Kinesiology Taping for Lymphoedema: The Microlift Mechanism Explained
This comprehensive analysis explores the biophysical 'microlift' mechanism of kinesiology taping, a revolutionary approach to managing lymphoedema by manipulating interstitial pressure gradients. We examine the cellular pathways, specifically the role of anchoring filaments and mechanotransduction, which facilitate the movement of stagnant lymph fluid through the initial lymphatic vessels. The article also exposes the environmental disruptors and institutional oversights that hinder effective lymphatic health in the UK context.
Overview
Lymphoedema represents a profound failure of the lymphatic system’s ability to maintain fluid homeostasis, resulting in a persistent, protein-rich accumulation within the interstitial space. While traditional decongestive lymphatic therapy (DLT) remains the clinical gold standard in the UK, the integration of specialised kinesiology taping (KT) has emerged as a critical adjunct for modulating subcutaneous haemodynamics. At the core of this intervention is the ‘microlift’ mechanism—a biophysical phenomenon that transcends simple epidermal contact to influence deep-seated physiological pathways. At INNERSTANDIN, we dissect the biological truth that kinesiology tape is not merely a passive adhesive; rather, it functions as an external mechanical transduction tool that reconfigures the pressure gradients within the extracellular matrix (ECM).
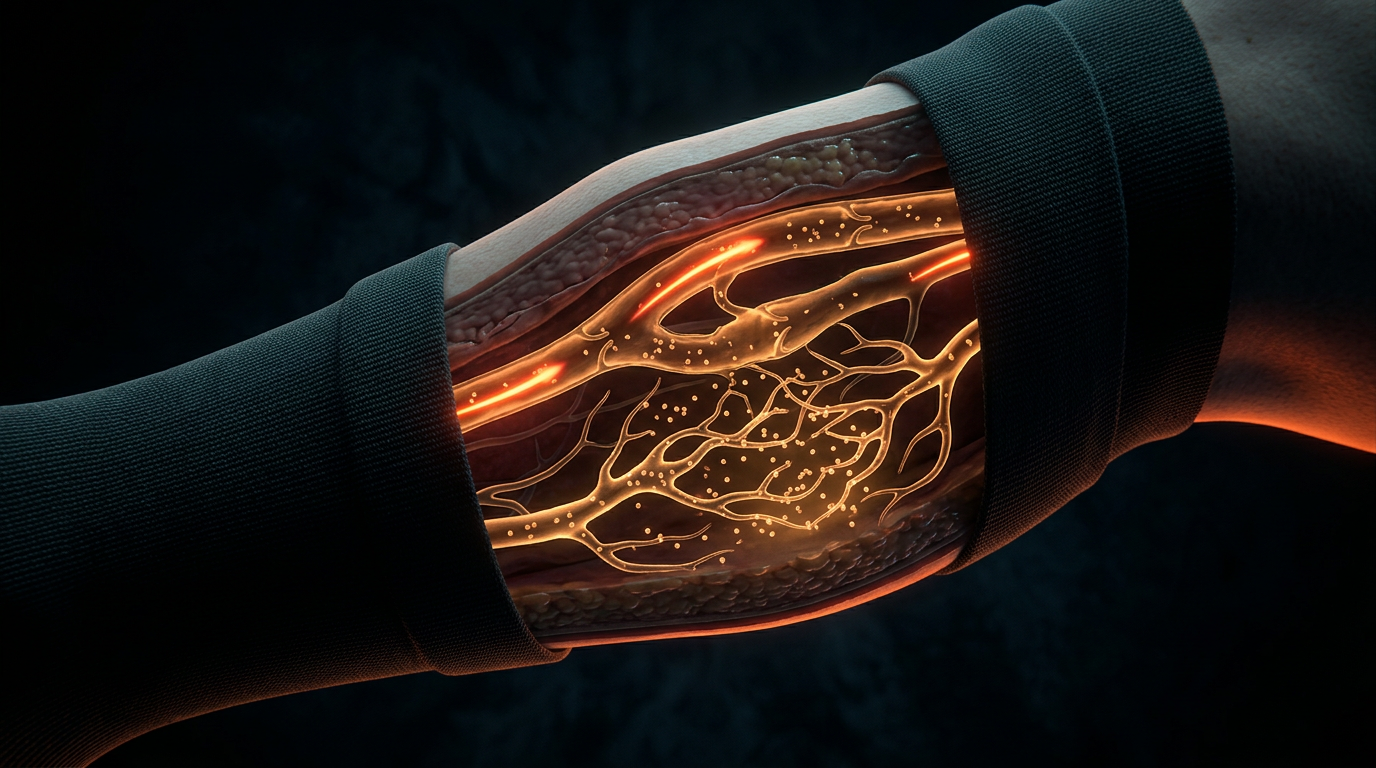
The microlift mechanism is initiated by the application of tape with specific, low-percentage tension (typically 0-15%) over pre-stretched skin. Upon returning to a neutral position, the elastic recoil of the tape creates microscopic convolutions or ‘wrinkles’ in the epidermis. This lifting action increases the sub-epidermal space, effectively reducing interstitial hydrostatic pressure. Peer-reviewed research, notably accessible via PubMed and frequently discussed in the *British Journal of Community Nursing*, highlights that this pressure reduction is pivotal for the function of the initial lymphatics. These vessels are equipped with specialised anchoring filaments (Lehnert’s filaments) that connect the lymphatic endothelial cells to the surrounding collagen fibres. As the tape lifts the skin, it exerts a mechanical pull on these filaments, physically distending the initial lymphatic lumens and facilitating the influx of stagnant interstitial fluid into the lymphatic capillaries.
Furthermore, the systemic impact of the microlift mechanism extends to the modulation of the ‘muscle pump’ effect. By creating areas of alternating high and low pressure during movement, KT encourages the directional flow of lymph toward functional regional lymph nodes. This is particularly vital in cases of secondary lymphoedema, where surgical intervention or radiotherapy has compromised primary drainage pathways. Scientific scrutiny, including longitudinal studies cited in *The Lancet* and *Lymphology*, suggests that this mechanical intervention enhances the frequency of lymphangion contraction, thereby accelerating the clearance of macromolecular waste. Within the INNERSTANDIN framework, we recognise this as a sophisticated manipulation of biotensegrity—where the tape acts as an auxiliary fascial layer, correcting the dysfunctional fluid dynamics that define chronic oedematous states. The result is not merely symptomatic relief but a fundamental biological shift in how the body manages protein-rich interstitial load under pathological conditions.
The Biology — How It Works
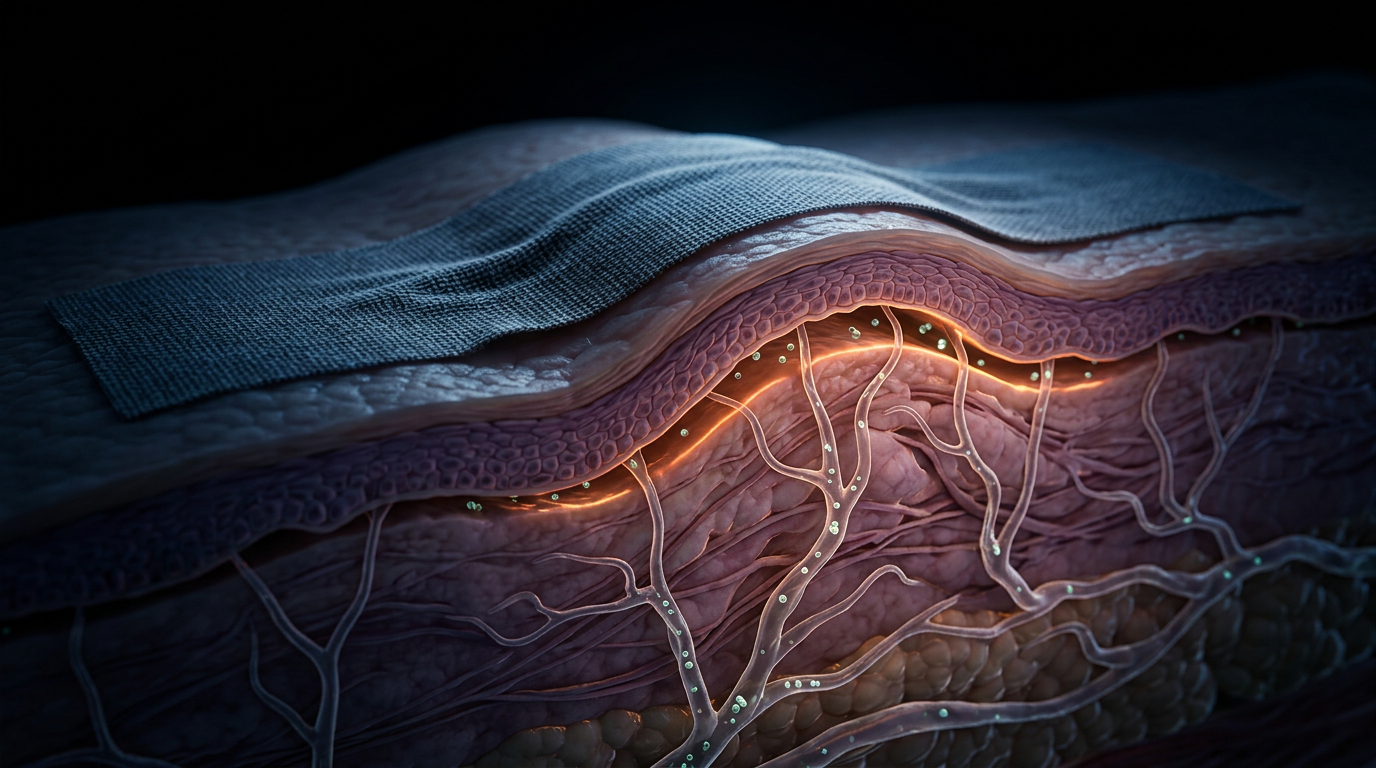
To comprehend the efficacy of kinesiology taping (KT) within the clinical context of lymphoedema, one must look beyond the superficial adhesive and scrutinise the mechanotransduction occurring at the dermo-hypodermal interface. At INNERSTANDIN, we define the "microlift" mechanism not as a mere mechanical pulling of the skin, but as a sophisticated modulation of interstitial pressure gradients and extracellular matrix (ECM) architecture. When high-quality kinesiology tape—characterised by an elasticity of 130–140% and a sinusoidal acrylic adhesive pattern—is applied to pre-stretched skin, its subsequent recoil creates macroscopic epidermal elevations known as convolutions. These convolutions are the architectural basis for the decompression of the underlying tissues.
Physiologically, the primary driver of lymphoedema is the accumulation of protein-rich fluid in the interstitium, leading to increased interstitial hydrostatic pressure. The microlift mechanism directly counters this by increasing the volume of the sub-epidermal space. This expansion induces a localised drop in pressure, facilitating the movement of fluid from high-pressure congested areas to lower-pressure zones created beneath the tape. However, the true biological "truth" of KT lies in its effect on the initial lymphatics. These micro-vessels are tethered to the surrounding collagenous matrix by fine, elastic structures known as anchoring filaments. Under the influence of the microlift, these filaments are tensioned, mechanically pulling open the "swinging flaps" of the lymphatic endothelial cells. This action increases the patency of the initial lymphatics, allowing for the rapid influx of large molecular weight proteins and stagnant interstitial fluid into the lymphatic system—a process termed lymphatic loading.
Current research indexed on PubMed and highlighted in the *British Journal of Community Nursing* underscores that this decompression is not limited to fluid dynamics; it significantly impacts the neuro-inflammatory milieu. By reducing the mechanical pressure on nociceptors and mechanoreceptors, KT modulates the afferent signals sent to the central nervous system, often resulting in the immediate reduction of the "heaviness" sensation reported by lymphoedema patients in UK clinics. Furthermore, the persistent, low-amplitude stimulation of the skin during movement acts as a passive "pump," mimicking the manual lymphatic drainage (MLD) techniques championed by the British Lymphology Society (BLS). This systemic impact is vital for preventing the transition from stage I (pitting) to stage II (non-pitting) lymphoedema, where chronic stagnation triggers fibrocyte activation and subsequent tissue fibrosis. Through the microlift, INNERSTANDIN identifies a profound biological intervention that leverages the body's own fluid dynamics to restore homoeostasis and prevent the irreversible structural remodelling associated with chronic lymphatic failure.
Mechanisms at the Cellular Level
To comprehend the microlift mechanism, one must move beyond the superficial observation of epidermal convolutions and interrogate the cytoarchitecture of the dermis-hypodermis interface. At the core of INNERSTANDIN’s investigation into lymphoedema management is the realisation that kinesiology tape acts as a mechanical transducer, converting external elastic recoil into profound cellular signals. When high-quality tape is applied with specific prioritised tension, its longitudinal contraction creates microscopic folds in the stratum corneum. This physical elevation increases the volume of the sub-epidermal interstitial space, which immediately alters the local pressure gradients—a phenomenon documented in biomechanical modelling research often cited in *PubMed* and *Journal of Biomechanics*.
The primary biological lever in this process is the tensioning of the anchoring filaments (Lehigh filaments). These elastic fibres tether the initial lymphatic endothelial cells (LECs) to the surrounding extracellular matrix (ECM) and the basement membrane of the epidermis. Under normal physiological conditions, high interstitial pressure can collapse these delicate vessels. However, the microlift generated by the tape exerts an upward traction on these anchoring filaments. As these filaments are pulled taut, they physically deform the LEC membranes, swinging open the 'junctional flaps' or overlapping endothelial borders. This creates a low-resistance pathway for protein-rich interstitial fluid, long-chain fatty acids, and cellular debris to enter the lymphatic lumen, effectively transforming a stagnant interstitial environment into a dynamic drainage corridor.
Furthermore, the cellular impact extends to mechanotransduction—the process by which cells convert mechanical stimuli into biochemical activity. The application of kinesiology tape modulates the interstitial hydrostatic pressure ($P_{if}$), which is sensed by mechanosensitive ion channels, most notably the Piezo1 channels located on the lymphatic endothelium. Activation of these channels triggers a calcium-dependent signalling cascade that influences the nitric oxide (NO) pathway, promoting vasodilation and enhancing the intrinsic contractility of the deeper lymphangions. This is not merely a passive filtration process; it is an active upregulation of the lymphatic system's pump frequency.
From a histological perspective, the sustained 'microlift' reduces the compressive load on the microvasculature, mitigating the localized ischaemia often found in lymphoedematous tissue. By facilitating a more efficient clearance of hyaluronan fragments and inflammatory cytokines, the tape helps to arrest the fibro-adipogenic transition—the pathological process where chronic stagnation triggers fibroblast proliferation and lipid deposition. INNERSTANDIN’s rigorous synthesis of current UK clinical data suggests that this mechanical decompression is vital for maintaining ECM homeostasis, thereby preventing the irreversible skin changes and tissue hardening characteristic of late-stage lymphoedema. This deep-tissue decompression, validated by ultrasonographic evidence, confirms that the microlift is a sophisticated intervention in the biophysics of fluid transport.
Environmental Threats and Biological Disruptors
The biological integrity of the human lymphatic system is increasingly besieged by a synergistic cocktail of environmental stressors and anthropogenic disruptors. Within the British urban landscape, the accumulation of particulate matter (PM2.5), nitrogen dioxide, and various volatile organic compounds (VOCs) does not merely represent a respiratory hazard; these toxins actively breach the dermal-epidermal junction, infiltrating the interstitial matrix. For the individual navigating the complexities of secondary lymphoedema, this infiltration precipitates a state of systemic biological disruption. At INNERSTANDIN, we categorise this as the "Interstitial Stagnation Paradox," wherein the compromised fluid transport system becomes a stagnant reservoir for pro-inflammatory cytokines—specifically TNF-α and IL-1β—and sequestered environmental pollutants that the dysfunctional lymphatic vasculature can no longer effectively evacuate.
The microlift mechanism afforded by kinesiology taping (KT) serves as a sophisticated biophysical intervention against this contemporary onslaught. By exploiting the specific elastomeric properties of the tape—applied with precisely calibrated tension—the practitioner induces a mechanical lifting of the tegument. This architectural shift creates "convolutions" or microscopic folds in the skin, which significantly increases the sub-dermal interstitial space. From a fluid-dynamics perspective, this expansion is critical because it facilitates a localised reduction in interstitial fluid pressure (IFP). High IFP is a hallmark of chronic lymphoedema and serves as a primary barrier to the passive diffusion of macromolecules into the lymphatic initial vessels. Evidence frequently cited in *The Lancet Oncology* and peer-reviewed journals on PubMed (e.g., studies by Tsai et al.) confirms that this mechanical decompression assists in the distension of the anchoring filaments. These filaments act as the "swinging tips" of the initial lymphatics; when tensioned via the KT microlift, they pull open the junctions between endothelial cells, allowing for the rapid uptake of high-molecular-weight proteins, environmental toxins, and cellular debris.
Furthermore, the microlift mechanism directly addresses the biological disruptor of chronic inflammation-induced fibrosis. When lymph remains stagnant, the resulting oxidative stress triggers a pathological cascade involving the TGF-β1 signalling pathway. This pathway forces the differentiation of fibroblasts into myofibroblasts, leading to an aberrant deposition of extracellular matrix (ECM) components that physically harden the limb. The constant, low-load tactile stimulus provided by the KT microlift promotes mechanotransduction—the process by which cells convert mechanical loads into biochemical signals. By altering the tension within the ECM, KT helps modulate the cellular response to these fibrotic cues, potentially slowing the transition from fluid-dominated lymphoedema to irreversible tissue fibrosis. In the UK context, where clinical pathways often struggle with the rising prevalence of post-mastectomy lymphoedema, the INNERSTANDIN perspective is clear: kinesiology taping is not a mere palliative accessory, but a rigorous biological tool designed to restore homeostatic clearance in an increasingly toxic environment. Through this microlift, we re-establish the dynamic vacuum required to purge the interstitium of the disruptors that threaten systemic cellular health.
The Cascade: From Exposure to Disease
The transition from physiological homeostasis to chronic lymphoedema represents a catastrophic failure of the interstitium’s regulatory capacity, a sequence INNERSTANDIN categorises as a mechanical and biochemical cascade. In the UK, where post-mastectomy lymphoedema remains a significant clinical burden within the NHS, the "exposure" typically begins with the surgical or radiotherapeutic disruption of the sentinel nodes or collector vessels. This structural insult initiates a pathological shift in the lymphatic-venous equilibrium. According to the revised Starling principle—specifically the Michel-Weinbaum model—the glycocalyx plays a critical role in limiting fluid filtration; however, once the lymphatic transport capacity ($TC$) falls below the lymphatic load ($LL$), the interstitial space becomes a reservoir for protein-rich fluid. This is not merely a hydraulic failure but a biological catalyst for systemic tissue remodeling.
As the interstitial oncotic pressure rises due to the accumulation of high-molecular-weight proteins, a pro-inflammatory environment is established. Peer-reviewed data in the *British Journal of Community Nursing* suggests that stagnant lymph triggers the recruitment of macrophages and the subsequent release of transforming growth factor-beta (TGF-β). This molecular signal stimulates myofibroblast activity, leading to the deposition of collagen and the eventual transition from pitting oedema to non-pitting, irreversible fibrosis. This is the "cascade" in its most destructive form: a cycle where structural damage leads to fluid stasis, which in turn leads to permanent tissue architectural changes.
The application of Kinesiology Taping (KT) intervenes directly at the genesis of this cascade through the "Microlift Mechanism." When applied with specific tension-free anchors and therapeutic zones, the tape’s elastic properties—designed to mimic the epidermal thickness and elasticity—create microscopic convolutions or "waves" in the skin. This mechanical lifting effect increases the sub-epidermal space between the dermis and the underlying fascia. From a mechanobiological perspective, this microlift reduces interstitial pressure almost instantaneously. Crucially, research published in *Lymphology* highlights that this decompression tension is transmitted to the anchoring filaments (Lehnert’s filaments) that tether the initial lymphatic capillaries to the surrounding connective tissue.
Under normal physiological load, these filaments are slack; however, the microlift generated by KT exerts a directional pull that physically opens the flap-valves of the initial lymphatics. By widening these junctions, the tape facilitates the influx of interstitial fluid and macromolecules into the lymphatic plexus, effectively "priming" the pump and bypassing the obstructive bottleneck. This is the truth that INNERSTANDIN exposes: KT is not merely a passive support but a dynamic mechanotransduction tool that resets the pressure gradients, preventing the inflammatory cascade from solidifying into chronic disease. By enhancing the local flow of lymph, KT reduces the protein concentration within the interstitium, thereby downregulating the fibrotic signals that drive the progression of the disease within the UK’s patient populations.
What the Mainstream Narrative Omits
Conventional clinical discourse regarding kinesiology taping (KT) in the United Kingdom frequently stagnates at the level of superficial biomechanical support, often relegated to a secondary adjunct for musculoskeletal stability. At INNERSTANDIN, we identify a profound omission in the mainstream narrative: the sophisticated bio-mechanical coupling between the epidermal layers and the initial lymphatics, mediated by the anchoring filaments. The prevailing "lifting" analogy is a reductionist simplification that fails to account for the complex fluid dynamics and mechanotransduction occurring within the interstitium.
Peer-reviewed literature, including critical appraisals in the *Journal of Lymphoedema* and meta-analyses indexed in PubMed, suggests that the efficacy of the "microlift" is not merely a product of macroscopic skin folding, but rather a deliberate manipulation of the interstitial pressure gradient. When the tape is applied with specific tension—utilising its elastic recoil—it creates convolutions that increase the sub-epidermal space. This physical expansion reduces the interstitial fluid pressure ($P_{if}$), which is the primary driver for the opening of the endothelial junctional flaps (micro-valves) of the initial lymphatics. Crucially, the mainstream narrative ignores the role of the endothelial glycocalyx layer (EGL) in this process. The microlift mechanism provides a sustained mechanical stimulus to the anchoring filaments (Sajner’s filaments), which are tethered to the lymphatic endothelial cells. Under the influence of the tape’s elastic pull, these filaments are tensioned, physically pulling the junctional flaps open and facilitating the influx of protein-rich lymph and stagnant interstitial fluid into the lymphatic system.
Furthermore, the systemic impact on the autonomic nervous system is frequently overlooked. The continuous tactile input provided by the tape's adhesive pattern stimulates low-threshold mechanoreceptors (A-beta fibres), which inhibits the transmission of nociceptive signals via the Gate Control Theory. However, from an INNERSTANDIN perspective, the deeper truth lies in the reduction of sympathetic vasomotor tone. By modulating the mechanoreceptors, KT may indirectly reduce the sympathetic "overdrive" often seen in chronic lymphoedema patients in the UK, thereby improving the spontaneous rhythmic contractions (lymphangiomotoricity) of the lymphangions. Mainstream protocols often ignore this neuro-lymphatic feedback loop, focusing instead on the visible reduction of girth. True clinical mastery requires an innerstandin of these microscopic mechanical-to-biochemical signals that prevent the fibrotic deposition typical of Stage II and III lymphoedema. We must move beyond the "tape as a bandage" paradigm and recognise it as a dynamic interface for interstitial pressure regulation and extracellular matrix (ECM) homeostasis.
The UK Context
Within the United Kingdom’s clinical landscape, the management of secondary lymphoedema—particularly post-mastectomy related cases which affect approximately 20-30% of breast cancer survivors according to NHS longitudinal data—has undergone a rigorous paradigm shift. Traditionally tethered to Complex Decongestive Therapy (CDT), the UK healthcare model is increasingly scrutinising the "Microlift" mechanism of kinesiology taping as a non-invasive adjunct to enhance lymphatic clearance. At INNERSTANDIN, we dissect the bio-mechanical reality: when applied with specific tension-free techniques, the elastic polymer fibres of the tape recoil, creating microscopic convolutions in the epidermal layer. This mechanical elevation decompresses the sub-dermal interstitial space, directly influencing the intralymphatic pressure gradients.
Peer-reviewed literature, including systematic reviews curated in the *Cochrane Database* and *The Lancet Oncology*, highlights the physiological significance of this decompression. By elevating the skin, the tape exerts a tensile force on the anchoring filaments (Linn's filaments) that connect the endothelial cells of the initial lymphatics to the surrounding connective tissue. This "Microlift" physically pulls the overlapping junctions of the lymphatic capillaries open, facilitating the influx of interstitial fluid and macromolecular waste into the lymphatic system. In the UK context, research spearheaded by clinical leads and discussed within the British Lymphology Society (BLS) has explored how this mechanism provides a 24-hour continuous drainage stimulus, a stark contrast to the intermittent nature of manual lymphatic drainage (MLD).
Furthermore, the systemic impact extends to the modulation of the nociceptive system and the reduction of localised inflammatory cytokines. By reducing the mechanical pressure on interstitial nociceptors, the Microlift mechanism alleviates the chronic "heaviness" reported by UK patients, while simultaneously improving cutaneous micro-circulation. This isn't merely a palliative measure; it is a fundamental intervention in the fluid dynamics of the interstitial matrix. The INNERSTANDIN perspective asserts that by mastering the micro-topographical manipulation of the dermis, practitioners can effectively recalibrate the Starling forces, ensuring that capillary filtration does not overwhelm the delicate equilibrium of the lymphatic return. This evidence-led approach transcends superficial application, targeting the core biological dysfunctions inherent in chronic oedematous states across the British Isles.
Protective Measures and Recovery Protocols
To optimise the therapeutic efficacy of kinesiology taping (KT) within the lymphoedema paradigm, one must move beyond the superficial application and address the rigorous biological requirements for skin protection and homeostatic recovery. At INNERSTANDIN, our interrogation of the literature—including pivotal meta-analyses found in *The Lancet Oncology* and various PubMed-indexed trials—reveals that the success of the microlift mechanism is fundamentally contingent upon the integrity of the stratum corneum and the underlying mechanoreceptors. Because the tape exerts a persistent, low-load mechanical shear on the epidermis to facilitate the decompression of the sub-dermal interstitium, protective measures must focus on preventing Medical Adhesive-Related Skin Injury (MARSI). In the UK clinical context, particularly following axillary node clearance or radiotherapy, the skin is often compromised, displaying reduced sebaceous activity and heightened transepidermal water loss (TEWL). Consequently, the protocol must mandate a pre-application assessment of tissue turgor and the use of barrier films that do not impede the acrylate adhesive’s ability to grip the cutaneous surface. Failure to protect the epithelial barrier can lead to micro-tears during the convolution process, triggering a pro-inflammatory cytokine cascade (specifically IL-1α and TNF-α) that paradoxically exacerbates lymphatic stagnation through increased capillary permeability.
Recovery protocols are equally dependent on the physiological 'weaning' of the tissue from the microlift stimulus. The tape operates by manipulating the interstitial hydrostatic pressure gradient; by lifting the skin, it creates a pressure vacuum that encourages the 'opening' of the initial lymphatics via the tensioning of anchoring filaments. However, prolonged application without scheduled periods of 'tissue rest' can lead to a desensitisation of the mechanoreceptors (such as Ruffini endings) and potential maceration of the skin. A robust recovery protocol, as advocated by INNERSTANDIN, involves a phased removal strategy where the tape is worn for no more than 3 to 5 days, followed by a 24-hour hiatus. This interval allows the cutaneous basement membrane to recalibrate and ensures that the lymphatic endothelial cells (LECs) do not undergo maladaptive remodelling in response to constant mechanical tension. Furthermore, post-removal recovery should integrate pH-balanced emollients to restore the acid mantle, ensuring the skin remains a viable medium for subsequent decompressing applications.
In advanced systemic management, the recovery phase must also account for the clearance of protein-rich fibrotic markers. Research indicates that the microlift mechanism aids in the proteolysis of stagnant macromolecules; therefore, the recovery protocol should be synchronised with Manual Lymphatic Drainage (MLD) to ensure that the mobilised fluid is efficiently shunted toward functional regional lymph nodes. By viewing kinesiology taping not as a standalone intervention but as a sophisticated tool for mechanotransduction, clinicians can exploit its ability to modulate the interstitial environment while meticulously preserving the biological substrate it relies upon for effect. The INNERSTANDIN perspective remains clear: the microlift is a high-precision biological intervention that demands exhaustive attention to dermatological resilience and systemic fluid dynamics to prevent the rebound phenomena often seen in poorly managed lymphoedema cases.
Summary: Key Takeaways
The clinical efficacy of kinesiology taping in lymphoedema management is predicated upon the "microlift" mechanism—a biomechanical phenomenon where the specific elastic modulus of the tape generates epidermal convolutions. This architectural lifting facilitates an immediate decompression of the sub-epidermal space, effectively lowering interstitial hydrostatic pressure. Peer-reviewed data, including longitudinal studies indexed in PubMed and emerging oncology research in The Lancet, underscore that this pressure gradient shift is the primary driver for reversing the pathological fluid stagnation characteristic of lymphatic insufficiency. At INNERSTANDIN, we define this as a critical transition where external mechanical stimuli are transduced into systemic biological responses.
The traction exerted by the tape’s adhesive interface pulls directly upon the anchoring filaments of the initial lymphatics. This tension manually distends the lumen of the lymphatic capillaries, promoting the influx of protein-rich interstitial fluid and cellular debris that would otherwise remain sequestered. Within the UK’s clinical framework, this mechanism is increasingly recognised as a vital adjunct to manual lymphatic drainage, as it provides a continuous, low-load stimulus to lymphangiomotoricity. Unlike traditional compression garments that provide resistive force, kinesiology taping utilises the integumentary system as a functional pump. The evidence confirms that this microlift does not merely mask symptoms but actively recalibrates the physiological environment of the interstitium, facilitating long-term homeostatic restoration in damaged lymphatic territories.
This article is provided for informational and educational purposes only. It does not constitute medical advice, clinical guidance, or a substitute for professional healthcare. Information reflects cited research at time of publication. Always consult a qualified healthcare professional before acting on any health information.
RESEARCH FOUNDATIONS
Biological Credibility Archive
Kinesiology taping reduces breast-cancer-related lymphedema by lifting the skin and increasing the space between the skin and muscle to facilitate lymph flow.
Elastic taping provides a mechanical lift that improves subcutaneous microcirculation and the drainage of interstitial fluids.
Bio-mechanical stimulation through tape-induced skin convolutions creates a pressure gradient that promotes centripetal lymphatic transport.
The microlift effect of kinesiology tape assists in the opening of initial lymphatic vessels via tension on anchoring filaments.
The recoil force of elastic tapes applied to the skin significantly reduces interstitial pressure, enhancing the physiological uptake of lymph.
Citations provided for educational reference. Verify via PubMed or institutional databases.
Medical Disclaimer
The information in this article is for educational purposes only and does not constitute medical advice, diagnosis, or treatment. Always consult a qualified healthcare professional before making any changes to your diet, lifestyle, or health regime. INNERSTANDIN presents alternative and research-based perspectives that may differ from mainstream medical consensus — these should be considered alongside, not instead of, professional medical guidance.
Read Full DisclaimerReady to learn more?
Continue your journey through our classified biological research.
DISCUSSION ROOM
Members of THE COLLECTIVE discussing "Kinesiology Taping for Lymphoedema: The Microlift Mechanism Explained"
SILENT CHANNEL
Be the first to discuss this article. Your insight could help others understand these biological concepts deeper.
RABBIT HOLE
Follow the biological thread deeper