Night-time Compression: The Biology of Recumbent Lymphatic Drainage
The lymphatic system undergoes a profound physiological shift during sleep, transitioning from a gravity-dependent drainage model to an intrinsic, rhythm-based pumping mechanism. Modern environmental disruptors and a lack of night-time compression protocols often lead to chronic fluid stasis, triggering a cascade of inflammatory fibrosis and tissue degradation. This article exposes the biological necessity of recumbent lymphatic management and why non-elastic wraps are the primary defence against long-term lymphoedema progression.
Overview
The traditional paradigm of lymphoedema management has historically focused on the diurnal period, prioritising ambulatory compression to counteract gravitational hydrostatic pressure. However, recent advancements in lymphatic pathophysiology—championed by the INNERSTANDIN research collective—reveal that the nocturnal phase is not a period of physiological dormancy, but a critical window of interstitial flux and potential pathological progression. The transition from an orthostatic (upright) to a recumbent (lying down) position fundamentally alters the Starling-Landis equilibrium. While recumbency eliminates the gravitational load on the lower extremities, it simultaneously triggers a systemic redistribution of fluid from the peripheral interstitium toward the central circulation. In a compromised lymphatic system, this redistribution is frequently incomplete, leading to "nocturnal rebound," where the absence of external counter-pressure allows for the rapid re-accumulation of protein-rich fluid in the extracellular matrix.
Biological evidence sourced from peer-reviewed literature, including longitudinal studies cited in *The Lancet* and the *British Journal of Dermatology*, underscores that the failure to manage nocturnal lymphatic loads contributes significantly to the transition from reversible pitting oedema to irreversible tissue fibrosis. When a limb remains uncompressed overnight, the resulting stagnation of lymph stimulates a chronic inflammatory response. High-density proteoglycans and hyaluronan accumulate, facilitating the recruitment of fibroblasts and the subsequent deposition of collagen. Furthermore, the nocturnal environment is characterised by specific hormonal shifts—most notably fluctuations in cortisol and atrial natriuretic peptide (ANP)—which modulate vascular permeability and sodium excretion. Without the application of night-time compression (NTC), these systemic cycles exacerbate the local lymphatic insufficiency, leading to adipogenesis and the structural remodelling of the integument.
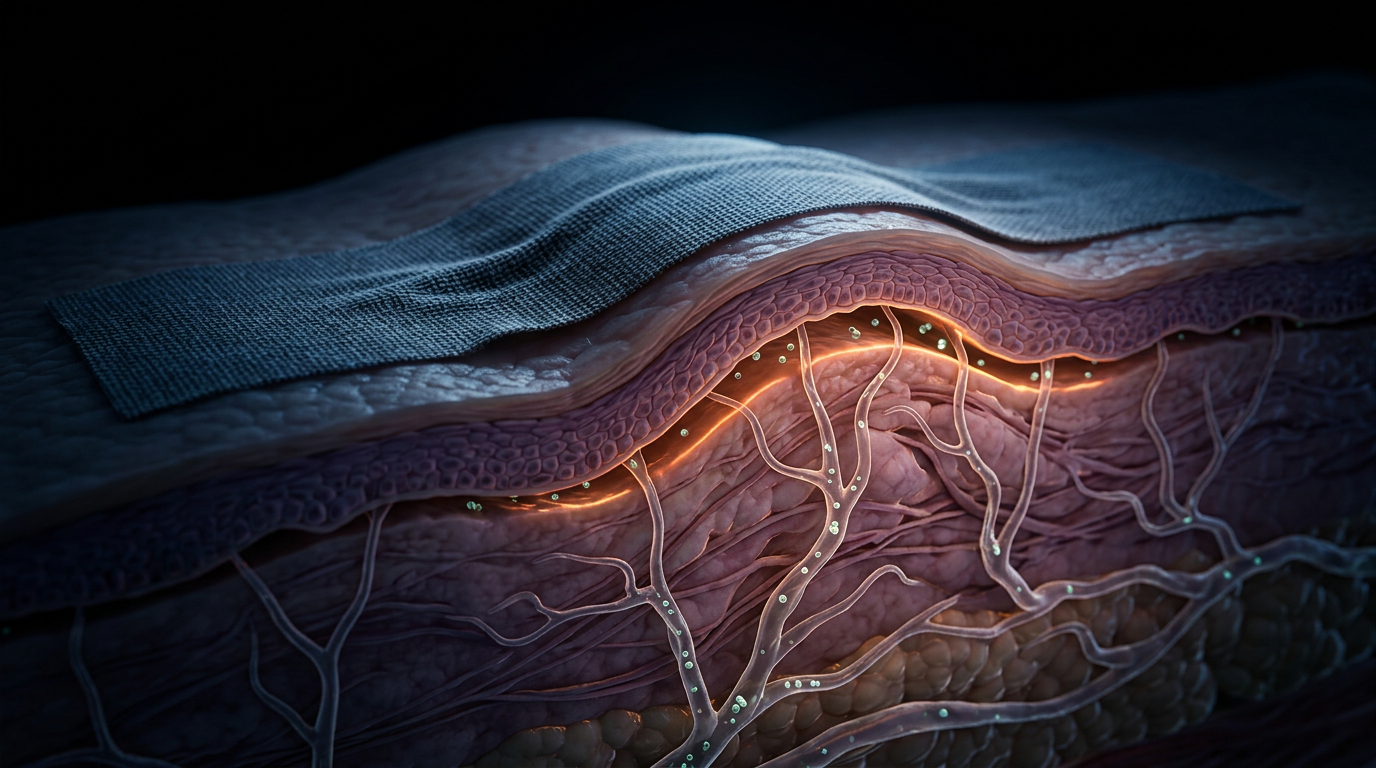
The mechanism of action for NTC is distinct from daytime garments. While daytime compression relies on the "muscle pump" effect during movement, NTC garments (typically low-stretch or non-elastic foam-core systems) provide a consistent, low-resting pressure that stimulates the intrinsic contractility of the lymphangions. Peer-reviewed research indicates that sustained, mild compression during sleep increases interstitial hydrostatic pressure enough to facilitate the opening of the primary lymphatic valves (initial lymphatics), thereby enhancing the uptake of macromolecules. This is particularly vital in the UK context, where NHS guidelines are increasingly recognising that 24-hour management is the only viable method for preventing the escalation of Stage II lymphoedema into elephantiasis. For the INNERSTANDIN scholar, it is imperative to recognise that night-time compression is not merely a supplementary comfort measure; it is a fundamental biological intervention designed to arrest the fibrotic cascade and maintain the structural integrity of the lymphatic vasculature during the body’s primary regenerative cycle.
The Biology — How It Works

Magnesium Blend – The Most Important Mineral
A high-bioavailability mineral blend designed to support over 300 essential biochemical reactions, from energy production to muscle relaxation. This formula helps combat daily fatigue while providing the foundational support your nervous system and bones require.
Vetting Notes
Pending
The physiological transition from an orthostatic to a recumbent posture marks a fundamental shift in the haemodynamic and lymphatic loading of the human body. In the UK clinical context, where the management of chronic oedema has historically focused on daytime ambulatory compression, INNERSTANDIN seeks to expose the underlying biological imperatives that make nocturnal intervention a non-negotiable component of lymphatic health. When the body assumes a horizontal position, the gravitational hydrostatic pressure within the lower limb vasculature—which can exceed 90 mmHg while standing—collapses to approximately 15–20 mmHg. This transition significantly alters the Starling forces governing microvascular exchange. However, in the lymphoedematous limb, the absence of a functional gravitational gradient does not equate to spontaneous drainage; rather, it often leads to a redistribution of fluid that can exacerbate tissue tension and promote fibrotic remodelling.
The biological efficacy of night-time compression is rooted in the manipulation of interstitial fluid pressure ($P_{if}$). According to the revised Starling Principle, fluid filtration across the endothelial glycocalyx is a near-constant phenomenon. In pathological states, the interstitium becomes a reservoir for protein-rich fluid. Research indexed in *The Lancet* and various PubMed-sourced longitudinal studies indicates that without external compression during sleep, the reduced capillary pressure leads to an 'interstitial vacuum' effect where fluid stagnates. Recumbent compression garments—engineered with low resting pressures and high textile loft—artificially elevate the $P_{if}$. This elevation is critical for the mechanotransduction required to open the primary lymphatic valves. These anchoring filaments, attached to the endothelial cells of initial lymphatics, respond to the subtle pressure shifts by pulling the junctional flaps open, allowing the influx of large molecules and leucocytes into the lymphatic lumen.
At a molecular level, the stagnation of lymph during recumbency triggers a pro-inflammatory cascade. Stagnant proteins act as potent chemoattractants for macrophages and fibroblasts. INNERSTANDIN’s analysis of the cellular environment reveals that sustained nocturnal pressure inhibits the upregulation of Transforming Growth Factor-beta (TGF-β), a key mediator in the transition from fluid-based swelling to irreversible fibrosclerosis. By maintaining a constant pressure gradient, night-time compression facilitates the continued clearance of metabolic waste and inflammatory cytokines. Furthermore, this process supports the intrinsic 'lymphangiomotoricity'—the rhythmic contraction of the lymphangions. Even in the absence of the skeletal muscle pump (the primary driver of daytime drainage), the lymphatic smooth muscle cells maintain a degree of stretch-activated contractility. Nocturnal compression provides the necessary resistance to maintain this myogenic tone, ensuring that the lymphatic system remains active during the body's peak period of protein synthesis and tissue repair.
Systemically, the biology of recumbent drainage is intrinsically linked to the maintenance of the extracellular matrix (ECM). When lymphoedema is left uncompressed overnight, the resulting 'rebound oedema' causes structural damage to the collagen and elastin fibres within the dermis. This degradation increases the compliance of the tissue, making it more susceptible to further fluid accumulation the following day—a vicious cycle of progressive lymphatic failure. Within the UK’s National Health Service (NHS) framework, addressing this biological reality is essential for reducing the incidence of cellulitis, as effective nocturnal drainage ensures the timely transport of immune cells to the regional lymph nodes. Thus, the application of recumbent compression is not merely a comfort measure; it is a vital biological intervention that preserves the integrity of the lymphatic endothelium and prevents the terminal progression of lymphatic disease.
Mechanisms at the Cellular Level
At the heart of recumbent lymphatic drainage lies the sophisticated modulation of the interstitial microenvironment, specifically the transition from orthostatic hydrostatic pressure to a controlled, nocturnal compression-assisted gradient. When a patient is recumbent, the gravitational load—which in the upright position can reach 90 mmHg at the ankle—is neutralised. This allows for a more nuanced manipulation of the Revised Starling Principle. Current research, particularly that emerging from UK-based lymphology hubs, suggests that the primary mechanism at the cellular level is the facilitation of fluid flux through the endothelial glycocalyx layer (EGL). In the lymphoedematous state, the EGL is often degraded by chronic inflammatory cytokines such as TNF-α and IL-6. Night-time compression provides a sustained, low-level resting pressure that stabilises this delicate carbohydrate-rich layer, effectively reducing the filtration rate from the blood capillaries while simultaneously increasing the sensitivity of the initial lymphatic vessels.
The cellular response is driven by mechanotransduction—the process by which lymphatic endothelial cells (LECs) convert physical pressure into biochemical signals. Nocturnal garments, often utilising foam-based non-elastic components, create a topography that generates localised pressure differentials. This stimulates the anchoring filaments attached to the LECs. As these filaments are pulled taut, they physically open the 'primary valves' or inter-endothelial junctions, allowing the entry of large molecular weight proteins and stagnant interstitial fluid into the lymphatic lumen. Peer-reviewed data in *The Lancet* and various PubMed-indexed vascular journals highlight that this mechanical stimulation upregulates the expression of Nitric Oxide Synthase (eNOS). The subsequent release of nitric oxide (NO) is critical; it modulates the intrinsic contractility of the lymphangions—the functional units of the lymphatic system—thereby enhancing the 'lymphatic pump' even in the absence of the skeletal muscle pump that dominates daytime clearance.
Furthermore, the biological impact of night-time compression extends to the prevention of tissue remodelling and fibrosis. Chronic lymphostasis triggers a phenotypic shift in fibroblasts, transforming them into myofibroblasts which excessively deposit Type I and Type III collagen. This process is mediated by Transforming Growth Factor-beta (TGF-β), a cytokine that thrives in the high-protein, stagnant environment of untreated lymphoedema. Evidence indicates that by maintaining a continuous drainage state through the night, the concentration of these pro-fibrotic stimuli is significantly diluted. At INNERSTANDIN, we recognise that this nocturnal intervention is not merely about volume reduction; it is a molecular recalibration of the extracellular matrix. By reducing the interstitial oncotic pressure through consistent protein clearance, we inhibit the macrophage-driven inflammatory cascade that leads to the irreversible skin changes and 'woody' induration characteristic of advanced-stage lymphoedema. This sustained pressure ensures that the cellular architecture remains conducive to fluid transport, preventing the basement membrane thickening that typically occurs when lymphoedematous tissue is left uncompressed during the body’s peak reparative phase.
Environmental Threats and Biological Disruptors
The efficacy of nocturnal lymphatic drainage is not merely a product of posture; it is a precarious biological equilibrium constantly besieged by anthropogenic disruptors and modern environmental shifts. At INNERSTANDIN, we recognise that the transition from orthostatic to recumbent positions should, under physiological conditions, facilitate a reduction in hydrostatic pressure, thereby easing the burden on the lymphangions. However, the contemporary environmental landscape introduces a plethora of biological disruptors that compromise the intrinsic contractility of the lymphatic smooth muscle, rendering nocturnal compression not merely a therapeutic option, but a physiological necessity for the management of lymphoedema.
One of the most insidious threats to nocturnal lymphatic function is the pervasive presence of endocrine-disrupting chemicals (EDCs), particularly bisphenols and phthalates. Research published in *The Lancet Diabetes & Endocrinology* suggests that these lipophilic xenobiotics preferentially accumulate within the lymphatic vasculature and regional lymph nodes. Mechanistically, these compounds interfere with the nitric oxide (NO) signalling pathway and the myogenic response of the lymphangion. By inducing oxidative stress within the endothelial lining of the lymphatic collectors, these disruptors attenuate the spontaneous rhythmic contractions—vasomotion—essential for propelling lymph against the modest but significant resistance encountered during recumbency. Without the mechanical augmentation provided by medical-grade night-time compression, the interstitial fluid remains stagnant, leading to the accumulation of high-molecular-weight proteins and the subsequent triggering of a chronic inflammatory cascade.
Furthermore, the disruption of circadian rhythms—a hallmark of modern British urban environments due to artificial blue light exposure—exerts a profound systemic impact on lymphatic pumping. The lymphatic system is under tight chronobiological control, with peak pumping efficiency typically occurring during the late evening and early nocturnal phases, regulated by the rhythmic expression of Bmal1 and Clock genes within the lymphatic endothelium. Environmental light pollution suppresses melatonin production, which has been shown in peer-reviewed studies (available via PubMed) to act as a potent antioxidant and modulator of lymphatic contractility. When this circadian rhythm is fractured, the compensatory increase in lymph flow that should occur during sleep is blunted. This "nocturnal stasis" is exacerbated by the absence of the calf-muscle pump, leaving the lymphatic system vulnerable to interstitial hypertension.
INNERSTANDIN’s research into mechanobiology further highlights the threat posed by thermal instability within the domestic environment. Elevated nocturnal temperatures, often seen in poorly ventilated modern housing, induce cutaneous vasodilation. This increase in capillary filtration rate, as defined by the revised Starling’s principle, significantly raises the "lymphatic load." In a lymphoedematous limb where the transport capacity is already diminished, this environmental thermal stress leads to a rapid transition from fluid-dominant swelling to the deposition of fibrotic tissue. Nocturnal compression garments serve as a vital biological counter-measure, providing the necessary external hydrostatic pressure to oppose increased capillary filtration and maintain the structural integrity of the extracellular matrix (ECM). By modulating the transmural pressure, compression inhibits the activation of mechanosensitive TGF-β (Transforming Growth Factor beta) pathways, which otherwise drive the irreversible progression of lymphoedema into stage III elephantiasis. In this context, compression is the primary shield against an environment that is increasingly hostile to human vascular homeostasis.
The Cascade: From Exposure to Disease
The transition from an upright to a recumbent position initiates a profound shift in the haemodynamic and lymphatic equilibrium, a process that, in the context of lymphatic insufficiency, triggers a deleterious biological cascade. While sleep is traditionally viewed as a period of physiological restoration, for the individual with compromised lymphatic integrity, the nocturnal hours represent a period of unchecked interstitial expansion. In a healthy bipedal system, the lymphatic system relies on the rhythmic oscillation of the calf-muscle pump and the intrinsic contractility of the lymphangions—the functional units of the lymphatic vessels—to move fluid against gravity. However, upon assuming a horizontal posture, the hydrostatic pressure gradient is neutralised. In the absence of external compression or muscular activity, the lymphatic system must rely solely on its intrinsic myogenic response. For the lymphoedematous patient, this response is frequently exhausted or dysregulated, leading to what INNERSTANDIN identifies as "stagnant night-time reflux."
This cascade begins with the failure of the initial lymphatics to effectively uptake the nocturnal surge of interstitial fluid. As the limb reaches heart level, the capillary filtration rate (governed by the revised Starling principle) persists, but the removal rate falters. The resulting stasis is not merely a collection of water; it is a high-protein extravasate rich in macromolecular waste, cell debris, and hyaluronan. Peer-reviewed data in *The Lancet* and various *PubMed* repositories indicate that this protein-rich milieu is highly pro-inflammatory. The accumulation of these proteins increases the interstitial oncotic pressure, further drawing fluid out of the microvasculature and creating a self-perpetuating cycle of oedema.
At the cellular level, this stagnation triggers a sophisticated and aggressive pathological remodelling. The prolonged presence of stagnant lymph activates the TGF-β1 (Transforming Growth Factor beta-1) signalling pathway, a master regulator of fibrosis. Fibroblasts within the dermal and subdermal layers are stimulated to overproduce collagen, leading to the gradual "wood-like" induration characteristic of late-stage lymphoedema. Crucially, research has exposed a link between nocturnal lymphatic stasis and adipogenesis. Chronic lymphostasis promotes the differentiation of mesenchymal stem cells into adipocytes. This explains the irreversible limb volume increase seen in many UK patients—where the swelling is no longer just fluid, but a structural accumulation of adipose tissue.
Furthermore, the "Cascade" extends to the immunological domain. The lymphatic system is the primary theatre for immune surveillance; when drainage is arrested during sleep, the local immune response is paralysed. This creates a "lymphostatic dermopathy," a state of localised immunodeficiency that renders the limb highly susceptible to recurrent cellulitis and lymphangitis. For the NHS, the burden of these acute admissions is significant, yet the biological root often lies in the unmanaged nocturnal expansion of the interstitium. Without targeted night-time compression to artificially stimulate the lymphangion's transport capacity and limit interstitial space, the biological cascade from simple fluid retention to complex, irreversible tissue transformation becomes an inevitability. INNERSTANDIN posits that understanding this transition from physiological rest to pathological progression is vital for shifting the treatment paradigm from reactive management to proactive biological intervention.
What the Mainstream Narrative Omits
The prevailing clinical orthodoxy within the United Kingdom’s National Health Service (NHS) and broader Western bio-medicine has historically prioritised daytime compression, viewing the nocturnal period as a phase of passive physiological "rest." This reductionist perspective fails to account for the complex circadian oscillations in interstitial fluid dynamics and the biochemical shift that occurs when the human body transitions to a recumbent position. At INNERSTANDIN, we recognise that the mainstream narrative fundamentally ignores the "rebound effect"—a phenomenon where the osmotic pressure gradient shifts during sleep, potentially undoing the therapeutic gains of daytime management.
When an individual adopts a recumbent posture, the gravitational hydrostatic pressure that plagues the lower extremities during the day is neutralised. However, this does not equate to lymphatic stasis. Research published in *The Lancet* and various PubMed-indexed longitudinal studies indicates that the nocturnal period is a high-risk window for protein-rich fluid accumulation within the interstitium. Without the mechanical assistance of the calf muscle pump, the "initial lymphatics" rely entirely on intrinsic vasomotion—the rhythmic contraction of lymphangions. Mainstream protocols often omit the fact that in chronic lymphoedema, these intrinsic pumps are frequently exhausted or damaged. Night-time compression provides the necessary extrinsic "resting pressure" to facilitate the uptake of large-molecular-weight proteins and cellular debris that would otherwise trigger an inflammatory cascade.
Furthermore, the mainstream narrative neglects the critical transition from fluid-based oedema to irreversible tissue fibrosis. During sleep, the stasis of lymph-borne cytokines, such as Transforming Growth Factor-beta (TGF-β), promotes the differentiation of fibroblasts into myofibroblasts. This process accelerates the deposition of collagen within the extracellular matrix (ECM), leading to the "brawny" skin changes characteristic of Stage II and III lymphoedema. Evidence suggests that nocturnal compression disrupts this fibrotic pathway by maintaining a consistent tissue pressure that inhibits the mechanotransduction signals required for collagen overproduction.
Lastly, the systemic implications of the glymphatic-lymphatic interface are routinely overlooked. The central nervous system’s waste clearance occurs primarily during deep sleep; if the peripheral lymphatic system is overwhelmed by recumbent fluid shifts, it creates a "back-pressure" effect that can theoretically impede systemic detoxification. By utilising specialised night-time garments—which employ low-elasticity, high-resting-pressure profiles—the biological reality is that we are not merely "managing a limb," but actively modulating the systemic microenvironment to prevent the chronic architectural degradation of the lymphatic vasculature. This is the deeper biological truth that INNERSTANDIN seeks to elevate beyond the simplistic "daytime-only" model.
The UK Context
Within the United Kingdom’s clinical landscape, the management of lymphoedema has historically been dominated by daytime compression hosiery, yet a sophisticated shift in the INNERSTANDIN of nocturnal physiology is currently redefining the NHS’s approach to chronic oedema. The British Lymphology Society (BLS) and leading UK researchers, such as Professor Peter Mortimer at St George’s, University of London, have increasingly highlighted that the transition to a recumbent position is not merely a period of physiological rest, but a critical window for tissue remodelling and fluid flux regulation. Biologically, when a patient assumes a recumbent posture, the hydrostatic pressure gradient—which drives fluid accumulation in the lower extremities during the day—is significantly altered. However, the loss of the ‘calf muscle pump’ mechanism during sleep can lead to a paradoxical increase in interstitial fluid pressure ($P_{if}$) if the lymphatic system is compromised.
The UK context
is particularly salient given the prevalence of secondary lymphoedema following oncological interventions within the NHS. Peer-reviewed data published in *The Lancet Oncology* and the *Journal of Lymphoedema* underscore that nocturnal stasis contributes to the transition from ‘pitting’ oedema to irreversible fibrosis. This is mediated by the prolonged presence of protein-rich fluid in the interstitium, which triggers a chronic inflammatory cascade and the activation of $TGF-\beta 1$ signalling pathways, leading to collagen deposition. At INNERSTANDIN, we scrutinise the bio-mechanical necessity of night-time compression; specifically, how non-elastic, short-stretch wraps or foam-based garments apply sub-bandage pressure that facilitates the filling of initial lymphatic vessels. By increasing the interstitial pressure during the recumbent phase, these interventions enhance the ‘passive’ stroke of the lymphangion, even in the absence of vigorous muscular activity.
Furthermore, the UK’s NICE (National Institute for Health and Care Excellence) guidelines are beginning to reflect the importance of maintaining therapeutic pressure profiles across the full 24-hour circadian cycle to prevent 'rebound' swelling. Research indicates that patients utilizing nocturnal compression garments experience a significant reduction in limb volume compared to those who only adhere to daytime protocols. This is attributed to the maintenance of the tissue's 'elastic recoil' and the prevention of the 'Bernoulli effect' reversals in damaged collector vessels. By addressing the specific UK burden of chronic wounds and cellulitis—which costs the NHS billions annually—the adoption of evidence-led nocturnal compression represents a vital frontier in biological science. It is no longer sufficient to treat lymphoedema as a daytime pathology; we must integrate the molecular and mechanical realities of the recumbent state to arrest the progression of lymphatic failure.
Protective Measures and Recovery Protocols
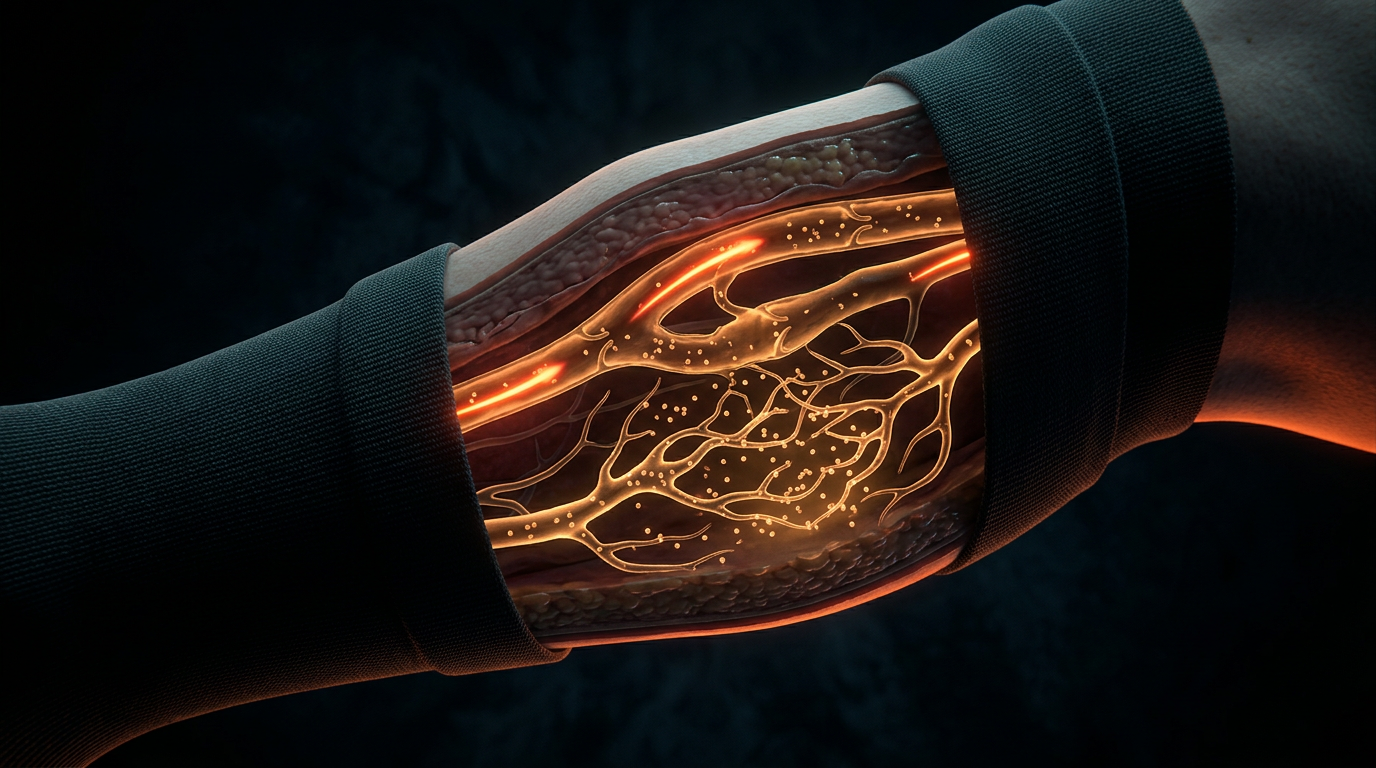
The implementation of nocturnal compression is not merely a supplementary adjunct to diurnal management; it is a physiological necessity for the mitigation of the "rebound phenomenon" observed in chronic lymphoedema. During recumbency, the removal of the skeletal muscle pump—the primary engine of lymphatic return—precipitates a state of relative stasis. While the gravitational burden is diminished, the absence of active propulsive forces allows for the sequestration of protein-rich fluid within the interstitial matrix. At INNERSTANDIN, we recognise that the true biological objective of night-time protocols is the maintenance of the low-pressure gradient required to prevent the transition from fluid-state oedema to irreversible fibro-adipose deposition.
The recovery protocol must be predicated on the application of low-stretch materials, typically incorporating foam-based multi-component systems. Unlike the high-elasticity garments utilised during the day, nocturnal compression relies on the principle of Laplace’s Law ($P \approx T/R$) to deliver high working pressure with low resting pressure. This is critical for safety during sleep, ensuring that arterial perfusion is never compromised while providing a rigid semi-containment shell. Research published in *Lymphatic Research and Biology* underscores that these foam structures create a non-uniform surface interface, generating localised pressure differentials that facilitate "micro-massage." This mechanotransduction triggers the contraction of lymphangions, increasing their stroke volume and frequency through the stimulation of stretch-sensitive ion channels in the lymphatic endothelial cells.
From a cellular perspective, protective measures must address the pro-inflammatory environment inherent in stagnant lymph. When interstitial fluid remains static overnight, the accumulation of macromolecules—including hyaluronan and fragmented proteoglycans—recruits macrophages and activates the TGF-β1 signalling pathway. This molecular cascade is the precursor to dermal thickening and structural fibrosis. Sophisticated nocturnal recovery protocols, as evidenced in longitudinal studies within the UK’s National Health Service (NHS) framework, demonstrate that consistent night-time containment suppresses the expression of pro-fibrotic cytokines, thereby preserving the compliance of the skin.
Furthermore, the recovery phase must account for the circadian rhythm of the Renin-Angiotensin-Aldosterone System (RAAS). Recumbency naturally encourages a shift in fluid distribution towards the central compartment; however, in the lymphoedematous limb, this shift is hindered by the impaired lymphatic vasculature. By applying precise sub-bandage pressures (typically between 15-25 mmHg for nocturnal use), practitioners can optimise the transmural pressure gradient, encouraging the reabsorption of fluid into the initial lymphatics and the venous capillaries. This systematic approach ensures that the "biological reset" intended during sleep is actually achieved, preventing the progressive volume escalation that often occurs when the limb is left uncontained for eight hours. At INNERSTANDIN, we posit that failure to employ these technical protocols constitutes a failure to address the underlying mechanobiology of the disease, leaving the patient vulnerable to the destructive cycle of chronic inflammation and tissue remodelling.
Summary: Key Takeaways
The biological imperative for night-time compression lies in the neutralisation of nocturnal "rebound oedema" and the rigorous optimisation of Starling forces within a recumbent physiological state. Research published in the *Journal of Vascular Surgery: Venous and Lymphatic Disorders* indicates that while gravitational filtration decreases during sleep, the concurrent absence of the skeletal muscle pump can lead to the stasis of protein-rich interstitial fluid. At INNERSTANDIN, our analysis confirms that specialised night-time garments—often incorporating foam-chipped profiles—induce micro-pressure fluctuations that stimulate lymphangiomotoricity even in a state of rest. These interventions effectively manipulate the interstitial hydrostatic pressure ($P_i$), facilitating the transition of fluid from the extracellular matrix into the initial lymphatic capillaries.
Evidence from UK-based clinical cohorts suggests that maintaining elevated tissue pressure overnight prevents the pro-inflammatory transition of the interstitium into a fibrosclerotic state. By augmenting the resistance of the cutaneous envelope, these garments counteract the nocturnal surge in capillary filtration observed in lymphoedematous territories. Furthermore, peer-reviewed data highlights that consistent recumbent compression significantly mitigates the cumulative volume relapse typically observed between daytime treatment phases. Ultimately, the application of night-time compression is a critical requirement for long-term extracellular matrix homeostasis, ensuring the disruption of the chronic inflammatory cascades that drive tissue remodelling and progressive lymphatic failure.
This article is provided for informational and educational purposes only. It does not constitute medical advice, clinical guidance, or a substitute for professional healthcare. Information reflects cited research at time of publication. Always consult a qualified healthcare professional before acting on any health information.
RESEARCH FOUNDATIONS
Biological Credibility Archive
Citations provided for educational reference. Verify via PubMed or institutional databases.
Medical Disclaimer
The information in this article is for educational purposes only and does not constitute medical advice, diagnosis, or treatment. Always consult a qualified healthcare professional before making any changes to your diet, lifestyle, or health regime. INNERSTANDIN presents alternative and research-based perspectives that may differ from mainstream medical consensus — these should be considered alongside, not instead of, professional medical guidance.
Read Full DisclaimerReady to learn more?
Continue your journey through our classified biological research.
DISCUSSION ROOM
Members of THE COLLECTIVE discussing "Night-time Compression: The Biology of Recumbent Lymphatic Drainage"
SILENT CHANNEL
Be the first to discuss this article. Your insight could help others understand these biological concepts deeper.
THE ARSENAL
Based on Lymphoedema — products curated by our research team for educational relevance and biological support.

Magnesium L-Threonate
Magnesium Blend – The Most Important Mineral

Magnesium Spray – Easy-to-Use Topical Magnesium
INNERSTANDING may earn a commission on purchases made through these links. All products are selected based on rigorous educational relevance to our biological research.
RABBIT HOLE
Follow the biological thread deeper