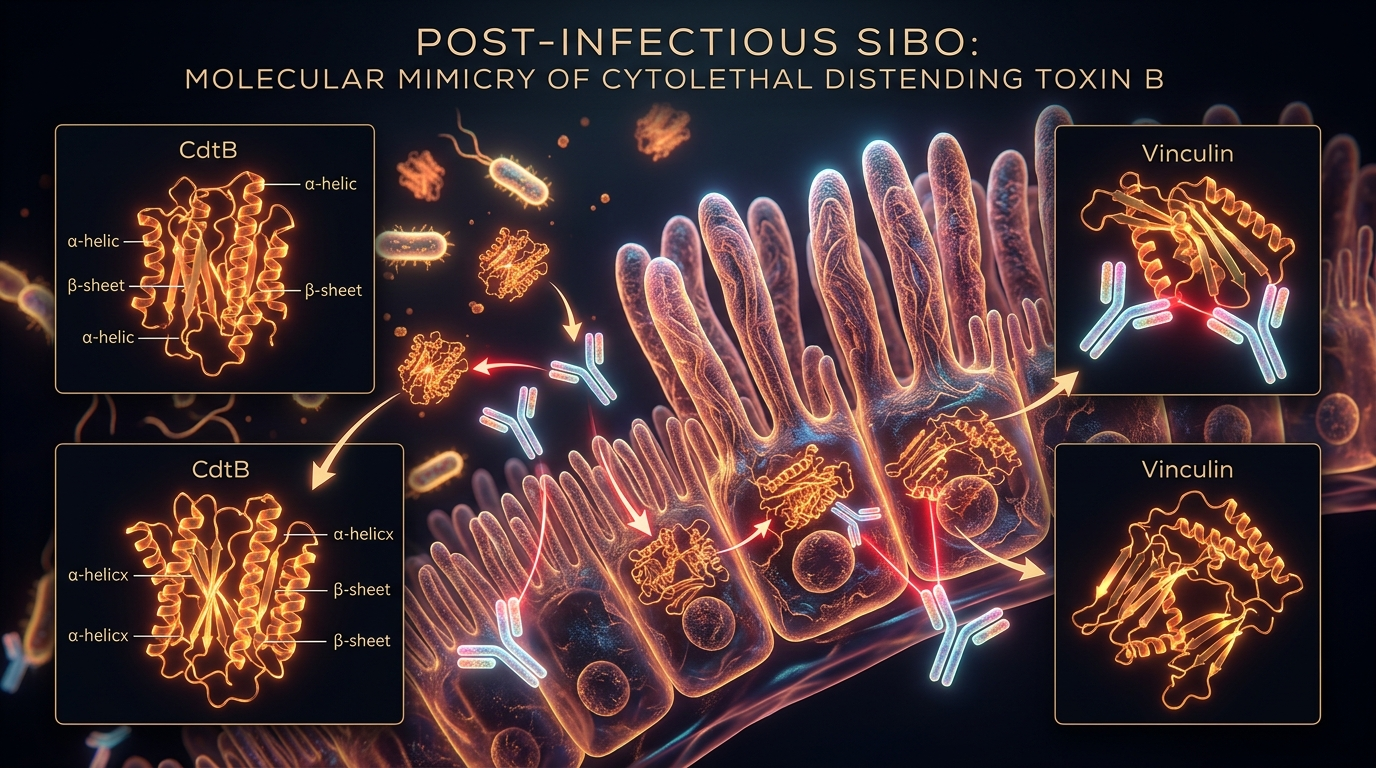
Post-Infectious SIBO: The Molecular Mimicry of Cytolethal Distending Toxin B
Food poisoning can trigger the production of antibodies that mistakenly attack vinculin, a protein essential for intestinal nerve health. This autoimmune response permanently alters the small intestine's ability to clear bacteria.
Overview
The landscape of gastroenterology is undergoing a seismic shift, moving away from the antiquated "wastebasket" diagnosis of Irritable Bowel Syndrome (IBS) towards a precise, molecular understanding of gut dysfunction. For decades, patients presenting with bloating, abdominal pain, and erratic bowel movements were told their condition was psychosomatic—a "functional" disorder of the mind-gut axis that lacked a clear organic cause. We now know this narrative is not only reductive but scientifically inaccurate. At the heart of at least 60% of these cases lies Small Intestinal Bacterial Overgrowth (SIBO), and more specifically, a condition triggered by a common bout of food poisoning: Post-Infectious SIBO (PI-SIBO).
This is not merely a "glitch" in digestion. It is an autoimmune phenomenon driven by a process known as molecular mimicry. When an individual consumes contaminated food—carrying pathogens such as *Campylobacter jejuni*, *Salmonella*, *Shigella*, or *Escherichia coli*—the body is exposed to a specific, highly virulent protein called Cytolethal Distending Toxin B (CdtB). In the desperate rush to neutralise this threat, the immune system produces potent antibodies. However, due to a tragic evolutionary overlap, the CdtB toxin shares structural similarities with vinculin, a crucial protein found within the human enteric nervous system.
The result is a case of mistaken identity with catastrophic consequences. The immune system, having successfully cleared the initial infection, continues to produce antibodies that now target the body’s own tissues. This autoimmune attack damages the Migrating Motor Complex (MMC), the "housekeeper" of the small intestine. When the MMC fails, the small intestine loses its ability to clear residual food and bacteria, leading to a stagnant environment where bacteria from the large intestine can migrate upward and flourish. This article explores the intricate molecular machinery of this process, exposing how a single meal can rewire the gut’s biological blueprint.
In the United Kingdom, it is estimated that over 10 million people suffer from IBS symptoms, yet the vast majority remain unaware that their condition may have been initiated by a single, forgotten episode of gastroenteritis.
---
##
The Biology — How It Works
To understand Post-Infectious SIBO, one must first understand the fundamental mechanics of small intestinal motility. The small intestine is not a passive tube; it is a highly sophisticated, muscular organ that relies on rhythmic, coordinated contractions to maintain homeostasis. The most critical of these movements is the Migrating Motor Complex (MMC).
The Migrating Motor Complex: The Gut’s Housekeeper
The MMC is a distinct pattern of electromechanical activity observed in gastrointestinal smooth muscle during the fasting state. It consists of four phases, with Phase III being the most significant. During Phase III, powerful "clearing waves" sweep through the stomach and small intestine, pushing undigested debris, cellular waste, and, crucially, bacteria toward the colon. This process occurs roughly every 90 to 120 minutes when the stomach is empty.
In a healthy individual, the MMC acts as a biological "reset button." It prevents the accumulation of bacteria in the small intestine, an area that should remain relatively sterile compared to the densely populated large intestine. However, in PI-SIBO, the MMC is not just sluggish; its neurological "wiring" is compromised.
The Pathogenic Trigger: Cytolethal Distending Toxin B
The catalyst for this failure is the Cytolethal Distending Toxin (Cdt). This tri-partite toxin is produced by the major pathogens responsible for food poisoning. The toxin consists of three subunits: CdtA, CdtB, and CdtC. While CdtA and CdtC act as the delivery vehicle, binding to the host cell membrane, CdtB is the "warhead."
Once inside the cell, CdtB migrates to the nucleus, where it acts as a DNase (an enzyme that breaks down DNA). This induces double-strand DNA breaks, causing the cell to arrest its cycle and eventually die or malfunction. While the initial infection might last only a few days, the presence of CdtB in the system triggers a prolonged and aggressive immune response.
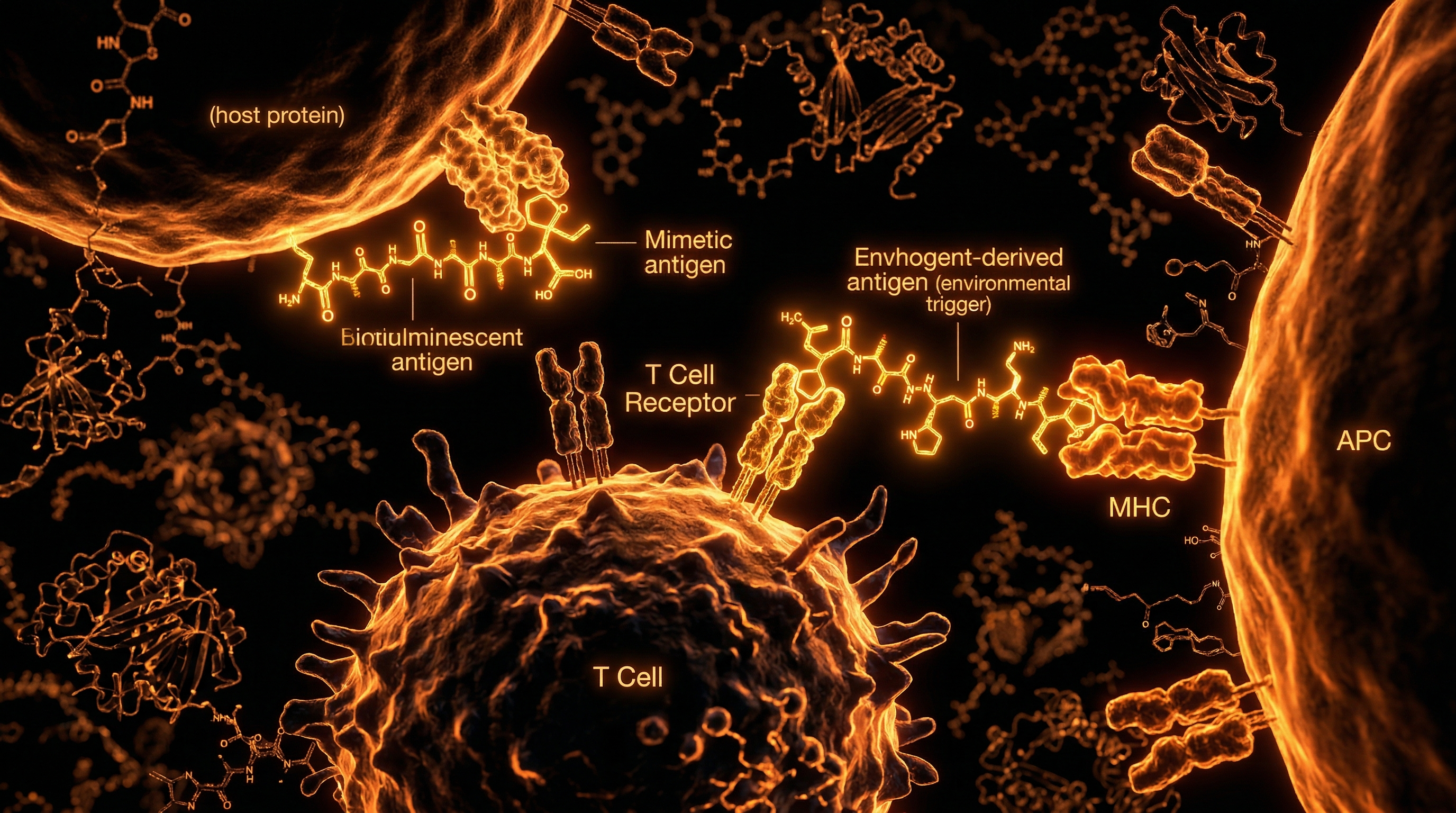
The Autoimmune Cross-Reaction
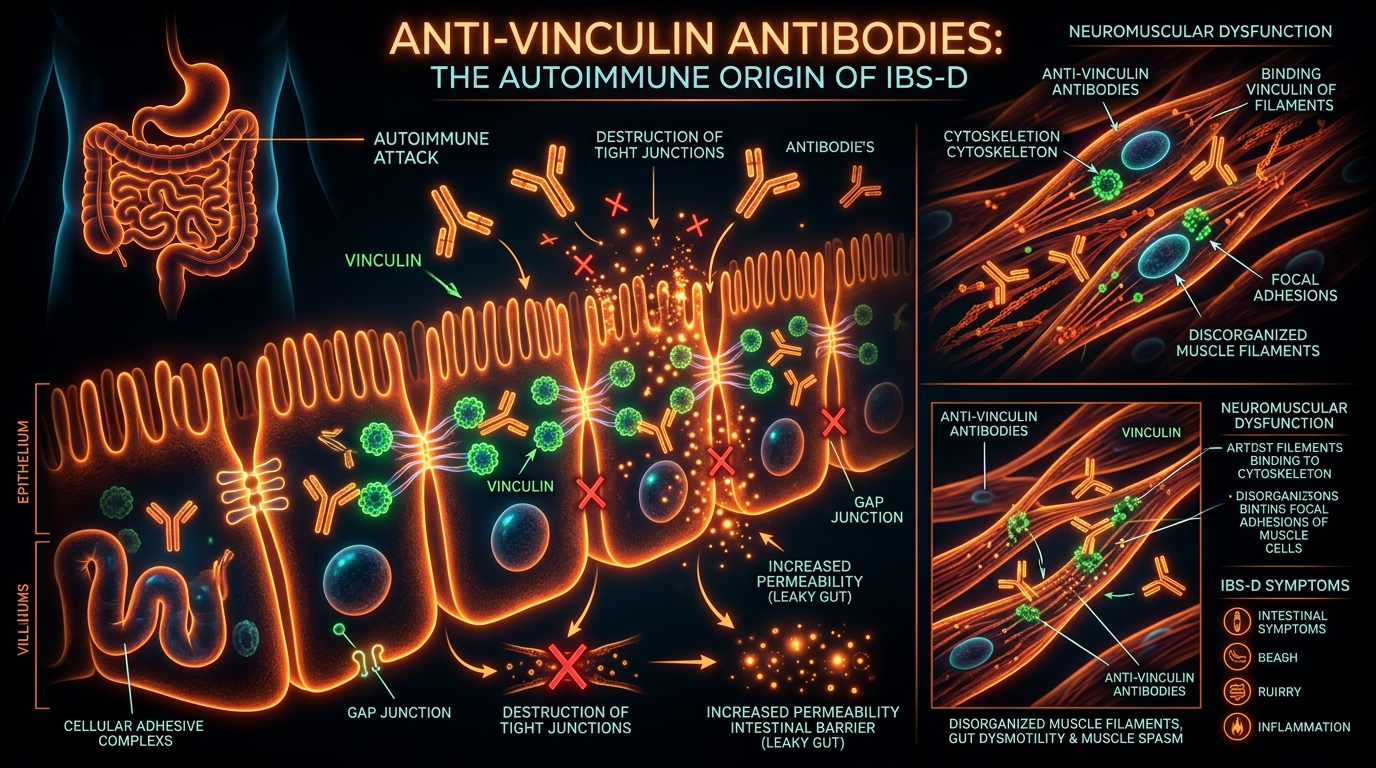
The human body is remarkably efficient at identifying foreign invaders, but it is not infallible. The immune system identifies CdtB as a high-priority target. However, the amino acid sequence of CdtB contains motifs that look alarmingly similar to vinculin. Vinculin is a cytoskeletal protein essential for cell-to-cell adhesion and the structural integrity of the Interstitial Cells of Cajal (ICCs) and the enteric nerves.
When the immune system produces anti-CdtB antibodies, these antibodies often "cross-react" with vinculin. This is the definition of molecular mimicry: the body’s "friendly fire" against its own proteins. The presence of anti-vinculin antibodies in the blood is now a validated biomarker for PI-SIBO, proving that the condition is an organic, autoimmune disease rather than a functional mystery.
---
##
Mechanisms at the Cellular Level
Delving deeper into the microscopic architecture of the gut reveals the true scale of the devastation caused by anti-vinculin antibodies. The damage is primarily localised within the myenteric plexus, a network of nerves located between the layers of the muscularis propria in the gastrointestinal tract.
The Role of Vinculin in Nerve Health
Vinculin is not just a structural filler; it is a linchpin of the focal adhesion complex. This complex connects the internal cytoskeleton of a cell to the extracellular matrix. In the context of the gut, vinculin is vital for the health and connectivity of the Interstitial Cells of Cajal (ICCs). These cells are the "pacemakers" of the gut; they generate the electrical slow waves that coordinate smooth muscle contractions.
When anti-vinculin antibodies bind to these proteins, they disrupt the structural integrity of the ICCs. Without functional vinculin, these pacemaker cells cannot maintain their connections or communicate effectively with the smooth muscle. Over time, the density of ICCs in the small intestine decreases—a phenomenon known as ICC loss. This loss is directly proportional to the severity of the motility defect.
The Failure of the Myenteric Plexus
The myenteric plexus (Auerbach's plexus) is responsible for the motor control of the gut. The autoimmune attack leads to a state of enteric neuropathy. The nerves become "blunted" or "frayed," unable to transmit the signals required to initiate the MMC.
Crucially, this is not a temporary inflammatory state. Because the body continues to produce anti-vinculin antibodies long after the *Campylobacter* or *Salmonella* has been cleared, the damage to the nerves can become chronic. This creates a permanent or semi-permanent state of stasis in the small intestine. When the "housekeeper" is absent, the small intestine becomes a stagnant pool, allowing bacteria to migrate from the colon (where they belong) into the small intestine (where they do not).
Bacterial Fermentation and Gas Production
Once the bacteria have colonised the small intestine, they begin to ferment the carbohydrates and fibres that the host consumes. This fermentation produces gases—primarily Hydrogen (H2), Methane (CH4), and Hydrogen Sulphide (H2S).
- —Hydrogen is produced by the fermentation of carbohydrates and is often associated with diarrhoea-predominant SIBO.
- —Methane is produced by archaea (specifically *Methanobrevibacter smithii*) that consume hydrogen. Methane acts as a local paralytic, further slowing transit and leading to chronic constipation.
- —Hydrogen Sulphide is associated with visceral hypersensitivity and "rotten egg" smelling gas.
The pressure from these gases causes the characteristic bloating and distension of SIBO, while the metabolic byproducts of the bacteria can damage the intestinal lining (the brush border), leading to malabsorption and systemic inflammation.
---
##
Environmental Threats and Biological Disruptors
While the primary cause of PI-SIBO is an acute infection, the modern environment plays a significant role in priming the immune system for this catastrophic overreaction. We are living in an era of unprecedented biological disruption, where our gut microbiomes and immune systems are under constant assault.
The Impact of Glyphosate and Agricultural Chemicals
Modern industrial farming relies heavily on herbicides like glyphosate. Emerging research suggests that glyphosate may act as a potent disruptor of the gut barrier and the microbiome. By altering the tight junctions of the intestinal wall—a condition known as leaky gut—glyphosate allows toxins like CdtB to enter the bloodstream more readily, increasing the likelihood of a systemic autoimmune response. Furthermore, glyphosate may inhibit the growth of "beneficial" bacteria that would otherwise keep pathogenic strains in check.
The Hygiene Hypothesis and Immune Dysregulation
The "Hygiene Hypothesis" suggests that our modern, hyper-sanitised environments prevent our immune systems from being properly "educated" during childhood. In the absence of diverse microbial exposures, the immune system becomes hyper-reactive and prone to errors like molecular mimicry. When a person raised in such an environment is suddenly exposed to a high dose of *Campylobacter* from undercooked chicken, their immune system may overreact, producing an excessive amount of CdtB antibodies that are more likely to cross-react with vinculin.
Antibiotic Overuse
The indiscriminate use of broad-spectrum antibiotics—both in human medicine and livestock—has decimated the diversity of the human microbiome. A "thin" microbiome lacks the resilience to withstand a pathogenic invasion. If a person’s indigenous microbial population is weak, a pathogen can more easily establish a foothold and produce the CdtB toxin in quantities that overwhelm the host's regulatory mechanisms.
Data from the UK’s Food Standards Agency (FSA) indicates that roughly 50-70% of retail chicken in the UK tests positive for *Campylobacter*, the leading cause of the molecular mimicry that triggers PI-SIBO.
---
##
The Cascade: From Exposure to Disease
The progression from a simple case of food poisoning to a chronic, life-altering autoimmune condition follows a predictable, yet devastating, cascade.
- —Ingestion: The host consumes food or water contaminated with CdtB-producing pathogens (*Campylobacter*, *Salmonella*, etc.).
- —Acute Infection: The pathogen colonises the gut, releasing Cytolethal Distending Toxin B. The host experiences standard "stomach flu" symptoms: cramps, diarrhoea, and vomiting.
- —Immune Mobilisation: The adaptive immune system identifies CdtB and creates B-cells to produce anti-CdtB antibodies.
- —The Molecular Error: Due to the structural similarity between CdtB and the human protein vinculin, the newly formed antibodies begin to attack the vinculin proteins within the Interstitial Cells of Cajal (ICCs).
- —Neurological Erosion: The myenteric plexus and ICCs suffer structural damage. The electrical pacing of the small intestine is disrupted.
- —The Failure of the MMC: The Migrating Motor Complex loses its Phase III "clearing wave." Stasis occurs in the small intestine.
- —Bacterial Translocation: Bacteria from the colon migrate upward into the small intestine. They find a rich environment of undigested carbohydrates and begin to proliferate.
- —Chronic SIBO: The patient begins to experience chronic bloating, altered bowel habits, and nutrient deficiencies.
- —The Autoimmune Loop: Even after the bacteria are cleared with antibiotics, the anti-vinculin antibodies may remain high, meaning the MMC remains broken. This explains why SIBO has such a high recurrence rate—often cited as 60-80% within a year of treatment.
---
##
What the Mainstream Narrative Omits
The current medical approach to "IBS" in the UK and globally is profoundly inadequate, often bordering on negligence. By failing to acknowledge the molecular mimicry of CdtB, the mainstream narrative leaves millions of patients in a cycle of suffering and "gaslighting."
The "Stress" Fallacy
For decades, patients have been told that their gut issues are a result of stress or anxiety. While the gut and brain are undeniably linked, this narrative reverses the order of operations. The inflammation and dysbiosis caused by PI-SIBO create systemic "biological stress" that can lead to anxiety and depression via the vagus nerve and the production of inflammatory cytokines. Stress does not cause anti-vinculin antibodies; molecular mimicry does.
The Diagnostic Gap
The standard of care for IBS usually involves a "diagnosis of exclusion." GPs may run basic blood tests for Coeliac disease and Inflammatory Bowel Disease (IBD), and if these are negative, the patient is given an IBS label and told to "eat more fibre" or "try a low-FODMAP diet."
What is omitted is the IBS-Smart or second-generation blood testing. These tests specifically measure the levels of anti-CdtB and anti-vinculin antibodies. High levels of these antibodies provide a definitive, organic diagnosis of PI-SIBO. In the UK, these tests are rarely available on the NHS, leaving patients to seek expensive private testing or remain undiagnosed.
The Failure of "More Fibre"
The standard advice to increase fibre intake is often the worst possible recommendation for a SIBO patient. Fibre is the primary fuel for the bacteria overgrowing in the small intestine. In a gut with a broken MMC, adding more fibre is like adding more cars to a motorway that is already blocked by a multi-car pile-up. It simply increases the substrate for fermentation, leading to more gas, more pain, and more damage.
---
##
The UK Context
The United Kingdom presents a unique and challenging environment for the management of Post-Infectious SIBO. Despite having a robust healthcare system, the disconnect between cutting-edge research and clinical practice is stark.
The Burden on the NHS
IBS is estimated to cost the UK economy over £1.3 billion annually in lost productivity and healthcare resources. Yet, the NHS remains slow to adopt the "post-infectious" model. Patients are often stuck in a loop of repeat appointments, unnecessary colonoscopies, and ineffective medications like buscopan or mebeverine, which do nothing to address the underlying autoimmune neuropathy.
Food Standards and Poultry
The UK’s reliance on intensive poultry farming is a significant risk factor. *Campylobacter* is the most common cause of bacterial food poisoning in the UK. Despite efforts by the Food Standards Agency (FSA), contamination rates remain high. A single undercooked Sunday roast or a cross-contaminated cutting board can be the trigger for a decade of chronic illness.
The "Wait and See" Culture
The British medical culture often leans toward conservative management. While this is beneficial in avoiding over-medicalisation, it is detrimental in the case of PI-SIBO. Early intervention—identifying the autoimmune trigger and using prokinetics to support the MMC—can prevent the long-term loss of ICCs. By the time a patient is referred to a specialist after years of "waiting and seeing," the neurological damage may be irreversible.
---
##
Protective Measures and Recovery Protocols
Recovering from Post-Infectious SIBO requires a multi-faceted approach that goes beyond simply "killing" the bacteria. We must address the underlying autoimmune cause and the broken motility.
1. Identifying the Root Cause
The first step is testing. If you have a history of food poisoning followed by a change in bowel habits, you must seek testing for anti-CdtB and anti-vinculin antibodies. Knowing your "titer" (the level of antibodies) is essential for determining the prognosis. High anti-vinculin levels suggest a more aggressive autoimmune process that requires longer-term management.
2. Clearing the Overgrowth
Once SIBO is confirmed via a Breathe Test (measuring hydrogen and methane), the bacteria must be cleared.
- —Pharmaceuticals: Rifaximin is the gold standard as it is non-systemic and stays within the small intestine. For methane-producers, Neomycin or Metronidazole is often added.
- —Herbal Antimicrobials: High-dose Oregano oil, Berberine, and Neem have shown efficacy comparable to Rifaximin in clinical trials.
3. Restoring the MMC (Prokinetics)
This is the most critical and often overlooked step. If the MMC is not restored, SIBO *will* return.
- —Pharmaceutical Prokinetics: Low-dose Erythromycin (acting on motilin receptors) or Prucalopride (a 5-HT4 agonist) can stimulate the MMC.
- —Natural Prokinetics: Ginger and Artichoke extracts have been shown to support gastric emptying and small intestinal motility.
- —Meal Spacing: To allow the MMC to function, one must avoid snacking. A minimum of 4–5 hours between meals and a 12-hour overnight fast is essential to allow the Phase III clearing waves to occur.
4. Protecting the Interstitial Cells of Cajal
While we cannot easily "replace" lost nerves, we can support the remaining ICCs. This involves reducing systemic inflammation through an anti-inflammatory diet (rich in polyphenols) and ensuring adequate levels of Vitamin D and B12, which are often depleted in SIBO patients.
5. Diet as a Management Tool
The Bi-Phasic Diet or Low FODMAP Diet should be used as a short-term tool to manage symptoms, not a long-term cure. The goal is to eventually transition back to a diverse, whole-food diet that feeds a healthy colonic microbiome without overfeeding the small intestinal overgrowth.
---
##
Summary: Key Takeaways
- —PI-SIBO is Autoimmune: It is not a "functional" disorder; it is a measurable autoimmune reaction triggered by Cytolethal Distending Toxin B (CdtB).
- —Molecular Mimicry: The body’s antibodies against food poisoning toxins mistakenly attack vinculin, a protein vital for gut nerve health.
- —The "Housekeeper" Fails: This attack damages the Migrating Motor Complex (MMC), the mechanical wave that keeps the small intestine clean.
- —Bacterial Stasis: Without the MMC, bacteria migrate into the small intestine, leading to fermentation, gas production, and inflammation.
- —Mainstream Failure: Standard IBS treatments (fibre, antispasmodics) fail because they do not address the underlying motility defect or the autoimmune trigger.
- —Recovery Requires Prokinetics: Simply killing bacteria is not enough. To prevent relapse, the MMC must be pharmacologically or naturally supported.
- —Testing is Vital: Second-generation blood tests for anti-CdtB and anti-vinculin are the only way to confirm this specific autoimmune pathway.
The era of dismissive "IBS" diagnoses is over. By understanding the molecular mimicry of CdtB, we can finally offer patients a clear explanation for their suffering and a scientifically grounded path to recovery. The gut is not a mystery; it is a machine, and we finally have the blueprint to fix it.
This article is provided for informational and educational purposes only. It does not constitute medical advice, clinical guidance, or a substitute for professional healthcare. Information reflects cited research at time of publication. Always consult a qualified healthcare professional before acting on any health information.
RESEARCH FOUNDATIONS
Biological Credibility Archive
Citations provided for educational reference. Verify via PubMed or institutional databases.
Medical Disclaimer
The information in this article is for educational purposes only and does not constitute medical advice, diagnosis, or treatment. Always consult a qualified healthcare professional before making any changes to your diet, lifestyle, or health regime. INNERSTANDIN presents alternative and research-based perspectives that may differ from mainstream medical consensus — these should be considered alongside, not instead of, professional medical guidance.
Read Full DisclaimerReady to learn more?
Continue your journey through our classified biological research.
DISCUSSION ROOM
Members of THE COLLECTIVE discussing "Post-Infectious SIBO: The Molecular Mimicry of Cytolethal Distending Toxin B"
SILENT CHANNEL
Be the first to discuss this article. Your insight could help others understand these biological concepts deeper.
THE ARSENAL
Based on SIBO & Small Intestine Health — products curated by our research team for educational relevance and biological support.

Panaceum – Prebiotic Oligosaccharide Complex

Magnesium Blend – The Most Important Mineral

Clean Slate – Detoxes thousands of chemicals,heavy metals, pesticides, allergens, mold spores and fungus
INNERSTANDING may earn a commission on purchases made through these links. All products are selected based on rigorous educational relevance to our biological research.
RABBIT HOLE
Follow the biological thread deeper