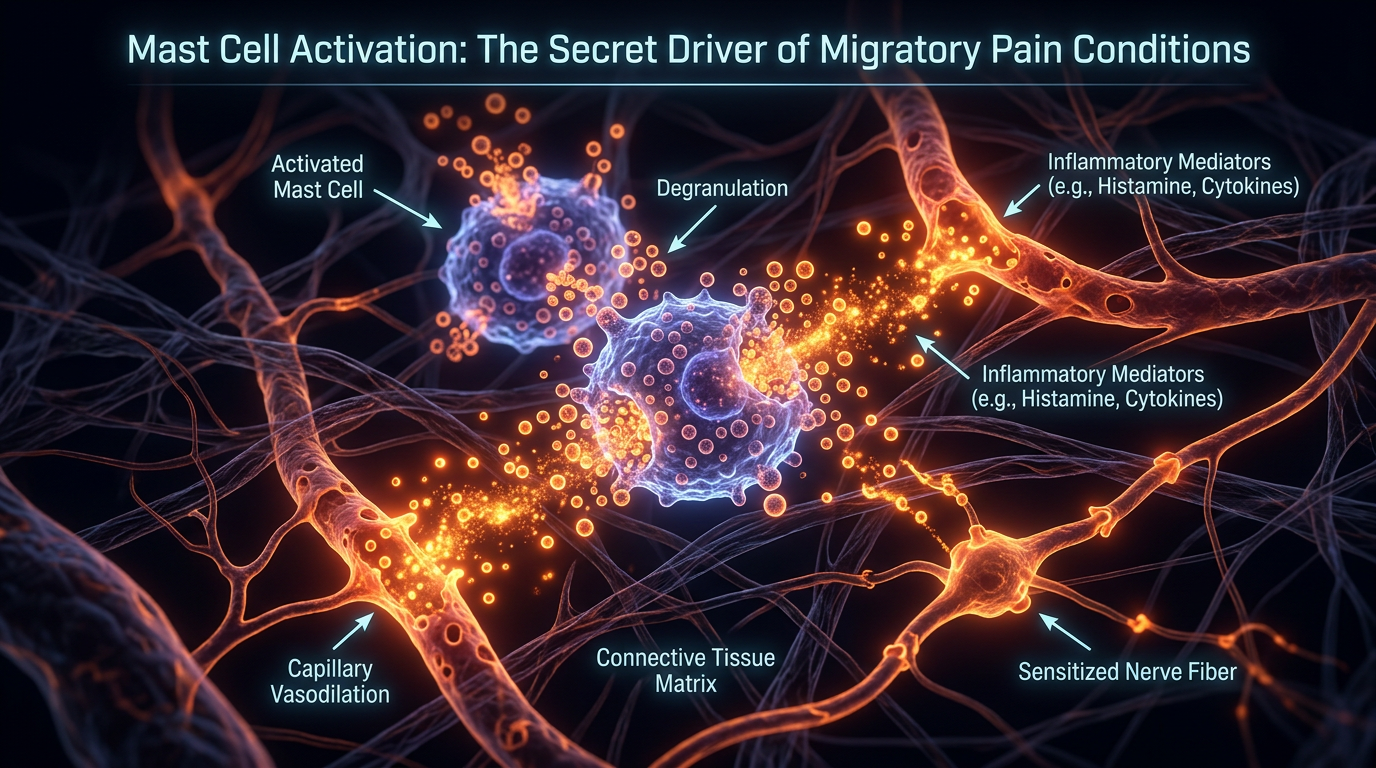
Mast Cell Activation: The Secret Driver of Migratory Pain Conditions
Mast cells are known for allergies but also release a cocktail of pro-inflammatory mediators that can trigger migratory pain. This under-diagnosed activation is a common thread in systemic chronic pain syndromes.
Overview
For decades, the medical establishment has viewed the human immune system through a remarkably narrow lens. In this traditional paradigm, the immune system is a reactive force—an army that sleeps until an invader, like a virus or bacterium, breaches the walls. Within this framework, Mast Cells have been relegated to the role of "allergy cells," the inconvenient biological actors responsible for hay fever, hives, or, in extreme cases, anaphylactic shock. This reductionist view has not only stalled our understanding of systemic health but has actively obscured the primary driver behind one of the most baffling phenomena in modern clinical practice: Migratory Pain.
Migratory pain—characterised by debilitating discomfort that moves from a shoulder to a hip, from a joint to a muscle group, appearing and disappearing with no clear mechanical injury—has long been the "ghost in the machine" for general practitioners. When standard blood tests for inflammatory markers like C-Reactive Protein (CRP) or Erythrocyte Sedimentation Rate (ESR) return normal results, patients are frequently dismissed. They are often told their pain is "psychosomatic," or are slapped with a generic label of "fibromyalgia" or "central sensitisation," labels that describe the symptoms without ever identifying the underlying mechanism.
However, emerging research at the intersection of neurobiology and immunology points to a single, insidious culprit: Mast Cell Activation Syndrome (MCAS).
Mast cells are not merely "allergy cells"; they are the masterful conductors of the body’s internal alarm system. Residing at the interface of our internal and external environments—the skin, the gut lining, the respiratory tract, and the blood-brain barrier—these cells are uniquely positioned to sense environmental threats. When they become dysregulated, they do not simply cause a sneeze or a rash. They release a devastating "chemical cocktail" of over 200 pro-inflammatory mediators, including histamine, tryptase, prostaglandins, and cytokines.
This article exposes how the inappropriate and chronic degranulation of mast cells triggers a systemic inflammatory firestorm that travels through the connective tissues and the nervous system. This is the biological reality of migratory pain. It is not "all in your head"; it is in your mast cells. By understanding this secret driver, we can finally dismantle the mystery of chronic systemic pain and move toward a model of true biological restoration.
UK STATISTIC: It is estimated that approximately 28 million adults in the UK suffer from some form of chronic pain, yet fewer than 15% receive a diagnosis that accounts for the multi-systemic, migratory nature of their symptoms.
---
##
The Biology — How It Works
To understand why mast cells drive migratory pain, one must first appreciate their evolutionary pedigree. Mast cells are ancient. They predate the adaptive immune system (the part of our immunity that remembers specific viruses) by hundreds of millions of years. This means they are part of our "innate" immune system—the primitive, fast-acting first responders that detect "danger" rather than specific "germs."
The Sentinels of the Interstitium
Mast cells are strategically located in the interstitium—the fluid-filled space between the skin and the internal organs, and throughout the fascia (the connective tissue webbing that holds us together). Because the fascia is a continuous network throughout the entire body, any chemical signal released into this "highway" can theoretically travel anywhere. This is the first clue as to why mast cell-driven pain is migratory.
Unlike other immune cells that circulate in the blood, mast cells are fixed in tissue. However, they are positioned directly adjacent to blood vessels and, crucially, nerve endings. This proximity is not accidental. The "Mast Cell-Nerve Unit" is a bidirectional communication hub. When a mast cell detects a threat—be it a toxin, a change in pressure, or a stress hormone—it releases mediators that directly stimulate the adjacent nociceptors (pain-sensing nerves).
The "Allergy" Misconception
The primary reason the mainstream narrative fails is the over-reliance on IgE-mediated responses. In a classic allergy, the body produces IgE antibodies to something like pollen. When pollen hits a mast cell, it "pops" (degranulates) and releases histamine.
However, in Mast Cell Activation Syndrome (MCAS), the mast cells have become "hyper-excitable." They no longer require an IgE antibody to fire. They can be triggered by a vast array of non-allergic stimuli: temperature changes, emotional stress, vibration, electromagnetic frequencies (EMFs), and chemical fragrances. When these cells fire in a disorganised, systemic fashion, the pain they produce is not localised to a single "injury" site but follows the path of the systemic inflammatory cascade.
---
##
Mechanisms at the Cellular Level
The "secret" of migratory pain lies in the specific biochemistry of what mast cells release and how those chemicals interact with the peripheral and central nervous systems.
The Chemical Cocktail
When a mast cell is triggered, it doesn't just release one thing. It undergoes a process called degranulation, or more subtly, differential secretion. It can "choose" which mediators to release based on the type of threat it perceives.
- —Histamine: This is a potent vasodilator. It makes blood vessels "leaky." When vessels leak in the tissues, it causes localised swelling (oedema) that puts physical pressure on nerves. Histamine also lowers the "firing threshold" of pain nerves, making them hypersensitive to even the slightest movement.
- —Tryptase: This enzyme breaks down the extracellular matrix (the "glue" between cells). If mast cells are chronically active in the joints or fascia, tryptase can cause micro-damage to the connective tissue, leading to a feeling of "structural" pain where no injury exists.
- —Prostaglandins (specifically PGD2): These are perhaps the most potent drivers of the "aching" sensation common in migratory pain conditions.
- —Cytokines and Chemokines: These are signalling molecules that recruit *other* immune cells to the area, creating a localized "pocket" of inflammation that can persist for days before the mast cells in that area finally calm down—only for mast cells in a different limb to ignite.
The Mast Cell-Nerve Cross-Talk
The most profound mechanism behind migratory pain is the Neuro-Immune Loop. Mast cells release a substance called Substance P and Nerve Growth Factor (NGF).
Substance P is a neuropeptide that acts as a powerful pain transmitter. When mast cells release it, it stimulates the nerve. In a "vicious cycle," the stimulated nerve then releases its own neuropeptides, which travel back to the mast cell and tell it to release *more* histamine. This creates a self-sustaining loop of pain.
Because the nervous system is interconnected, a "flare" in one area (say, the gut) can cause "referred" activation of mast cells along the spinal cord, leading to pain in the extremities. This is why a patient may experience a "migrating" pain that seems to jump across the body; it is the inflammatory signal travelling through the neural-fascial network.
The Role of the Blood-Brain Barrier
Mast cells also reside on the brain side of the Blood-Brain Barrier (BBB). When systemic mast cell activation occurs, these mediators can increase the permeability of the BBB, allowing inflammatory chemicals into the Central Nervous System (CNS). This leads to Neuroinflammation, which manifests as "brain fog," cognitive dysfunction, and a heightened state of "central sensitisation," where the brain begins to amplify all pain signals coming from the body.
---
##
Environmental Threats and Biological Disruptors
In a vacuum, mast cells are our protectors. Why, then, have they become the "secret drivers" of chronic disease in the 21st century? The answer lies in our "mismatched" environment. Our ancient mast cells are being bombarded by modern stimuli they were never evolved to handle.
The Mycotoxin Menace (The UK’s Hidden Crisis)
In the United Kingdom, environmental mold (mycotoxins) is a primary driver of MCAS. Due to the UK's damp climate and aging, poorly ventilated housing stock, millions are living in "sick buildings." Mycotoxins are potent mast cell triggers. Unlike bacteria, which the immune system can often clear, mycotoxins act as "ionophores," disrupting the delicate calcium signalling within mast cells and keeping them in a state of constant, low-level degranulation.
EMFs and Cellular Vibration
Emerging research suggests that mast cells are sensitive to Electromagnetic Frequencies (EMFs). The voltage-gated calcium channels (VGCCs) on the surface of mast cells can be forced open by non-ionizing radiation from mobile phones, Wi-Fi, and smart meters. When these channels stay open, calcium floods the cell, triggering the release of inflammatory mediators. This explains why many sufferers of migratory pain report that their symptoms worsen in high-tech urban environments.
The "Chemical Soup" of Modern Living
- —Adjuvants and Preservatives: Modern processed foods are loaded with "histamine releasers" and preservatives like sodium benzoate and tartrazine.
- —Microplastics: Recent studies have shown that microplastics can accumulate in the interstitium, where they act as physical "irritants" that mast cells attempt to "attack," leading to chronic local inflammation.
- —Fragrance and Volatile Organic Compounds (VOCs): The ubiquitous use of synthetic "air fresheners" and perfumes provides a constant "sensory trigger" for mast cells in the respiratory tract, which then signal the rest of the systemic mast cell population to go on high alert.
ALARMING FACT: The average modern Briton is exposed to over 500 synthetic chemicals daily—many of which have been shown in laboratory settings to trigger mast cell degranulation even at "sub-toxic" levels.
---
##
The Cascade: From Exposure to Disease
The progression from "sensitive person" to a patient with "migratory pain syndrome" follows a predictable biological cascade. Understanding this timeline is essential for reversing the process.
Phase 1: The "Bucket" Fills
We often use the "Histamine Bucket" analogy. Everyone has a bucket. Your genetics, your gut health, and your environment determine the size of your bucket. Throughout life, you add "water" to the bucket: a round of antibiotics, a stressful divorce, a moldy flat, a viral infection. For years, you feel fine because the bucket hasn't overflowed.
Phase 2: The Threshold Event
Usually, a single major event—a "perfect storm"—causes the bucket to overflow. This might be a severe bout of the flu, a period of extreme emotional trauma, or a significant toxic exposure. At this point, the mast cells become "primed." Priming is a biological state where the cell’s internal machinery is wound tight, like a spring. It now takes only a tiny nudge to cause a massive release of chemicals.
Phase 3: Systemic Sensitisation
Once mast cells are primed, the pain begins to "migrate." Because the cells are hyper-reactive, a trigger in the gut (like eating a piece of aged cheese) causes a systemic release of mediators. These mediators travel through the fascia and settle in areas of "least resistance"—perhaps an old injury site or a joint that is slightly misaligned.
The patient feels pain in their knee. Three days later, the knee feels fine, but the pain has moved to the jaw (TMJ). This is not the "injury" moving; it is the wave of mast cell degranulation moving through the body’s connective tissue system.
Phase 4: The Neurological Lock-In
If the cascade continues, the Central Nervous System becomes involved. The constant barrage of mast cell mediators "rewires" the pain processing centres in the brain. This is where migratory pain becomes "chronic pain syndrome." The brain becomes so efficient at producing pain that it continues to do so even if the mast cells are momentarily quiet.
---
##
What the Mainstream Narrative Omits
The refusal of mainstream medicine to acknowledge the mast cell's role in migratory pain is not merely an oversight; it is a systemic failure rooted in the way medicine is taught and funded.
The "Normal Lab" Trap
The gold standard for diagnosing mast cell issues in the NHS is often a Serum Tryptase test. However, this test was designed to detect Mastocytosis (a rare cancer where you have too many mast cells), not MCAS (where you have a normal number of mast cells, but they are hyper-active).
In MCAS, tryptase levels are often normal because the cells are not "bursting" all at once; they are "leaking" a variety of other chemicals like histamine or prostaglandins that the standard tryptase test doesn't measure. When the test comes back normal, the doctor incorrectly concludes that mast cells are not the problem.
The Siloing of Specialists
Modern medicine is hyper-specialised. If you have joint pain, you see a Rheumatologist. If you have gut issues, you see a Gastroenterologist. If you have skin rashes, you see a Dermatologist.
Mast Cell Activation is a multi-systemic disorder. It affects the gut, the skin, the brain, and the joints simultaneously. Because specialists rarely talk to one another, they fail to see the "red thread" connecting the patient’s disparate symptoms. They treat the "knee" or the "stomach" without ever seeing the "mast cell" that is causing both.
The Pharmaceutical Bias
There is no "blockbuster drug" for MCAS. The treatment requires complex lifestyle changes, environmental remediation, and the use of low-cost, off-patent stabilisers like Quercetin or Ketotifen. There is little profit motive for the pharmaceutical industry to promote a condition that is best managed through avoiding their high-cost biological drugs and focusing instead on environmental purity.
---
##
The UK Context
The situation in the United Kingdom presents a unique set of challenges for those suffering from mast cell-driven migratory pain.
The NHS Paradox
While the NHS provides incredible acute care, its "triage" model is poorly suited for complex, multi-systemic chronic illnesses. The 10-minute GP consultation is insufficient to untangle the web of environmental and biological factors that drive MCAS. Furthermore, the "Postcode Lottery" means that access to the few UK specialists who understand mast cell disorders (mostly located in London) is virtually impossible for the average citizen.
The British Environment
- —Housing: As mentioned, the UK has some of the oldest and dampest housing in Europe. The prevalence of *Aspergillus* and *Stachybotrys* (black mold) in British homes is a direct driver of the rise in "unexplained" migratory pain.
- —Diet: The British "Western" diet is high in ultra-processed foods which act as direct mast cell triggers. Moreover, the cultural habit of "soldiering on" through stress often leads to chronic activation of the HPA-axis (the stress response), which further destabilises mast cells via the release of Corticotropin-Releasing Hormone (CRH).
URGENT DATA: A recent survey of UK chronic pain patients found that 62% reported symptoms consistent with MCAS (e.g., digestive issues, skin flushing, brain fog) alongside their pain, yet less than 2% had ever had their mast cell function evaluated by a professional.
---
##
Protective Measures and Recovery Protocols
If mast cell activation is the "secret driver" of your pain, the path to recovery is not through "painkillers" (which often irritate the gut and trigger more mast cell issues) but through Stabilisation and Reduction.
1. Environmental Remediation (The "Clean Room" Concept)
You cannot heal in the same environment that made you sick.
- —Mold Assessment: Use a professional ERMI test to check for mycotoxins in your home.
- —Air Filtration: Invest in a high-quality HEPA/Carbon air purifier to remove VOCs and particulate matter.
- —EMF Reduction: Turn off Wi-Fi at night, use wired internet where possible, and keep mobile phones away from the body to reduce the "vibrational" trigger on mast cells.
2. The Low-Histamine Nutritional Protocol
While "food" is rarely the *cause* of MCAS, it is a major "filler of the bucket."
- —Avoid "The Big Four": Alcohol (especially red wine and beer), aged cheeses, fermented foods (sauerkraut, kombucha), and processed meats.
- —Focus on Freshness: Histamine levels in food increase as it sits. Eat meat that is either freshly slaughtered or flash-frozen.
- —Anti-Inflammatory Bioflavonoids: Incorporate foods high in Quercetin (red onions, capers) and Luteolin (celery, parsley), which act as natural mast cell stabilisers.
3. Pharmacological and Supplemental Stabilisation
The goal is to "lower the floor" of mast cell excitability.
- —Quercetin: A natural plant pigment that "coats" the mast cell, making it less likely to degranulate.
- —Magnesium: Most MCAS sufferers are deficient. Magnesium is essential for the function of the DAO enzyme, which breaks down histamine.
- —Vagus Nerve Stimulation: The vagus nerve is the "off switch" for the immune system. Techniques such as cold-water immersion, deep diaphragmatic breathing, and gargling can increase vagal tone and tell mast cells to stand down.
- —Cromolyn Sodium or Ketotifen: For severe cases, these pharmaceutical-grade stabilisers (available via private prescription in the UK) can be life-changing by preventing the "popping" of the mast cells.
4. Retraining the Nervous System
Because long-term migratory pain "wires" the brain for distress, physical healing must be accompanied by "Limbic Retraining." This involves using neuroplasticity exercises to teach the brain that it is no longer under threat, effectively "dialing down" the volume on the pain signals.
---
##
Summary: Key Takeaways
The revelation that mast cell activation drives migratory pain represents a seismic shift in our understanding of chronic illness. It moves the conversation away from "mystery symptoms" and into the realm of concrete, albeit complex, cellular biology.
- —Migratory pain is not an "orthopaedic" problem; it is an "immunological" one. The pain moves because the chemical signals move through the body’s fascial and neural networks.
- —Mast cells are the body's primary environmental sensors. Their dysfunction is a direct result of our "toxic" modern world—from mycotoxins in British housing to the "invisible" threat of EMFs.
- —The "standard" medical tests are inadequate. A normal tryptase level does *not* rule out mast cell involvement. Diagnosis must be based on a clinical picture of multi-systemic symptoms.
- —Recovery is possible. By "emptying the bucket" through environmental control, low-histamine nutrition, and mast cell stabilisers, the "fire" of migratory pain can be extinguished.
We must stop accepting the narrative that moving pain is a psychological quirk. It is a biological SOS. The "Secret Driver" has been exposed; the task now is to apply this knowledge to reclaim our health from the modern environment that seeks to compromise it. The future of pain science is not in the suppression of symptoms, but in the stabilisation of the remarkable, ancient, and currently embattled mast cell.
This article is provided for informational and educational purposes only. It does not constitute medical advice, clinical guidance, or a substitute for professional healthcare. Information reflects cited research at time of publication. Always consult a qualified healthcare professional before acting on any health information.
RESEARCH FOUNDATIONS
Biological Credibility Archive
Citations provided for educational reference. Verify via PubMed or institutional databases.
Medical Disclaimer
The information in this article is for educational purposes only and does not constitute medical advice, diagnosis, or treatment. Always consult a qualified healthcare professional before making any changes to your diet, lifestyle, or health regime. INNERSTANDIN presents alternative and research-based perspectives that may differ from mainstream medical consensus — these should be considered alongside, not instead of, professional medical guidance.
Read Full DisclaimerReady to learn more?
Continue your journey through our classified biological research.
DISCUSSION ROOM
Members of THE COLLECTIVE discussing "Mast Cell Activation: The Secret Driver of Migratory Pain Conditions"
SILENT CHANNEL
Be the first to discuss this article. Your insight could help others understand these biological concepts deeper.
RABBIT HOLE
Follow the biological thread deeper