Anti-Vinculin Antibodies: The Autoimmune Origin of IBS-D
Modern testing now allows for the detection of anti-vinculin antibodies, proving that many cases of 'functional' IBS are actually post-infectious autoimmune conditions. This discovery shifts the treatment focus from symptoms to immune modulation.
Overview
For decades, the medical establishment has relegated Irritable Bowel Syndrome (IBS) to the dustbin of "functional" disorders—a polite clinical euphemism for "we don’t know what is wrong, so it must be psychosomatic." Millions of patients, particularly in the United Kingdom, have been dismissed by General Practitioners with advice to "reduce stress" or "eat more fibre," while their lives are decimated by debilitating urgency, chronic bloating, and systemic fatigue. However, a seismic shift in gastroenterological research has finally unmasked the culprit. We now know that for a vast majority of those suffering from the diarrhoea-predominant subtype (IBS-D), the condition is not a vague functional malaise but a measurable, post-infectious autoimmune disease.
The discovery of anti-vinculin antibodies represents the "smoking gun" in the landscape of gut health. This biomarker proves that a single episode of acute gastroenteritis—food poisoning—can trigger a molecular cascade that turns the body’s immune system against its own enteric nervous system. The implications are profound: IBS-D is often an autoimmune injury to the gut’s "pacemaker" cells. This transition from a diagnosis of exclusion to a diagnosis of organic pathology changes everything. It shifts the therapeutic focus from the futile management of symptoms to the sophisticated modulation of the immune system and the restoration of intestinal motility.
At INNERSTANDING, we view this as a pivotal moment in biological medicine. The identification of anti-vinculin and its precursor, anti-CdtB (Cytolethal Distending Toxin B), allows us to move beyond the superficial narrative of "gut dysbiosis" and into the realm of structural proteomics. We are no longer guessing. We are witnessing the mechanical failure of the Migrating Motor Complex (MMC) due to an autoimmune assault. This article serves as the definitive guide to understanding how a common bacterial toxin can rewire your biology, leading to a lifetime of gastrointestinal distress, and more importantly, how we can begin to reverse the damage.
##
The Biology — How It Works
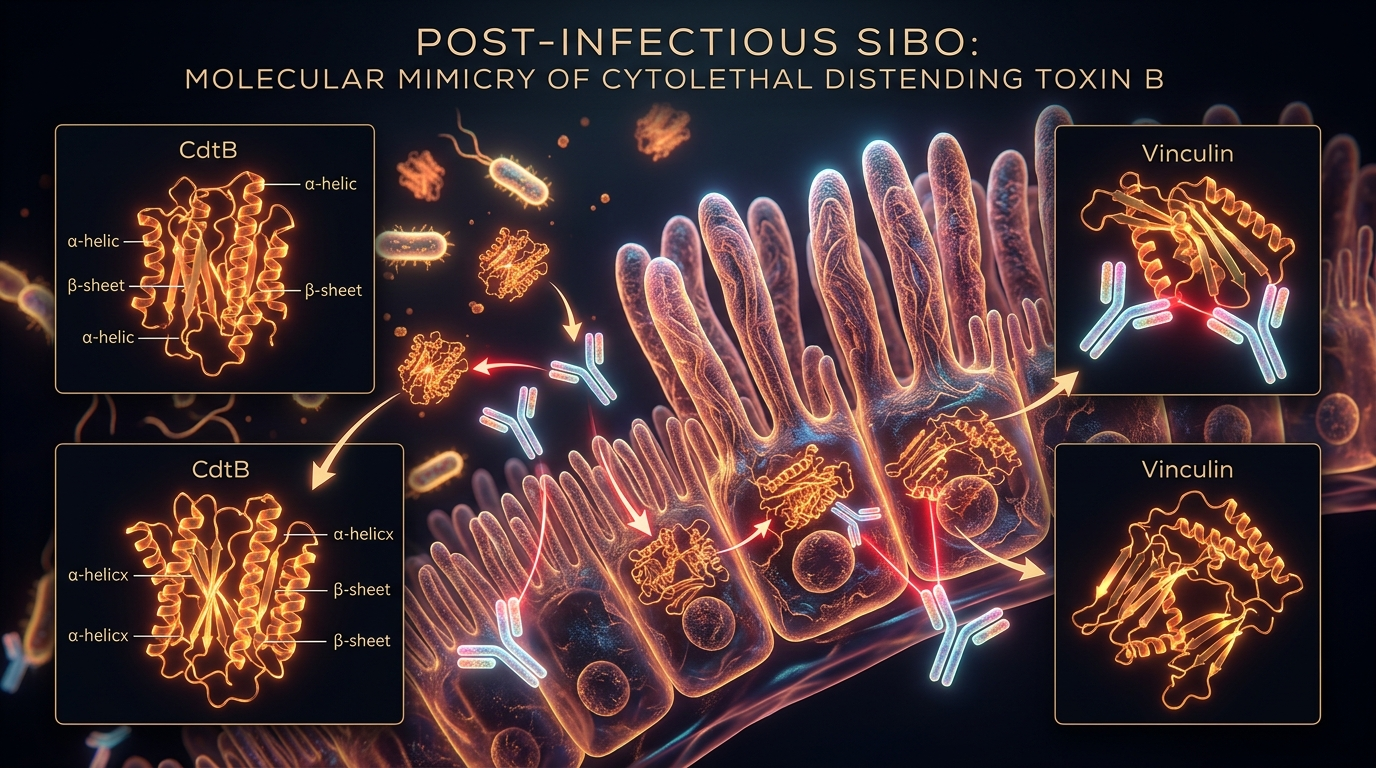
To understand the autoimmune origin of IBS-D, one must first understand the concept of molecular mimicry. This is a biological "case of mistaken identity" where the immune system, in its zeal to protect the host from an external pathogen, develops antibodies that accidentally target the body’s own proteins because they share a similar molecular sequence.
The process begins with an exposure to specific Gram-negative bacteria. The most common offenders are *Campylobacter jejuni* (the UK’s leading cause of food poisoning), *Salmonella*, *Shigella*, and certain strains of *Escherichia coli*. These bacteria produce a potent virulence factor known as Cytolethal Distending Toxin B (CdtB). When these pathogens invade the intestinal mucosa, the innate immune system identifies CdtB as a high-priority threat. The body responds by producing B-cells that secrete highly specific anti-CdtB antibodies to neutralise the toxin.
However, a critical biological complication arises. The molecular structure of CdtB bears a striking resemblance to a human protein called vinculin. Vinculin is an essential actin-binding protein found in the cytoplasm of mammalian cells. It plays a foundational role in cell-to-cell adhesion and the maintenance of the cytoskeleton. Specifically, in the gastrointestinal tract, vinculin is a key component of the Interstitial Cells of Cajal (ICC) and the enteric neurons that coordinate movement.
When the levels of anti-CdtB antibodies remain elevated—often due to repeated exposures or a hyper-reactive immune response—they begin to cross-react with vinculin. The immune system, unable to distinguish between the bacterial toxin and the structural proteins of the gut, begins to attack the vinculin within the intestinal lining. This is the moment a transient infection transforms into a chronic autoimmune condition. The presence of these anti-vinculin antibodies leads to the degradation of the cellular architecture required for normal peristalsis, effectively crippling the "second brain" of the gut.
UK Statistic: Public Health England reports over 500,000 cases of food poisoning annually, yet it is estimated that only 1 in 10 cases are officially recorded. This suggests a massive, hidden reservoir of potential autoimmune IBS triggers within the British population.
##
Mechanisms at the Cellular Level
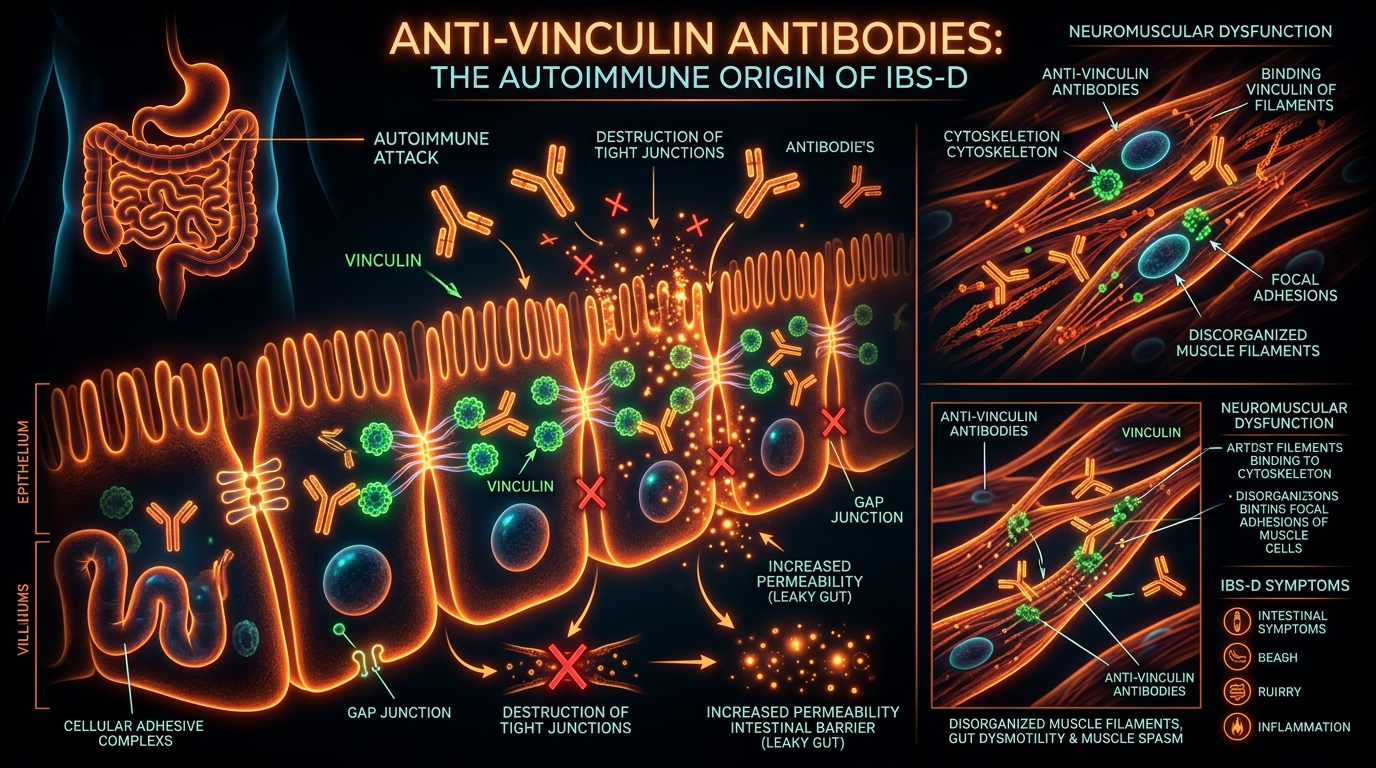
The damage caused by anti-vinculin antibodies is not merely superficial; it occurs at the microscopic junctions where cells communicate. Vinculin is a 117-kDa protein that acts as a physical bridge between the actin cytoskeleton and the extracellular matrix. It is concentrated at focal adhesions and adherens junctions. Without functional vinculin, cells lose their structural integrity and their ability to transmit mechanical signals.
The Destruction of the Interstitial Cells of Cajal (ICC)
The Interstitial Cells of Cajal are frequently described as the "pacemakers" of the gut. They are responsible for generating the electrical "slow waves" that trigger smooth muscle contractions. In a healthy gut, these waves ensure that food and bacteria are moved efficiently through the small intestine and into the colon.
When anti-vinculin antibodies target these cells, the ICCs undergo apoptosis (programmed cell death) or become severely dysfunctional. The loss of ICC density is a hallmark of post-infectious IBS. As the pacemaker population thins, the electrical signalling becomes erratic or non-existent. This leads to a breakdown of the Migrating Motor Complex (MMC)—the "cleansing wave" that occurs during fasting states.
The Failure of the Migrating Motor Complex (MMC)
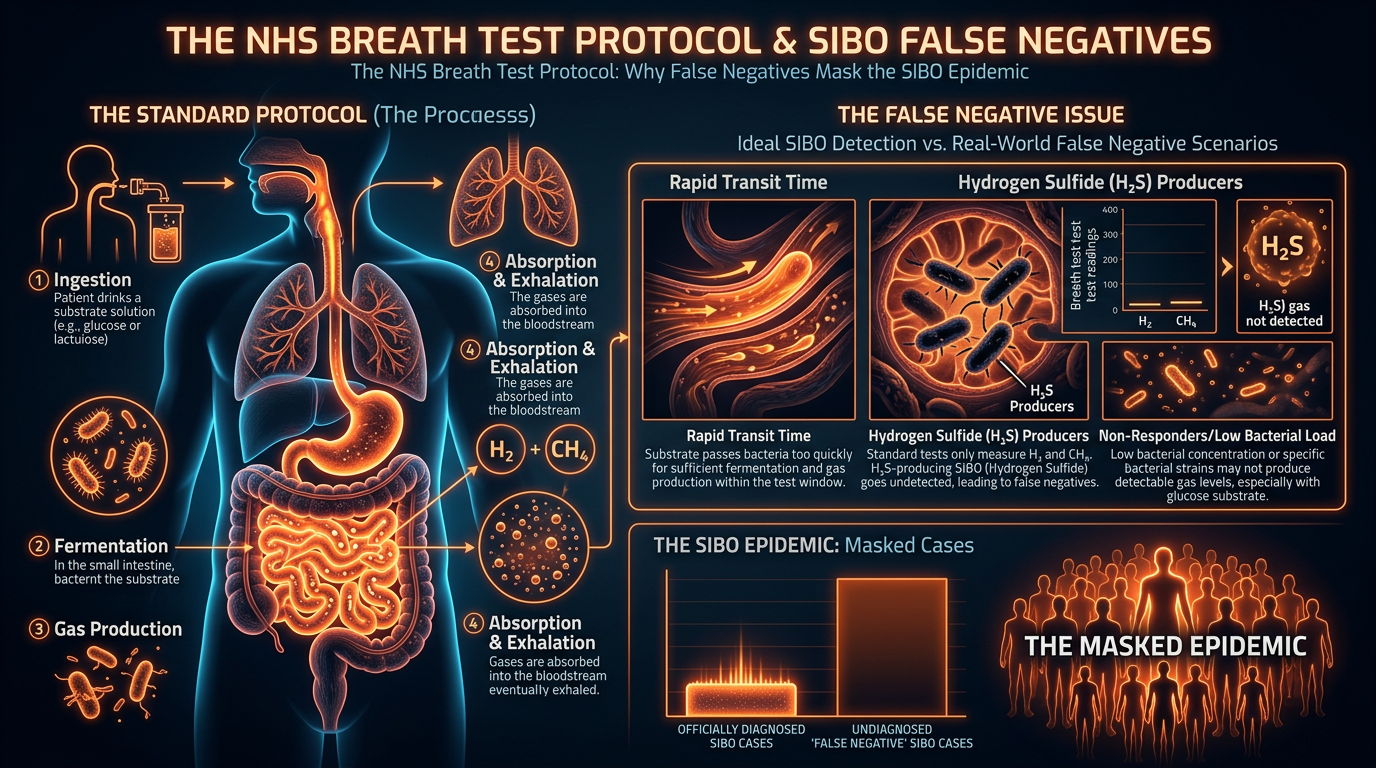
The MMC is a distinct pattern of electromechanical activity that acts as a "sweeper" for the small intestine. It usually occurs every 90 to 120 minutes between meals. Its primary biological function is to clear out undigested food debris and, crucially, to prevent colonic bacteria from migrating upwards into the small intestine.
When anti-vinculin antibodies disrupt the vinculin-dependent scaffolding of the enteric nervous system, the MMC fails. This creates a state of intestinal stasis. In this stagnant environment, bacteria that belong in the large intestine begin to colonise the small intestine, where they ferment carbohydrates, produce gases (hydrogen and methane), and cause the classic symptoms of Small Intestinal Bacterial Overgrowth (SIBO). Thus, SIBO is often not the primary disease, but a secondary consequence of the autoimmune destruction of the MMC's structural proteins.
Epithelial Barrier Dysfunction
Beyond the nervous system, vinculin is also vital for the integrity of the intestinal epithelial barrier. The "tight junctions" that prevent toxins and undigested proteins from entering the bloodstream rely on a stable cytoskeleton. When anti-vinculin antibodies interfere with these structural proteins, the gut becomes "leaky" (increased intestinal permeability). This allows Lipopolysaccharides (LPS)—pro-inflammatory endotoxins from bacterial cell walls—to enter the systemic circulation, further driving the autoimmune cycle and causing systemic symptoms like brain fog and joint pain.
##
Environmental Threats and Biological Disruptors
The rise in anti-vinculin mediated IBS-D cannot be viewed in isolation. It is exacerbated by a modern environment that is increasingly hostile to the delicate balance of the human microbiome and the enteric nervous system.
- —The Ubiquity of Glyphosate: In the UK, glyphosate remains a widely used herbicide in industrial agriculture. Research suggests that glyphosate can act as a "pathway opener," disrupting the tight junctions of the gut and making it easier for CdtB toxins to penetrate the mucosal layer and trigger an immune response.
- —Over-prescription of Proton Pump Inhibitors (PPIs): By suppressing stomach acid, PPIs remove the first line of defence against food-borne pathogens. This increases the likelihood of a high-load bacterial infection, providing the "antigenic load" necessary to trigger the production of anti-CdtB and anti-vinculin antibodies.
- —Ultra-Processed Foods (UPFs): The British diet is among the highest in Europe for UPF consumption. Emulsifiers and artificial sweeteners found in these foods have been shown to degrade the protective mucus layer of the gut. A thinned mucus layer provides a direct gateway for pathogens like *Campylobacter* to reach the epithelial cells and release CdtB.
- —Chronic Stress and the HPA Axis: While stress does not *cause* anti-vinculin antibodies, it acts as a biological accelerant. Chronic activation of the sympathetic nervous system inhibits the MMC and alters the gut's immune environment, making the body more prone to maintaining high antibody titres rather than clearing them.
Biological Fact: The small intestine contains approximately 70-80% of the body's immune cells. When this area is compromised by an autoimmune attack on vinculin, the entire systemic immune profile shifts toward a pro-inflammatory state.
##
The Cascade: From Exposure to Disease
The progression from a simple "stomach bug" to a chronic autoimmune condition follows a predictable biological timeline. Understanding this cascade is essential for both diagnosis and intervention.
Phase 1: The Initial Insult
The individual consumes contaminated food or water. Pathogens like *Salmonella* or *Campylobacter* colonise the small intestine. The person experiences "typical" food poisoning symptoms: vomiting, diarrhoea, and abdominal cramps. Most people "recover" within 48 to 72 hours and believe the incident is over.
Phase 2: The Latent Autoimmune Trigger
While the acute symptoms vanish, the immune system has been primed. In genetically susceptible individuals, the B-cells continue to produce antibodies against the CdtB toxin. Because of molecular mimicry, these antibodies begin to recognize and bind to vinculin on the Interstitial Cells of Cajal.
Phase 3: The Slow Decay of Motility
Over the following 3 to 12 months, the density of functional ICCs begins to decline. The Migrating Motor Complex weakens. The person may notice they are slightly more bloated than usual or that their bowel movements are becoming less predictable. They often attribute this to "getting older" or "a change in diet."
Phase 4: SIBO Colonisation
As the "sweeper waves" fail, the small intestine becomes a stagnant pond. Bacteria from the colon move upstream. They feast on starches and sugars, producing hydrogen gas. This gas distends the small intestine (which is not designed to hold gas), causing intense bloating, pain, and—due to the osmotic effect and irritation—urgent, watery diarrhoea.
Phase 5: The Chronic State (IBS-D)
The patient is now in a state of chronic SIBO and autoimmune-driven dysmotility. They visit their GP, undergo a colonoscopy (which comes back "normal" because the damage is microscopic and functional), and are eventually diagnosed with IBS. By this point, the anti-vinculin antibodies are often circulating at high levels, ensuring that even if the SIBO is treated with antibiotics, it will return, because the underlying "motor" is still broken.
##
What the Mainstream Narrative Omits
The current standard of care for IBS in the UK is woefully outdated. The NHS "NICE" guidelines still largely focus on the Bristol Stool Chart and dietary modifications like the Low FODMAP diet. While these tools have their place, they are essentially band-aids on a gaping wound.
What the mainstream narrative fails to mention is that IBS is often a neurological injury. By focusing exclusively on the "microbiome" or "fibre intake," the medical establishment ignores the structural proteomics of the enteric nervous system. There is a significant reluctance to adopt the IBS-Smart or similar blood tests that measure anti-CdtB and anti-vinculin levels. Why? Because identifying a specific autoimmune cause requires a shift in the pharmaceutical model—from selling indefinite supplies of over-the-counter laxatives or anti-diarrhoeals to a more complex model of immune modulation and prokinetic therapy.
Furthermore, the mainstream narrative often ignores the recursive nature of the infection. Many IBS-D patients are told their "gut is sensitive," when in reality, their low levels of vinculin and weakened MMC make them *more* susceptible to subsequent food poisoning. Each minor "stomach upset" adds fuel to the autoimmune fire, increasing the antibody titres and further destroying the ICCs. This is a vicious cycle that cannot be broken by "mindfulness" or "eating more vegetables."
Critical Fact: Research led by Dr Mark Pimentel has shown that the levels of anti-vinculin antibodies correlate directly with the severity of the IBS symptoms. The higher the antibody count, the more profound the damage to the intestinal motility.
##
The UK Context
The United Kingdom presents a unique set of challenges regarding the autoimmune origin of IBS-D. The prevalence of *Campylobacter*—the primary trigger for these antibodies—is higher in the UK than in many other developed nations, largely due to intensive poultry farming practices.
Furthermore, the NHS structure creates a "diagnostic lag." A patient typically waits months for a gastroenterology referral, only to be offered a colonoscopy. Since anti-vinculin damage is not visible on a standard colonoscopy or biopsy (which focuses on the large intestine and looks for gross inflammation like IBD), the patient is told nothing is wrong. The specialised testing for SIBO (breath testing) and autoimmunity (antibody testing) is rarely available on the NHS, forcing patients into an expensive private sector that is often unregulated and variable in quality.
There is also a cultural element. The "keep calm and carry on" attitude often leads Britons to ignore "minor" digestive issues for years. By the time they seek help, the autoimmune damage to the vinculin proteins may have reached a critical threshold, making recovery a much longer and more arduous process.
- —NHS Waiting Times: Current targets for specialist referrals are often missed, meaning the window for early intervention after food poisoning is frequently lost.
- —Diagnostic Tunnel Vision: The focus remains on excluding Crohn’s Disease and Ulcerative Colitis, leaving the "middle ground" of autoimmune IBS-D largely unaddressed.
- —Public Health Failure: There is a lack of public awareness regarding the long-term autoimmune risks of food poisoning. A "stomach bug" is seen as a rite of passage rather than a potential trigger for a chronic disease.
##
Protective Measures and Recovery Protocols
If anti-vinculin antibodies are the cause, the solution must address the immune system, the structural proteins, and the mechanical motility of the gut. Recovery is not about "killing" bacteria; it is about restoring the "cleansing wave."
1. Accurate Diagnosis via Biomarkers
The first step is to confirm the autoimmune status. Testing for anti-CdtB and anti-vinculin antibodies (such as the IBS-Smart test) is essential. If these are elevated, the patient has a confirmed post-infectious autoimmune IBS. This validates the patient's experience and directs the treatment toward motility rather than just "dysbiosis."
2. Prokinetic Therapy
Since the MMC is compromised, we must manually "jump-start" the motor. Prokinetics are agents that stimulate the 5-HT4 receptors or motilin receptors to induce an MMC wave.
- —Pharmaceutical Prokinetics: Low-dose Naltrexone (LDN) has shown promise in modulating the immune response, while Low-dose Erythromycin or Prucalopride (Resolor) can stimulate the MMC.
- —Natural Prokinetics: High-potency ginger and artichoke extracts are effective for milder cases, helping to encourage the small intestine to clear its contents.
3. The "Spacing" Strategy
The MMC only occurs during fasting. Therefore, "grazing" or eating six small meals a day—the traditional advice for some digestive issues—is catastrophic for an anti-vinculin patient. There must be at least 4 to 5 hours between meals, with no snacking, to allow the weakened MMC to attempt a cleansing wave.
4. Immune Modulation and Mucosal Support
We must calm the B-cell production of antibodies. This involves:
- —Identifying Cross-Reactive Foods: Some patients find that dairy or gluten can exacerbate the immune response through further molecular mimicry.
- —Vagal Nerve Stimulation: The vagus nerve is the "on switch" for the MMC. Techniques such as gargling, deep diaphragmatic breathing, and cold water immersion can help shift the body from a "fight or flight" state to a "rest and digest" state, supporting the enteric nervous system.
- —Immunoglobulins: Oral immunoglobulin therapy (SBI) can help "mop up" CdtB toxins and other antigens in the gut before they can trigger further antibody production.
5. Prevention of Re-infection
For an individual with high anti-vinculin antibodies, one more case of food poisoning could be the "final straw" for their motility. Extreme hygiene, avoiding high-risk foods (undercooked poultry, unwashed salads in restaurants), and using "traveler's probiotics" like *Saccharomyces boulardii* during high-risk exposures are non-negotiable.
##
Summary: Key Takeaways
The revelation that IBS-D is frequently an autoimmune condition rooted in the production of anti-vinculin antibodies represents a turning point in modern medicine. We are moving away from the "functional" myths of the past and into a future of precision gastroenterology.
- —The Root Cause: IBS-D is often triggered by food poisoning. The toxin CdtB mimics the human protein vinculin, leading the immune system to attack the gut's own structural architecture.
- —The Target: The Interstitial Cells of Cajal (ICCs) are destroyed or damaged, leading to the failure of the Migrating Motor Complex (MMC).
- —The Consequence: Without the "cleansing wave" of the MMC, SIBO develops, leading to chronic bloating, pain, and diarrhoea.
- —The Diagnosis: Modern blood tests for anti-CdtB and anti-vinculin antibodies can provide a definitive diagnosis, moving IBS from a "diagnosis of exclusion" to a "diagnosis of inclusion."
- —The Solution: Treatment must focus on stimulating motility through prokinetics, spacing meals to allow the MMC to function, and protecting the gut from further infectious insults.
At INNERSTANDING, we believe that knowledge is the ultimate biological intervention. By understanding the autoimmune origin of IBS-D, patients can stop blaming themselves for a "functional" failure and start addressing the mechanical and immunological reality of their condition. The era of dismissing gut health as "stress" is over; the era of vinculin-focused recovery has begun.
This article is provided for informational and educational purposes only. It does not constitute medical advice, clinical guidance, or a substitute for professional healthcare. Information reflects cited research at time of publication. Always consult a qualified healthcare professional before acting on any health information.
RESEARCH FOUNDATIONS
Biological Credibility Archive
Citations provided for educational reference. Verify via PubMed or institutional databases.
Medical Disclaimer
The information in this article is for educational purposes only and does not constitute medical advice, diagnosis, or treatment. Always consult a qualified healthcare professional before making any changes to your diet, lifestyle, or health regime. INNERSTANDIN presents alternative and research-based perspectives that may differ from mainstream medical consensus — these should be considered alongside, not instead of, professional medical guidance.
Read Full DisclaimerReady to learn more?
Continue your journey through our classified biological research.
DISCUSSION ROOM
Members of THE COLLECTIVE discussing "Anti-Vinculin Antibodies: The Autoimmune Origin of IBS-D"
SILENT CHANNEL
Be the first to discuss this article. Your insight could help others understand these biological concepts deeper.
THE ARSENAL
Based on SIBO & Small Intestine Health — products curated by our research team for educational relevance and biological support.

Panaceum – Prebiotic Oligosaccharide Complex

Magnesium Blend – The Most Important Mineral

Clean Slate – Detoxes thousands of chemicals,heavy metals, pesticides, allergens, mold spores and fungus
INNERSTANDING may earn a commission on purchases made through these links. All products are selected based on rigorous educational relevance to our biological research.
RABBIT HOLE
Follow the biological thread deeper