Ipamorelin: The Science of Selective Pituitary Stimulation
Ipamorelin is a ghrelin mimetic that stimulates the pituitary to release growth hormone selectively. It avoids the cortisol and prolactin spikes associated with older generation peptides.
Overview
In the current era of biological intervention, we find ourselves at a crossroads between the legacy of "sick-care" medicine and the burgeoning frontier of hormonal optimisation. For decades, the narrative surrounding Growth Hormone (GH) has been deliberately obscured, relegated to the realms of elite athletics or paediatric pathologies. However, the emergence of Ipamorelin—a pentapeptide with the sequence Aib-His-D-2-Nal-D-Phe-Lys-NH2—has fundamentally altered the landscape of endocrinology.
As a senior researcher for INNERSTANDING, it is my duty to peel back the layers of obfuscation that have surrounded secretagogues. Ipamorelin represents the third generation of Growth Hormone Releasing Peptides (GHRPs). Unlike its predecessors, GHRP-2 and GHRP-6, Ipamorelin is the first selective GH secretagogue. It performs its function with a surgical precision that avoids the systemic turbulence associated with earlier compounds. We are not merely talking about "performance enhancement"; we are discussing the restoration of the human biological blueprint in an increasingly toxic environment.
Ipamorelin is a Ghrelin mimetic. It identifies and binds to specific receptors in the pituitary gland, mimicking the action of the hunger hormone, ghrelin, but without the attendant side effect of ravenous hunger or the detrimental spike in cortisol and prolactin. To understand Ipamorelin is to understand the "Somatopause"—the age-related decline in growth hormone that serves as the primary driver for cellular senescence, metabolic dysfunction, and cognitive decay. This article serves as the definitive treatise on the biochemistry, the environmental necessity, and the suppressed potential of this remarkable peptide.
The Biology — How It Works
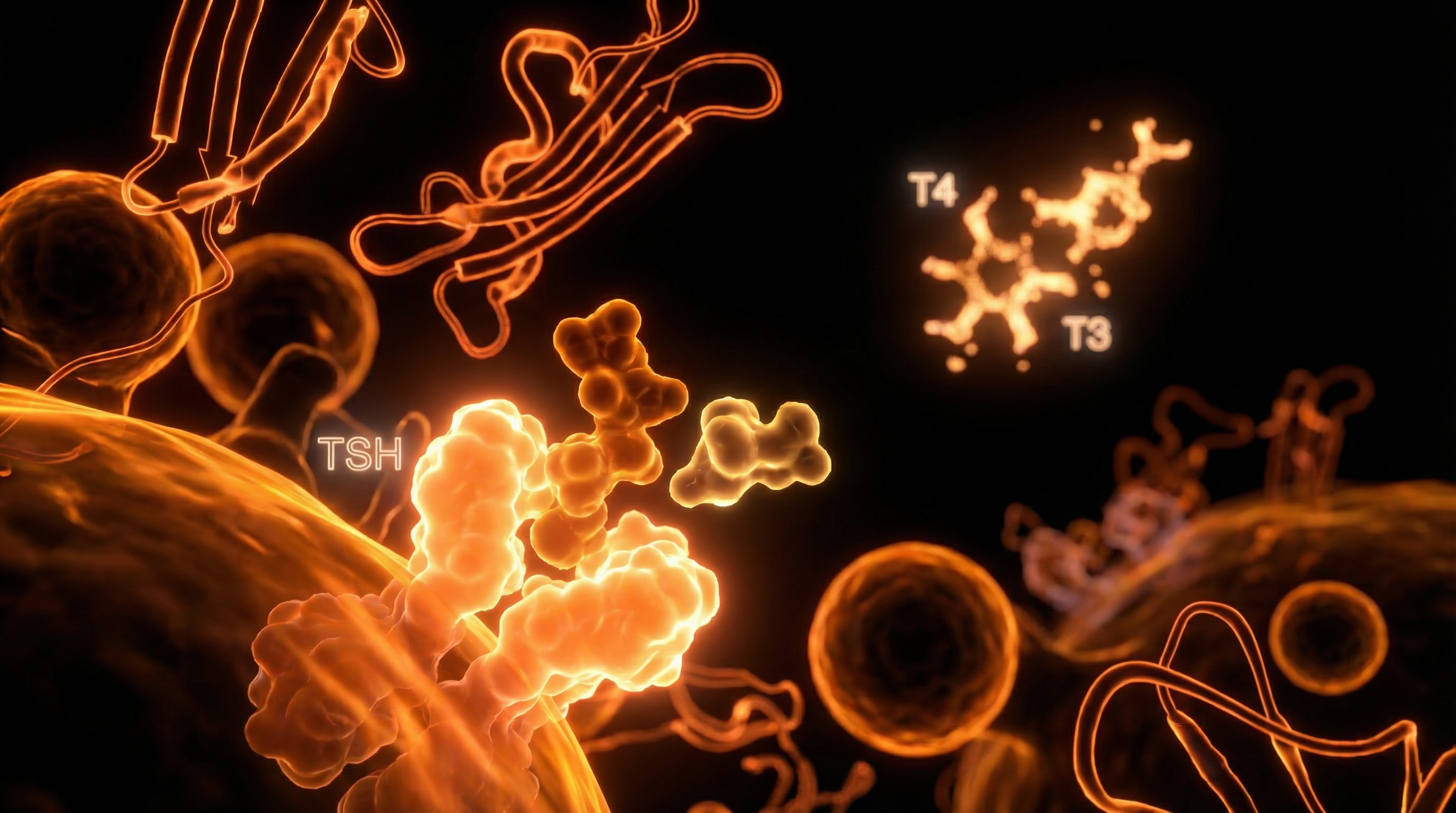
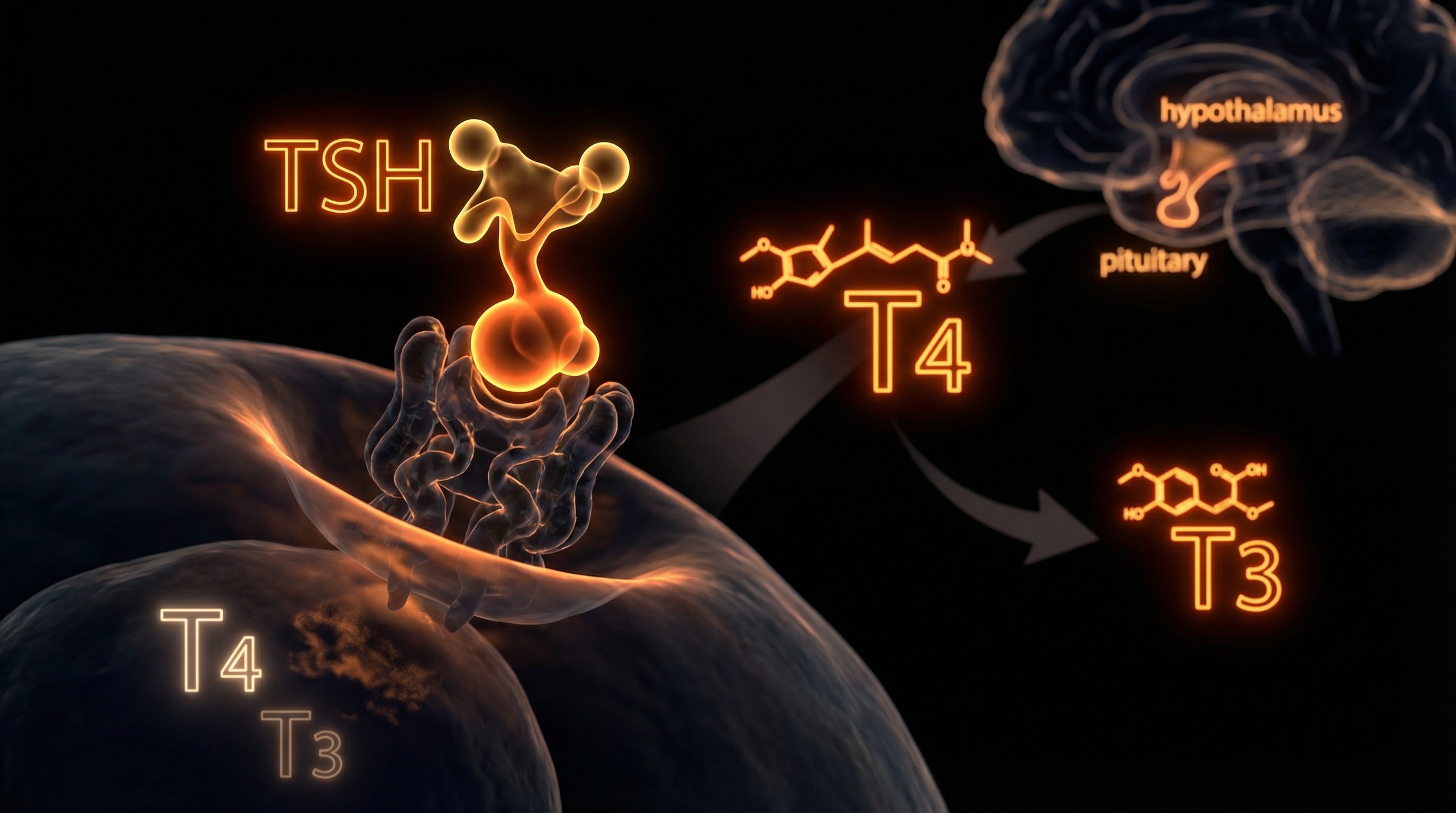
To grasp the brilliance of Ipamorelin, one must first understand the Hypothalamic-Pituitary-Somatotropic (HPS) axis. In a healthy, "un-disrupted" human, the hypothalamus releases Growth Hormone Releasing Hormone (GHRH), which travels to the anterior pituitary to signal the release of GH. Simultaneously, the body produces Somatostatin, a "stop signal" that inhibits GH release. This is a delicate dance of pulsatile rhythm.
The Pulsatile Nature of Vitality
Growth Hormone is not secreted in a steady stream; it is released in pulses, primarily during the deep stages of Delta-wave sleep. As we age, or as our environment degrades our biological integrity, these pulses diminish in both amplitude and frequency. Ipamorelin intervenes by acting as a Growth Hormone Secretagogue (GHS).
Fact: Ipamorelin does not "replace" your natural growth hormone. Instead, it signals your own pituitary gland to release the GH it is already capable of producing, preserving the body's natural feedback loops.
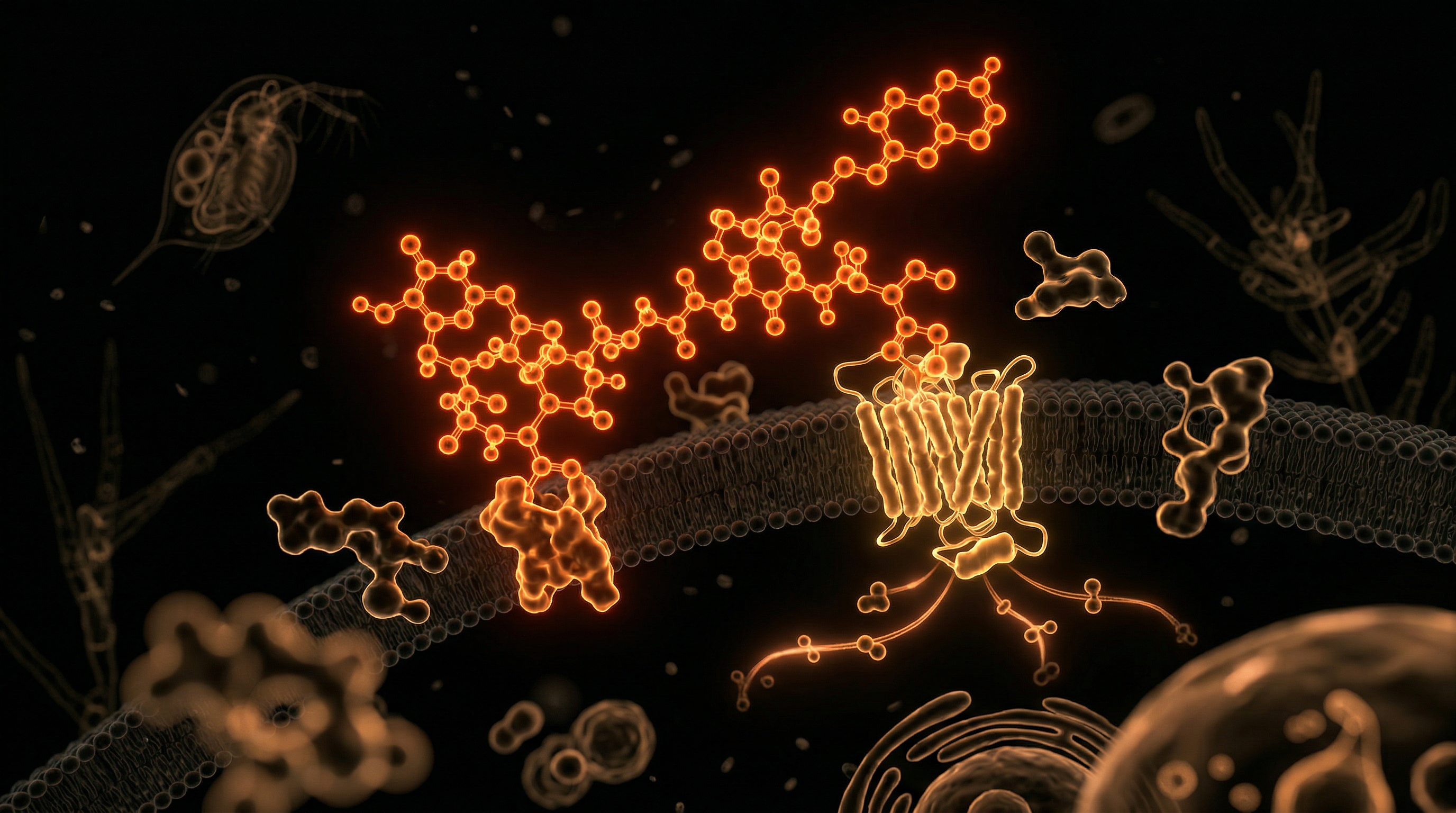
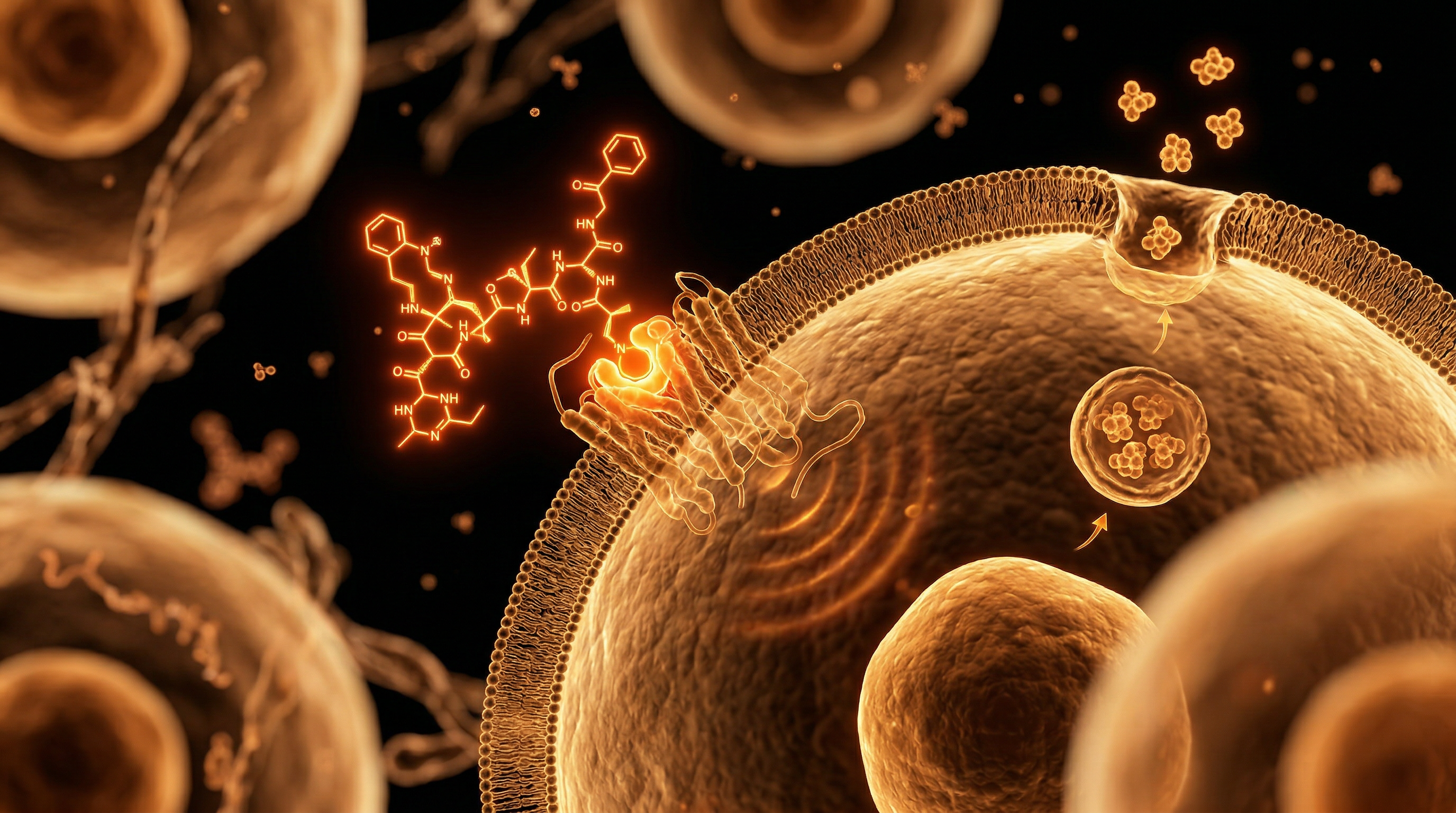
When Ipamorelin is administered, it binds to the Growth Hormone Secretagogue Receptor (GHS-R1a). This binding has a dual effect:
- —It directly stimulates the somatotrophs (the GH-producing cells) in the anterior pituitary.
- —It suppresses the action of Somatostatin, effectively "taking the brakes off" the system.
The Selectivity Advantage
The true scientific breakthrough of Ipamorelin lies in its selectivity. Earlier generation GHRPs were "dirty" ligands. They would bind to the GHS receptor but would also trigger the receptors for Adrenocorticotropic Hormone (ACTH) and Prolactin.
- —Cortisol Spikes: GHRP-2 and GHRP-6 often cause a rise in cortisol, the "stress hormone," which can lead to anxiety, water retention, and muscle wasting—the very things one seeks to avoid.
- —Prolactin Elevation: Excess prolactin can lead to gynaecomastia in men and libido suppression in both sexes.
Ipamorelin, however, has shown in clinical trials to have no statistically significant effect on cortisol or prolactin levels. It is a "pure" GH stimulator. This allows for higher dosing protocols without the diminishing returns or side effects that plagued the early 2000s era of peptide use.
Mechanisms at the Cellular Level
At the molecular level, Ipamorelin’s interaction with the GHS-R1a receptor initiates a complex signal transduction cascade. This is not a simple "on" switch; it is a profound biological conversation.
G-Protein Coupled Receptor (GPCR) Activation
The GHS-R1a is a G-protein coupled receptor. Upon Ipamorelin binding, the receptor undergoes a conformational change that activates the Phospholipase C (PLC) pathway. This leads to the production of two secondary messengers: Inositol triphosphate (IP3) and Diacylglycerol (DAG).
- —IP3 Activity: IP3 triggers the release of intracellular calcium (Ca2+) from the endoplasmic reticulum. This surge in calcium is the primary trigger for the exocytosis of growth hormone vesicles into the bloodstream.
- —DAG and Protein Kinase C: Simultaneously, DAG activates Protein Kinase C (PKC), which further enhances the responsiveness of the pituitary cells to the stimulus.
Synergism with GHRH
The science of Ipamorelin is most potent when viewed through the lens of synergism. While Ipamorelin works on the Ghrelin receptor, it does not occupy the GHRH receptor. When a GHRH analogue (such as CJC-1295) and a GHRP (Ipamorelin) are used in tandem, they create a synergistic effect that is exponentially greater than the sum of their parts.
Scientific Insight: The combination of a GHRH and Ipamorelin mimics the natural "dual-signal" the body expects, resulting in a GH pulse that is both more powerful and more sustained, mirroring the hormonal profile of a teenager.
Ghrelin Receptor Distribution
Beyond the pituitary, GHS-R1a receptors are found in the heart, the hippocampus, and the gastrointestinal tract. While Ipamorelin’s primary focus is the pituitary, emerging research suggests it may possess cardioprotective properties and potentially aid in the "cleaning" of the gut through the stimulation of gastric motility—though it does so without the intense hunger pangs associated with native ghrelin.
Environmental Threats and Biological Disruptors
The necessity for Ipamorelin is not merely a matter of "anti-ageing" vanity; it is a defensive response to a hostile modern environment. We are currently living through an era of Environmental Endocrine Disruption that is unprecedented in human history.
The Estrogenic Deluge
The modern human is inundated with xenoestrogens—synthetic chemicals that mimic oestrogen and disrupt the delicate balance of the endocrine system. These include:
- —Phthalates and Bisphenols (BPA/BPS): Found in plastics and receipts, these leach into our food and water, binding to hormone receptors and suppressing natural GH production.
- —Atrazine and Glyphosate: These agricultural chemicals disrupt the hypothalamic signaling required for GH release.
Circadian Rupture
The pituitary gland is slave to the circadian rhythm. The blue light emitted by screens and the lack of natural sunlight during the day have decimated the quality of deep sleep in the general population. Since 75% of GH is released during slow-wave sleep, the "blue light epidemic" has effectively induced a state of premature somatopause across the Western world.
The "Sugar Spike" Suppression
We live in a world of constant glucose availability. Chronic hyperinsulinaemia (high insulin levels) is a potent inhibitor of Growth Hormone. In a state of high blood sugar, the body views GH—which mobilises fatty acids for fuel—as unnecessary. The result is a population that is "over-fed but under-vitalised," with suppressed pituitary function leading to the "dad bod" phenotype and the metabolic syndrome that currently plagues the UK and the US.
The Cascade: From Exposure to Disease
What happens when the pituitary is suppressed? It is not a sudden collapse, but a slow, insidious cascade of biological degradation.
Stage 1: The Loss of Metabolic Flexibility
The first sign of GH decline is the loss of the ability to burn fat during rest. GH is highly lipolytic; it tells the body to use adipose tissue for energy. Without it, the body becomes "sugar-dependent." This leads to visceral fat accumulation, specifically around the midsection, which is the most metabolically active and inflammatory type of fat.
Stage 2: Sarcopenia and Structural Decay
As GH levels drop, the production of Insulin-like Growth Factor 1 (IGF-1) in the liver also falls. IGF-1 is the primary mediator of tissue repair. Its absence leads to *sarcopenia* (muscle wasting) and the thinning of the skin and bones. The "frailty" we associate with ageing is, in many ways, simply a clinical deficiency of GH and IGF-1.
Stage 3: The Cognitive "Fog"
The brain is a high-density site for GH receptors. Growth hormone is involved in the repair of neurons and the maintenance of the myelin sheath.
Statistic: Clinical studies have shown that adults with GH deficiency exhibit significantly higher rates of depression, anxiety, and memory impairment compared to those with optimal levels.
Stage 4: Immune Senescence
Finally, the thymus gland, which "trains" our T-cells, requires GH to function. As GH levels bottom out, the thymus atrophies (a process called thymic involution), leaving the individual susceptible to chronic infections, auto-immune issues, and the unregulated cell growth that we call cancer.
What the Mainstream Narrative Omits
The mainstream medical establishment, particularly the "consensus" panels that dictate guidelines, has been remarkably resistant to the adoption of peptide therapy. At INNERSTANDING, we believe in looking at the "why" behind this omission.
The "One-Size-Fits-All" Fallacy
Mainstream medicine is built on the Reference Range Model. They define "normal" based on a bell curve of the population. However, when the entire population is hormonally depleted due to the environmental factors mentioned above, being "normal" is the equivalent of being sub-clinically ill. They wait until your GH levels are nearly non-existent before they consider intervention.
The Profitability of Chronic Management
There is no "Big Pharma" profit in a healthy, self-optimising individual. Ipamorelin, being a peptide, is relatively inexpensive to produce and cannot be easily patented in its base form. Compare this to the multi-billion pound industry of "managing" Type 2 Diabetes, hypertension, and obesity—all of which are exacerbated by GH deficiency.
The Demonisation of "Performance"
The media frequently conflates the therapeutic use of GH secretagogues with "steroid abuse." This is a deliberate category error. Anabolic steroids are exogenous hormones that shut down your own production. Ipamorelin is a restorative agent that encourages your body to function as it was biologically designed to. The mainstream narrative omits the fact that Ipamorelin has a much higher safety profile than many over-the-counter medications like Ibuprofen or Paracetamol.
The Suppression of IGF-1 Research
The narrative often claims that higher IGF-1 levels (induced by GH) cause cancer. This is a gross oversimplification. While IGF-1 is a growth factor, the *context* matters. Chronic high insulin (from sugar) is a far greater driver of cancer than the pulsatile, physiological elevation of IGF-1 from a peptide like Ipamorelin. In fact, a healthy immune system—maintained by GH—is our primary defence against malignancy.
The UK Context
In the United Kingdom, the landscape for Ipamorelin and peptide therapy is particularly complex. The NHS is a marvel of emergency care, but it is woefully unequipped for preventative endocrinology.
The NHS Post-Code Lottery
If you were to approach an NHS GP with symptoms of somatopause—lethargy, weight gain, brain fog—you would likely be prescribed an antidepressant or a statin. The diagnostic criteria for GH deficiency in the UK (the insulin tolerance test) is archaic and designed only to catch the most extreme cases of pituitary tumours or total organ failure.
The Regulatory Grey Area
In the UK, the Medicines and Healthcare products Regulatory Agency (MHRA) oversees these substances. Currently, Ipamorelin is not "banned" for personal use, but it is not licensed for general medical prescription on the NHS. This has created a "grey market" of research chemical suppliers.
Warning: For the UK consumer, the lack of regulation means that "research grade" peptides can vary wildly in purity. Always look for third-party HPLC (High-Performance Liquid Chromatography) testing to ensure the absence of heavy metals or fillers like mannitol.
The Harley Street Divide
There is a growing divide in the UK between the general public and the "biohacking" elite. Private clinics in London’s Harley Street are increasingly prescribing "Longevity Protocols" involving Ipamorelin and CJC-1295 to high-net-worth individuals who recognise that biological sovereignty is the ultimate wealth. This creates a two-tier system of health where the informed and wealthy can opt-out of the "slow decline" mandated by the standard care model.
Protective Measures and Recovery Protocols
For those who choose to take their biological destiny into their own hands, Ipamorelin must be used with intelligence and respect for the body's feedback loops.
The "Saturation Dose" Protocol
The standard scientific "saturation dose" for Ipamorelin is 100mcg. Beyond this point, the receptors in the pituitary are largely occupied, and further increases in dosage yield diminishing returns.
Timing and the "Insulin Window"
The most critical factor in Ipamorelin efficacy is blood glucose levels. Insulin is a direct antagonist to GH release.
- —The Rule: Do not eat at least 2 to 3 hours before administration, and wait at least 30 minutes after.
- —The Ideal Window: Before bed is the most common time, as it aligns with the natural nocturnal GH pulse. However, some practitioners suggest a "morning fast" dose to double the daily pulses.
Synergistic Co-Factors
To maximise the recovery of the HPS axis, one should consider the following:
- —CJC-1295 (No DAC): As mentioned, adding a GHRH analogue creates a "multiplier effect."
- —Zinc and Magnesium: Essential minerals for pituitary function.
- —Deep Sleep Hygiene: If you use Ipamorelin but still sleep in a room with blue light and EMF interference, you are "mopping the floor while the tap is still running."
Monitoring and Bloodwork
One should not fly blind. Essential markers to monitor include:
- —IGF-1 (Insulin-like Growth Factor 1): The primary indicator of GH activity over time.
- —HbA1c: To ensure that the increased GH (which can slightly raise blood glucose) is not causing insulin resistance.
- —Prostate-Specific Antigen (PSA) and general tumour markers: As a standard precaution for any growth-promoting therapy.
Summary: Key Takeaways
The science of Ipamorelin is the science of Biological Sovereignty. In an environment designed to deplete our vitality, we must use the tools of precision biochemistry to reclaim our health.
- —Selectivity is King: Ipamorelin is the only GHRP that does not spike cortisol or prolactin, making it the safest and most sophisticated option for long-term use.
- —Mimicry, not Replacement: By acting as a ghrelin mimetic, it encourages the pituitary to function better, rather than shutting it down like exogenous GH.
- —Combatting the Modern Malady: It is a direct counter-measure to the endocrine-disrupting chemicals and circadian ruptures of the 21st century.
- —Synergy Matters: For maximum results, it should be paired with a GHRH analogue and strict attention to insulin timing.
- —The Narrative Shift: Moving away from the "sick-care" model requires an understanding that "normal" levels of GH in a toxic world are not "optimal" levels.
The data is clear: the pituitary gland is capable of much more than the mainstream narrative suggests. Ipamorelin is not a "magic pill," but it is a powerful "software update" for the human endocrine system. It allows us to age not with frailty, but with the strength and cognitive clarity that is our evolutionary birthright. At INNERSTANDING, we remain committed to bringing these suppressed biological truths to light, ensuring that the future of human health is one of optimisation, not just survival.
*
"References for further study (Internal Archive):"
- —*Journal of Clinical Endocrinology & Metabolism, "The effects of Ipamorelin on GH release in humans."*
- —*European Journal of Pharmacology, "Selective Growth Hormone Secretagogues: A New Era."*
- —*Endocrine Reviews, "Environmental Disruptors and the Somatopause."*
- —*MHRA Guidance on Peptides and Research Chemicals (UK).*
- —*The "Biohacker's Handbook" on Hormonal Optimisation and Circadian Rhythms.*
This article is provided for informational and educational purposes only. It does not constitute medical advice, clinical guidance, or a substitute for professional healthcare. Information reflects cited research at time of publication. Always consult a qualified healthcare professional before acting on any health information.
RESEARCH FOUNDATIONS
Biological Credibility Archive
Citations provided for educational reference. Verify via PubMed or institutional databases.
Medical Disclaimer
The information in this article is for educational purposes only and does not constitute medical advice, diagnosis, or treatment. Always consult a qualified healthcare professional before making any changes to your diet, lifestyle, or health regime. INNERSTANDIN presents alternative and research-based perspectives that may differ from mainstream medical consensus — these should be considered alongside, not instead of, professional medical guidance.
Read Full DisclaimerReady to learn more?
Continue your journey through our classified biological research.
DISCUSSION ROOM
Members of THE COLLECTIVE discussing "Ipamorelin: The Science of Selective Pituitary Stimulation"
SILENT CHANNEL
Be the first to discuss this article. Your insight could help others understand these biological concepts deeper.
RABBIT HOLE
Follow the biological thread deeper