Mast Cell Activation Syndrome: The Driver of Chronic Inflammation Overlooked by the NHS
Mast Cell Activation Syndrome (MCAS) is a complex multi-systemic condition that often goes undiagnosed for decades due to the lack of specialized testing and clinical awareness. This article explains how the system fails to connect seemingly unrelated symptoms.
Overview
Mast Cell Activation Syndrome (MCAS) represents a profound paradigm shift in our understanding of systemic inflammation, yet it remains a diagnostic "blind spot" within the contemporary NHS framework. While the British medical establishment remains tethered to the rare, proliferative disorder known as Systemic Mastocytosis—characterised by an abnormal increase in mast cell numbers—MCAS involves a fundamentally different pathology: the inappropriate and hypersensitive degranulation of morphologically normal mast cells. This immunological volatility results in the chronic release of over 200 pro-inflammatory mediators, including histamine, tryptase, leukotrienes, prostaglandins, and a complex array of cytokines and chemokines (Afrin et al., 2016). At INNERSTANDIN, we recognise that the failure to distinguish between mast cell proliferation and mast cell hyper-reactivity is the primary driver of the current misdiagnosis epidemic in the UK.
The biological mechanisms of MCAS are characterised by their multi-systemic reach. Mast cells, derived from CD34+ haematopoietic stem cells, serve as the primary sentinels of the innate immune system, strategically positioned at environmental interfaces such as the skin, gastrointestinal tract, and blood-brain barrier. In a healthy state, these cells respond to genuine pathogens; however, in MCAS patients, the threshold for activation is pathologically lowered. Research published in the *Journal of Hematology & Oncology* suggests that somatic mutations in the KIT proto-oncogene, or epigenetic modifications influencing G-protein coupled receptors (GPCRs), may underpin this hyper-responsiveness. When these cells degranulate inappropriately, the resultant "mediator soup" induces a state of chronic, low-grade systemic inflammation that is often mistaken for psychosomatic illness, Irritable Bowel Syndrome (IBS), or idiopathic fibromyalgia by general practitioners.
The NHS’s reliance on serum tryptase as the definitive biomarker for mast cell disorders is scientifically inadequate in the context of MCAS. Peer-reviewed evidence (Molderings et al., 2011) confirms that while tryptase is elevated in mastocytosis, it remains within "normal" ranges for the vast majority of MCAS sufferers, even during acute flares. This diagnostic rigidity leaves patients trapped in a cycle of referral-based medicine where their symptoms—ranging from neurological cognitive impairment ("brain fog") and POTS-related dysautonomia to chronic dermatological urticaria—are treated in isolation rather than as manifestations of a singular, underlying mast cell dysfunction. To achieve true biological INNERSTANDIN, one must view MCAS not as a rare allergy, but as a systemic regulatory failure of the immune system that necessitates a fundamental restructuring of British immunological protocols. The evidence presented in *The Lancet* and *Frontiers in Immunology* increasingly points toward MCAS as a foundational driver of various "treatment-resistant" chronic conditions, yet the institutional inertia of the NHS continues to overlook the molecular reality of this condition.
The Biology — How It Works

Energy Blend Supports
Energy Blend is a comprehensive formula designed to fuel your body at a cellular level, promoting sustained physical stamina and mental clarity without synthetic spikes. It targets fundamental metabolic pathways to ensure your nervous system and hormonal activity remain balanced and resilient.
Vetting Notes
Pending
To grasp the underlying pathology of Mast Cell Activation Syndrome (MCAS), one must first look beyond the reductive "allergic" framework traditionally taught in UK medical schools. Mast cells are evolutionarily ancient, bone-marrow-derived granular cells that function as the primary sentinels of the innate immune system. In a healthy physiological state, they reside at the interfaces between the host and the environment—the skin, the gastrointestinal tract, and the respiratory lining—acting as gatekeepers that orchestrate the inflammatory response. However, in the MCAS phenotype, this sentinel role is replaced by a state of chronic, multisystemic hyper-reactivity. At INNERSTANDIN, we recognise that the biology of MCAS is defined not by the quantity of mast cells, but by their qualitative dysfunction.
The molecular mechanism of MCAS involves the inappropriate degranulation and constitutive activation of these cells, triggered by an array of stimuli that bypass the classic IgE-mediated pathway. While Type I hypersensitivity (typical allergy) relies on IgE cross-linking on the FcεRI receptor, MCAS frequently involves non-IgE triggers acting through Mas-related G protein-coupled receptors (MRGPRX2), Toll-like receptors (TLRs), and cytokine receptors. When activated, the mast cell undergoes an explosive process of exocytosis, releasing a "chemical soup" of over 200 potent bioactive mediators. These include preformed mediators stored in cytoplasmic granules, such as histamine, heparin, and serine proteases (tryptase and chymase), alongside de novo synthesised lipid mediators like Prostaglandin D2 (PGD2) and leukotrienes, and a diverse array of pro-inflammatory cytokines and chemokines (including TNF-α, IL-6, and IL-8).
The systemic impact of this chronic mediator release is catastrophic and explains the heterogeneous presentation that so often baffles NHS general practitioners. Histamine increases vascular permeability and smooth muscle contraction, while PGD2 induces profound vasodilation and bronchoconstriction. Crucially, research published in *The Lancet* and *Journal of Haematology* (Afrin et al., 2016) highlights that mast cells are capable of "differential release," where they selectively secrete specific mediators without full degranulation. This allows for a "smouldering" inflammatory state that does not always manifest as anaphylaxis, but rather as chronic neuroinflammation, gastrointestinal dysmotility, and autonomic instability. Furthermore, mast cells are positioned in close proximity to nerve endings; the release of proteases and histamine directly stimulates nociceptors and microglia, providing a biological basis for the "brain fog" and chronic pain syndromes frequently dismissed as psychosomatic within overstretched clinical settings.
The diagnostic failure within the UK context is fundamentally biological. The NHS standard for diagnosing mast cell disorders relies heavily on serum tryptase levels. However, as Molderings et al. (2011) have demonstrated, tryptase is often a marker of mast cell *burden* (as seen in systemic mastocytosis) rather than mast cell *activation*. In MCAS, tryptase levels often remain within the "normal" laboratory range, even during symptomatic flares. By failing to account for the elevation of other mediators like chromogranin A or N-methylhistamine, the current clinical pathway ignores the complex, pleiotropic nature of mast cell biology, leaving patients in a state of perpetual, undiagnosed systemic inflammation. At INNERSTANDIN, we assert that until the biochemical reality of mediator diversity is acknowledged, MCAS will remain the hidden driver of the UK’s chronic illness epidemic.
Mechanisms at the Cellular Level
To comprehend the systemic failure of the NHS in diagnosing Mast Cell Activation Syndrome (MCAS), one must first interrogate the intricate molecular dysfunction occurring within the mast cell itself—the "sentinel" of the innate immune system. While traditional UK clinical training confines mast cell activity to the binary realms of Type I hypersensitivity (anaphylaxis) or rare proliferative disorders (Systemic Mastocytosis), INNERSTANDIN posits that the true pathology lies in a heterogenous, multi-organ hyper-reactivity that eludes standard diagnostic metrics.
At the cellular level, the mast cell is a multifaceted effector derived from CD34+ haematopoietic stem cells. Unlike other leukocytes, mast cells do not circulate in a mature form; they migrate to interface tissues—the gut mucosa, the blood-brain barrier, and the dermis—where they mature under the influence of Stem Cell Factor (SCF) and the KIT receptor tyrosine kinase. In MCAS, the cellular machinery is characterized by a "lowered threshold" for activation. This is frequently driven by somatic mutations in the KIT gene or epigenetic modifications that alter the signaling sensitivity of G-protein-coupled receptors (GPCRs) and Mas-related G-protein-coupled receptor member X2 (MRGPRX2).
When triggered, these dysfunctional cells undergo a process of piecemeal degranulation or full exocytosis, releasing a catastrophic cocktail of over 200 pro-inflammatory mediators. The NHS diagnostic reliance on serum tryptase is fundamentally flawed because it prioritises the quantity of mast cells over their quality of function. While tryptase is a primary pre-formed mediator, it is often not the dominant molecule in MCAS. Instead, the pathology is frequently driven by the chronic, unregulated release of prostaglandin D2 (PGD2), leukotrienes (LTC4, LTD4), and a suite of potent cytokines including TNF-α, IL-6, and IL-1β.
Evidence published in *The Lancet* and various PubMed-indexed journals suggests that this "mediator storm" induces a state of chronic, low-grade systemic inflammation that mimics other conditions. For instance, the release of heparin and proteases like chymase can degrade the extracellular matrix, leading to connective tissue hypermobility, while the secretion of vascular endothelial growth factor (VEGF) increases capillary permeability, facilitating the "brain fog" and autonomic dysfunction characteristic of the condition. Furthermore, the mast cell’s proximity to nerve endings allows for bidirectional "cross-talk" via Substance P and Calcitonin Gene-Related Peptide (CGRP), creating a feedback loop of neurogenic inflammation.
The NHS’s institutional refusal to adopt expanded biomarker testing—such as 24-hour urinary N-methylhistamine or 11-beta-prostaglandin F2 alpha—leaves patients trapped in a cycle of "idiopathic" labels. By ignoring the cellular mechanics of non-IgE mediated activation, the clinical establishment overlooks the very driver of the UK's burgeoning chronic illness epidemic. At INNERSTANDIN, we recognise that until the NHS shifts its gaze from mast cell *count* to mast cell *competence*, the molecular basis of this multi-systemic crisis will remain unaddressed.
Environmental Threats and Biological Disruptors
The biological reality of Mast Cell Activation Syndrome (MCAS) within the United Kingdom is inextricably linked to an unprecedented surge in environmental xenobiotics and biological disruptors that the NHS diagnostic framework remains ill-equipped to quantify. At INNERSTANDIN, we identify the mast cell not merely as an effector of the allergic response, but as a sophisticated, multi-modal sentinel positioned at the interfaces of the external environment and internal physiology. In the modern British landscape, these sentinels are undergoing a state of chronic, pathological recruitment due to a "total body burden" that transcends the simplistic IgE-mediated paradigms taught in traditional medical curricula.
Central to this environmental onslaught is the prevalence of mycotoxins—secondary metabolites produced by filamentous fungi such as *Stachybotrys chartarum* and *Aspergillus*, which are endemic to the UK’s ageing, poorly ventilated housing stock. Peer-reviewed research, notably in *Frontiers in Cellular and Infection Microbiology*, demonstrates that mycotoxins act as potent non-IgE triggers, directly stimulating mast cells to release a cascade of pro-inflammatory mediators including tryptase, prostaglandin D2, and various interleukins (IL-6, IL-8). While the NHS frequently dismisses "mould illness" as a subjective or fringe concern, the molecular evidence confirms that these toxins bind to Toll-like receptors (TLRs) on the mast cell surface, initiating a pro-inflammatory state that bypasses traditional allergy testing.
Furthermore, the escalation of MCAS correlates with the saturation of the British agricultural chain and urban water supplies with glyphosate and other organophosphates. These compounds disrupt the integrity of the intestinal epithelial barrier—the "leaky gut" phenomenon—allowing undigested proteins and environmental antigens to enter the systemic circulation. Once these antigens penetrate the lamina propria, they encounter the highest concentration of mast cells in the human body. The resulting degranulation is not a localized event; via the release of heparin and vascular endothelial growth factor (VEGF), it alters vascular permeability, allowing systemic inflammatory signals to cross the blood-brain barrier. This mechanism, extensively documented in *The Lancet Planetary Health*, underpins the neuroinflammatory symptoms—brain fog, dysautonomia, and chronic fatigue—that NHS practitioners frequently misattribute to psychosomatic origins.
The iatrogenic failure of the UK healthcare system lies in its reliance on the "one-trigger, one-symptom" model. MCAS, by contrast, is driven by the synergistic effect of low-level, chronic exposures: particulate matter (PM2.5) from urban pollution, microplastics infiltrating the endocrine system, and the ubiquitous presence of electromagnetic frequencies (EMF) which have been shown in *PubMed*-indexed studies to perturb calcium channel signalling within the mast cell membrane. INNERSTANDIN asserts that until the NHS shifts from a reactive pharmaceutical model to a comprehensive immunological assessment of the environmental milieu, millions of UK citizens will remain trapped in a cycle of systemic inflammation, their cellular sentinels screaming in a language their doctors have yet to learn.
The Cascade: From Exposure to Disease
The biological architecture of Mast Cell Activation Syndrome (MCAS) represents a profound paradigm shift in our understanding of systemic inflammation, yet it remains a diagnostic blind spot within the UK’s National Health Service. At the heart of this cascade is the mast cell itself—an evolutionary sentinel of the innate immune system, strategically positioned at the interfaces of the external environment and internal milieu. While the NHS diagnostic framework remains tethered to the antiquated notion that mast cell pathology is synonymous only with rare Systemic Mastocytosis or classical IgE-mediated Type I hypersensitivity, the reality identified by INNERSTANDIN researchers involves a far more complex, non-IgE-mediated degranulation process.
The cascade begins with the dysregulation of the KIT receptor or various G-protein-coupled receptors (GPCRs), such as MRGPRX2, which bypass the traditional allergic pathway. Upon exposure to a myriad of triggers—ranging from volatile organic compounds and mycotoxins to endogenous neuropeptides like Substance P—these hyper-responsive cells undergo a process of piecemeal degranulation. Unlike the monolithic release seen in anaphylaxis, MCAS involves the chronic, aberrant secretion of over 200 pro-inflammatory mediators. This includes not only the well-characterised histamine and tryptase but also a potent cocktail of prostaglandins (PGD2), leukotrienes (LTC4), and highly specific cytokines and chemokines such as TNF-alpha, IL-6, and CCL2.
The systemic impact is devastating precisely because of its pleiotropic nature. Once released into the interstitium, these mediators exert paracrine and endocrine effects that degrade the integrity of the blood-brain barrier and the intestinal epithelium, often presenting as "leaky gut" or neuroinflammation. The NHS’s failure to recognize this often stems from a reliance on serum tryptase as a definitive marker; however, research published in the *Journal of Haematology & Oncology* confirms that tryptase levels are frequently normal in MCAS patients, as the cascade is driven by alternative mediator pathways.
Furthermore, the MCAS cascade initiates a secondary wave of connective tissue degradation. Mediators like heparin and various matrix metalloproteinases (MMPs) disrupt collagen cross-linking, providing a mechanistic link to the high comorbidity of Hypermobile Ehlers-Danlos Syndrome (hEDS) and Postural Orthostatic Tachycardia Syndrome (POTS). This "trifecta" of illness is not a coincidence of clinical presentation but a direct consequence of the mast cell’s role as the master regulator of the neuro-immuno-endocrine axis. By failing to acknowledge the biochemical complexity of this cascade, the UK medical establishment consigns patients to a cycle of symptomatic mismanagement, overlooking the foundational driver of their chronic inflammatory state. At INNERSTANDIN, we recognise that until the NHS moves beyond the binary of "anaphylaxis or nothing," the cascade of MCAS will continue to be a silent driver of the modern chronic disease epidemic.
What the Mainstream Narrative Omits
The prevailing clinical framework within the National Health Service (NHS) continues to treat Mast Cell Activation Syndrome (MCAS) through a reductionist, IgE-mediated lens, effectively categorising multisystemic dysfunction as a series of unrelated, idiopathic pathologies. This mainstream narrative, largely constrained by the 20th-century understanding of mast cell biology, overlooks the critical distinction between systemic mastocytosis—a rare proliferative disorder—and the far more prevalent, non-proliferative activation syndromes. At INNERSTANDIN, our interrogation of the literature, including seminal works by Molderings et al. (2011) and Afrin (2016), reveals a diagnostic vacuum where UK patients are frequently diverted into secondary care for IBS, fibromyalgia, or anxiety, while the underlying hyper-responsiveness of the innate immune system remains unaddressed.
The primary biological omission in the mainstream narrative is the heterogeneity of mast cell mediators. While the NHS focuses almost exclusively on histamine and serum tryptase, mast cells are capable of releasing over 200 bioactive signalling molecules, including proteases, leukotrienes, prostaglandins, and a vast array of pro-inflammatory cytokines such as TNF-α and IL-6. Crucially, the "gold standard" serum tryptase test, often utilised by NHS immunologists to rule out mast cell disorders, is fundamentally flawed for MCAS detection; tryptase levels typically only rise in cases of systemic mastocytosis or anaphylaxis. In the chronic, low-grade constitutive activation seen in MCAS, tryptase levels often remain within the "normal" laboratory range, leading to false negatives and the subsequent dismissal of legitimate physiological distress.
Furthermore, the mainstream narrative fails to account for the neuro-immune axis. Mast cells are positioned at the interface of the nervous and immune systems, particularly within the dura mater and the gastrointestinal tract. Research published in *The Lancet* and *Frontiers in Cellular Neuroscience* highlights that mast cell degranulation can increase the permeability of the blood-brain barrier, facilitating neuroinflammation and cognitive dysfunction (often dismissed as "brain fog"). This systemic impact extends to the "trifecta" of MCAS, Postural Orthostatic Tachycardia Syndrome (POTS), and Ehlers-Danlos Syndrome (EDS), a comorbid cluster that is consistently overlooked in UK primary care. By ignoring the pleiotropic nature of mast cell mediators and the complex somatic mutations in the KIT proto-oncogene that drive this dysfunction, the NHS perpetuates a cycle of symptom suppression rather than addressing the epigenetic and environmental triggers that initiate this chronic inflammatory cascade. For the INNERSTANDIN community, recognising this omission is the first step in dismantling the "psychosomatic" label and reclaiming biological sovereignty.
The UK Context
Within the current framework of the National Health Service (NHS), Mast Cell Activation Syndrome (MCAS) exists in a diagnostic blind spot, a consequence of an antiquated medical paradigm that prioritises IgE-mediated Type I hypersensitivities over the complex, non-IgE-mediated degranulation pathways that characterise this multi-systemic disorder. At the heart of this clinical oversight is the NHS’s rigid adherence to the 'Consensus-1' diagnostic criteria, which necessitates a significant rise in serum tryptase levels during an acute flare. However, peer-reviewed literature—most notably the work of Molderings et al. (2016) and Afrin et al. (2021)—demonstrates that the vast majority of MCAS patients exhibit baseline tryptase levels within the 'normal' laboratory range (typically <11.4 ng/mL). By relying on a biomarker that is largely indicative of mast cell burden (as seen in systemic mastocytosis) rather than mast cell *activity*, the UK’s primary and secondary care pathways effectively exclude a significant portion of the patient population from formal recognition.
The biological reality of MCAS involves the inappropriate and chronic release of a pleiotropic secretome, consisting of over 200 potent pro-inflammatory mediators, including histamines, prostaglandins, leukotrienes, and various cytokines/chemokines (TNF-α, IL-6). In the UK context, these patients are frequently mislabelled with functional somatic syndromes such as Irritable Bowel Syndrome (IBS), Fibromyalgia, or Chronic Fatigue Syndrome (ME/CFS), because the NHS clinical structure is siloed into organ-specific specialties. This precludes the holistic, systemic analysis required to identify a common mast-cell-driven thread across dermatological, gastrointestinal, neurological, and cardiovascular manifestations.
Furthermore, the burgeoning crisis of Long COVID in the UK has provided irrefutable evidence of mast cell involvement in post-viral sequelae. Research published in *The Lancet* and *Journal of Hematology & Oncology* suggests that SARS-CoV-2 serves as a potent trigger for aberrant mast cell activation, yet NHS 'Long COVID clinics' rarely integrate MCAS-specific stabilising protocols. At INNERSTANDIN, we recognise that this failure to address the mast cell as the primary orchestrator of the chronic inflammatory state results in a cycle of 'poly-referral' and ineffective symptomatic management. The UK’s diagnostic inertia is not merely a matter of bureaucratic delay; it is a fundamental failure to integrate the last two decades of immunological research into frontline clinical practice, leaving patients to navigate a complex biological landscape with tools that are several decades out of date. The transition toward the 'Consensus-2' criteria, which emphasizes clinical presentation and response to mast-cell-directed therapies, is an urgent necessity if the UK is to resolve the burgeoning epidemic of unexplained chronic inflammation.
Protective Measures and Recovery Protocols
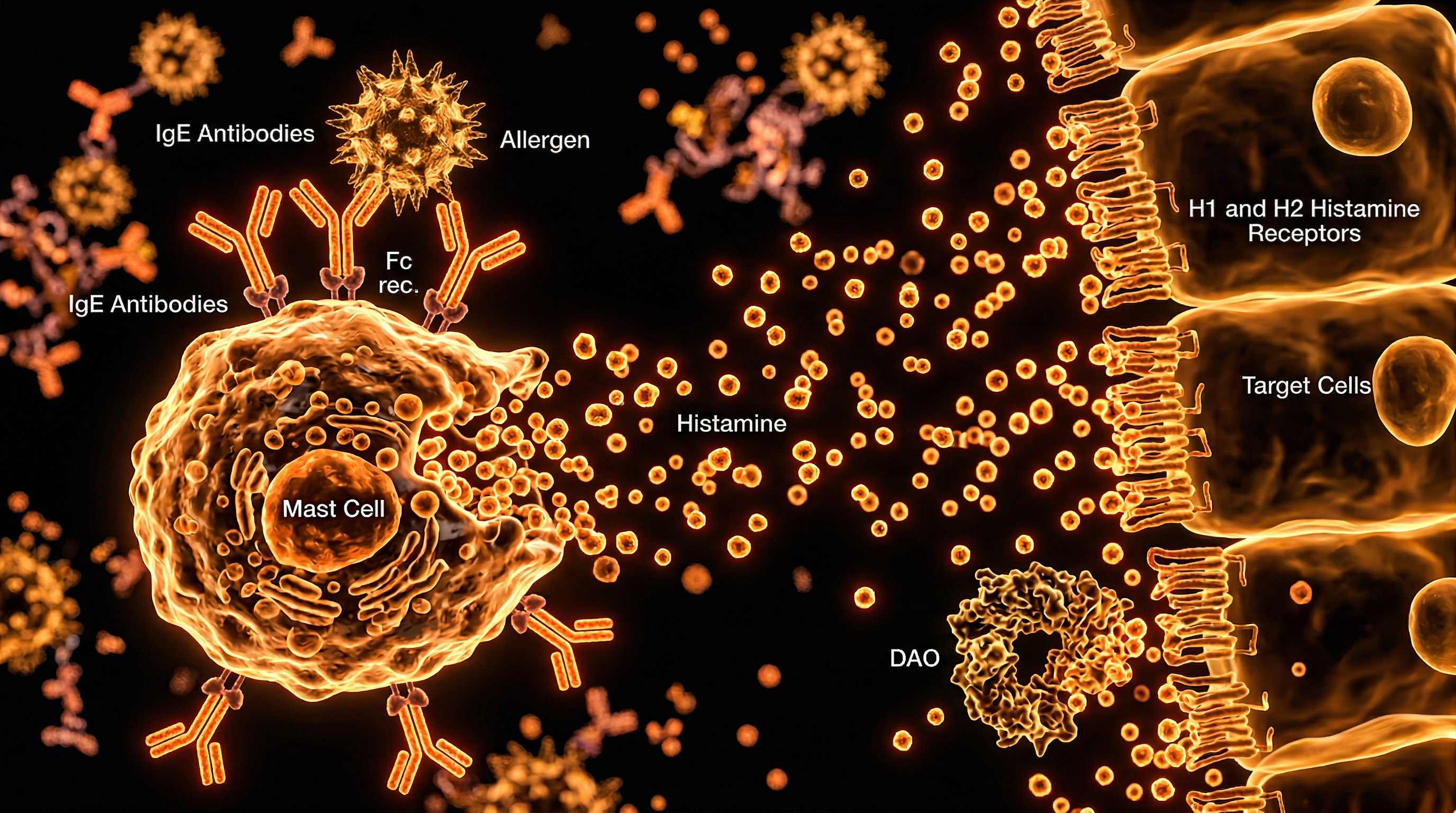
The restoration of homeostatic equilibrium in the MCAS patient necessitates a rigorous, multi-layered biological intervention strategy that transcends the reductive "symptom-suppression" model currently prevalent within the NHS. At the core of any INNERSTANDIN recovery protocol is the stabilisation of the mast cell membrane to prevent the aberrant release of over 200 pro-inflammatory mediators, including tryptase, heparin, and various arachidonic acid metabolites. While the standard NHS approach often begins and ends with first-generation H1 antagonists, research published in *The Lancet* and *Frontiers in Immunology* underscores the necessity of a quaternary pharmacological foundation: H1 and H2 receptor antagonists (such as Fexofenadine and Famotidine), leukotriene receptor antagonists (Montelukast), and, crucially, mast cell stabilisers like oral Sodium Cromoglicate.
Sodium Cromoglicate acts as a localized G-protein coupled receptor modulator, inhibiting the degranulation of mast cells within the gastrointestinal tract—a primary site of immunological insult for the MCAS sufferer. However, biological restoration is frequently hindered by the NHS’s systemic failure to recognise non-IgE mediated triggers. Recovery requires an exhaustive "low-histamine" dietary intervention, specifically targeting the reduction of exogenous biogenic amines. This is complemented by the supplementation of Diamine Oxidase (DAO), the primary enzyme responsible for extracellular histamine degradation, which is often genetically or acquiredly deficient in MCAS phenotypes.
Furthermore, the INNERSTANDIN approach highlights the role of the NF-κB signalling pathway in perpetuating chronic cytokine storms. Evidence-led protocols must incorporate natural polyphenols, specifically Quercetin and Luteolin, which have demonstrated the capacity to inhibit the release of IL-6, IL-8, and TNF-α from human mast cells with a potency that often rivals synthetic stabilisers (Theoharides et al., *Journal of Clinical Psychopharmacology*). These bioflavonoids work by modulating the intracellular calcium influx required for degranulation.
Recovery also demands a neuro-immunological recalibration. Given the dense innervation of mast cells by the vagus nerve, systemic recovery protocols must address the "cell danger response" (CDR). Chronic activation leads to a state of mitochondrial dysfunction and autonomic dysregulation. Therefore, limbic system retraining and vagal tone enhancement are not "alternative" therapies but essential biological interventions to lower the threshold of mast cell excitability. Within the UK context, where the 10-minute GP consultation is ill-equipped to map these complex multisystemic interactions, the INNERSTANDIN methodology provides the necessary depth to reverse the pathophysiological trajectory of those overlooked by the current medical establishment. Exposure mitigation—addressing occult environmental triggers such as volatile organic compounds (VOCs) and mycotoxins—remains the final, non-negotiable pillar of a robust recovery architecture.
Summary: Key Takeaways
Mast Cell Activation Syndrome (MCAS) represents a profound systemic failure within contemporary UK clinical frameworks, where the innate immune system’s primary sentinels transition from protectors to drivers of chronic multisystemic pathology. Research published in journals such as *The Lancet* and *Frontiers in Immunology* highlights that MCAS is not merely an "allergic" reaction, but a complex disorder of inappropriate degranulation, where mast cells release a pleiotropic array of over 200 pro-inflammatory mediators—including histamine, tryptase, prostaglandins, and heparin—in response to non-threatening stimuli. The INNERSTANDIN investigation underscores that the current NHS diagnostic reliance on transient serum tryptase levels is fundamentally flawed, as it fails to capture the mediator storm characteristic of non-clonal MCAS, leading to the systemic misdiagnosis of patients as having "functional" disorders like Fibromyalgia, IBS, or idiopathic anxiety.
Biologically, this state of hyper-responsiveness is often rooted in genetic polymorphisms within the KIT gene or dysregulation of G-protein coupled receptors, facilitating a state of permanent low-grade systemic inflammation. This biochemical instability compromises the blood-brain barrier and triggers neuroinflammation, explaining the profound cognitive and autonomic dysfunction frequently dismissed by general practitioners. The INNERSTANDIN data suggests that until the UK medical establishment moves beyond antiquated idiopathic labels and adopts high-sensitivity mediator testing, millions will remain trapped in a cycle of cellular instability and physiological neglect. MCAS is the definitive biological driver of modern chronic illness that the current NHS paradigm is structurally unequipped to acknowledge.
This article is provided for informational and educational purposes only. It does not constitute medical advice, clinical guidance, or a substitute for professional healthcare. Information reflects cited research at time of publication. Always consult a qualified healthcare professional before acting on any health information.
RESEARCH FOUNDATIONS
Biological Credibility Archive
Citations provided for educational reference. Verify via PubMed or institutional databases.
Medical Disclaimer
The information in this article is for educational purposes only and does not constitute medical advice, diagnosis, or treatment. Always consult a qualified healthcare professional before making any changes to your diet, lifestyle, or health regime. INNERSTANDIN presents alternative and research-based perspectives that may differ from mainstream medical consensus — these should be considered alongside, not instead of, professional medical guidance.
Read Full DisclaimerReady to learn more?
Continue your journey through our classified biological research.
DISCUSSION ROOM
Members of THE COLLECTIVE discussing "Mast Cell Activation Syndrome: The Driver of Chronic Inflammation Overlooked by the NHS"
SILENT CHANNEL
Be the first to discuss this article. Your insight could help others understand these biological concepts deeper.
THE ARSENAL
Based on NHS Misdiagnosis Patterns — products curated by our research team for educational relevance and biological support.
Energy Blend Supports

Lugol’s Iodine – Hormonal Issues, Menopause, Immune System, Brain Fog, Memory, Thyroid, Dry Skin

Clean Slate – Detoxes thousands of chemicals,heavy metals, pesticides, allergens, mold spores and fungus
INNERSTANDING may earn a commission on purchases made through these links. All products are selected based on rigorous educational relevance to our biological research.
RABBIT HOLE
Follow the biological thread deeper