fermented foods, as the gut enzyme intestinal sulfatase converts inactive T3-sulfate back into active T3.
4. Stress Management and Cortisol Control
Lowering rT3 requires convincing the body it is no longer in danger.
- —Circadian Biology: View morning sunlight to regulate the hypothalamus.
- —Adaptogens: Herbs like Ashwagandha (carefully, as it can stimulate the thyroid) or Holy Basil can help modulate the stress response.
- —Sleep: Deep sleep is the primary time for metabolic repair.
5. Advocacy within the NHS
When speaking to a GP:
- —Use phrases like "clinical symptoms of hypothyroidism persist despite T4 therapy."
- —Reference the British Thyroid Association guidelines which do allow for T3 trials in specific "unmet need" cases.
- —If necessary, seek a referral to an endocrinologist who specialises in "bio-identical" or "combination" therapy.
---
Summary: Key Takeaways
The current medical approach to thyroid health is dangerously reductive. By focusing solely on the TSH, the system ignores the complex, multi-stage journey thyroid hormones must take to actually produce energy in your cells.
- —TSH is a Pituitary Signal, Not a Cellular Measure: You can have a perfect TSH while your cells are starving for T3.
- —Conversion is King: If your body cannot convert T4 to T3, or if it is producing too much Reverse T3, you will remain hypothyroid regardless of your Levothyroxine dose.
- —Environmental Sabotage is Real: Fluoride, bromide, and EDCs are active participants in the UK's thyroid epidemic.
- —The "Normal" Range is Not the "Optimal" Range: Statistical averages include the sick. Aim for functional, optimal levels.
- —Biochemical Sovereignty: You have the right to investigate your own biology beyond the basic NHS TSH screen.
Thyroid resistance is not a life sentence; it is a signal that the cellular environment is out of balance. By identifying the specific point of failure—whether it be conversion, receptor sensitivity, or toxic interference—you can reclaim your metabolism and your vitality from a system that is currently content to leave you in the dark.
This article is provided for informational and educational purposes only. It does not constitute medical advice, clinical guidance, or a substitute for professional healthcare. Information reflects cited research at time of publication. Always consult a qualified healthcare professional before acting on any health information.
RESEARCH FOUNDATIONS
Biological Credibility Archive
Citations provided for educational reference. Verify via PubMed or institutional databases.
Medical Disclaimer
The information in this article is for educational purposes only and does not constitute medical advice, diagnosis, or treatment. Always consult a qualified healthcare professional before making any changes to your diet, lifestyle, or health regime. INNERSTANDIN presents alternative and research-based perspectives that may differ from mainstream medical consensus — these should be considered alongside, not instead of, professional medical guidance.
Read Full DisclaimerReady to learn more?
Continue your journey through our classified biological research.
DISCUSSION ROOM
Members of THE COLLECTIVE discussing "Thyroid Resistance: Why Your TSH Might Be Normal While You Are Not"
SILENT CHANNEL
Be the first to discuss this article. Your insight could help others understand these biological concepts deeper.
THE ARSENAL
Based on Hormonal Health — products curated by our research team for educational relevance and biological support.

Magnesium Blend – The Most Important Mineral
Rejuvenation Pack – Essential Vitamins and Minerals for Health Restoration

Magnesium L-Threonate
INNERSTANDING may earn a commission on purchases made through these links. All products are selected based on rigorous educational relevance to our biological research.
RABBIT HOLE
Follow the biological thread deeper