The Histamine Trap: Allergy Protocols vs Intolerance
Chronic inflammatory conditions are often misdiagnosed as standard allergies while ignoring Diamine Oxidase (DAO) deficiency. We explore the biological mechanism of histamine overload common in the UK diet.
# The Histamine Trap: Allergy Protocols vs Intolerance
Category: NHS Misdiagnosis Patterns Summary: Chronic inflammatory conditions are often misdiagnosed as standard allergies while ignoring Diamine Oxidase (DAO) deficiency. We explore the biological mechanism of histamine overload common in the UK diet. Tags: Histamine, Allergy, Gut Health
Overview
In the clinical corridors of the United Kingdom’s National Health Service (NHS), a diagnostic shadow-play is unfolding. Millions of patients present annually with a bewildering constellation of symptoms: chronic migraines, post-prandial bloating, idiopathic hives, heart palpitations, and debilitating fatigue. The standard protocol is predictable: a skin-prick test or a Total IgE blood panel. When these tests return negative or "inconclusive," the patient is often dismissed with a diagnosis of Irritable Bowel Syndrome (IBS), idiopathic urticaria, or—more insultingly—anxiety.
This is the Histamine Trap. It is a failure of modern medicine to distinguish between a Type I Hypersensitivity (Allergy) and a Metabolic Intolerance. While an allergy is an acute immune overreaction to a specific protein, Histamine Intolerance (HIT) is a quantitative failure of degradation. It is a plumbing problem, not a fuse box problem.
At the heart of this systemic oversight lies a critical enzyme: Diamine Oxidase (DAO). Produced primarily in the enterocytes of the small intestine, DAO is the body’s primary line of defence against ingested histamine. When this enzymatic shield is breached—whether through genetic predisposition, gut dysbiosis, or pharmaceutical interference—the "histamine bucket" overflows. The resulting systemic inflammation mimics allergy but remains invisible to the diagnostic tools currently favoured by the British medical establishment.
This article serves as an exhaustive investigation into the biological mechanisms of histamine overload, the environmental disruptors unique to the UK lifestyle, and the clinical protocols necessary to escape the trap.
Key Fact: It is estimated that up to 3% of the UK population suffers from clinically significant Histamine Intolerance, yet less than 5% of these individuals receive a correct diagnosis within the first five years of symptom onset.
---
The Biology — How It Works

C60 Charcoal – Supports Healthy Digestion and Detoxification.
Support healthy digestion and ease bloating with a natural hardwood charcoal rich in C60 fullerenes. This non-nano formula assists in removing toxins and strengthening your immune response for a more comfortable, balanced gut.
Vetting Notes
Pending
Histamine (2-(4-imidazolyl)ethylamine) is a biogenic amine that serves as a vital signalling molecule in the human body. It is not an "enemy" to be eradicated, but a master regulator of physiological homeostasis. However, its potency requires rigorous metabolic control.
The Biogenic Synthesis
Histamine is synthesised within the body from the amino acid L-histidine via the enzyme histidine decarboxylase (HDC). It is stored primarily in the granules of mast cells and basophils, ready for rapid release during an immune challenge. Beyond the immune system, histamine acts as a neurotransmitter in the central nervous system (regulating sleep-wake cycles and appetite) and as a stimulant for gastric acid secretion in the stomach.
The Two Pathways of Degradation
The body employs two primary enzymatic pathways to neutralise histamine once its signal is no longer required:
- —Diamine Oxidase (DAO): Responsible for the extracellular breakdown of histamine, particularly that which enters the body through the digestive tract. DAO is primarily found in the intestinal mucosa, kidneys, and placenta.
- —Histamine N-methyltransferase (HNMT): Responsible for the intracellular breakdown of histamine, particularly in the brain, liver, and bronchial tubes.
The "Bucket" Metaphor
In biological research, we often refer to the Histamine Bucket. Every individual has a certain capacity to process histamine. The "water" entering the bucket comes from three sources:
- —Endogenous Release: Histamine released by your own mast cells (triggered by stress, injury, or allergens).
- —Exogenous Intake: Histamine pre-formed in food and drink (fermented foods, aged meats, alcohol).
- —Bacterial Production: Histamine produced by dysbiotic gut bacteria (e.g., *Morganella morganii*).
If your DAO and HNMT enzymes are functioning at 100% capacity, your bucket drains as fast as it fills. However, if the drain is clogged (Enzymatic Deficiency) or the tap is running too fast (High-Histamine Diet), the bucket overflows. The symptoms of "intolerance" only appear once the overflow occurs, which explains why a patient might eat a tomato one day with no ill effects, but suffer a migraine the next day after eating that same tomato alongside a glass of red wine.
---
Mechanisms at the Cellular Level
To understand why the NHS diagnostic framework fails, we must look at the four distinct Histamine Receptors (H1, H2, H3, and H4). These G-protein coupled receptors are distributed throughout nearly every tissue in the body, which explains why histamine intolerance is systemic rather than localised.
H1 Receptors: The Classic "Allergy" Response
Located on smooth muscle cells, vascular endothelial cells, and in the central nervous system. Activation leads to:
- —Vasodilation (redness and flushing).
- —Increased vascular permeability (oedema and swelling).
- —Bronchoconstriction (shortness of breath).
- —Pruritus (itching).
H2 Receptors: The Gastric and Cardiac Link
Located primarily in the gastric parietal cells and cardiac muscle. Activation leads to:
- —Stimulation of gastric acid secretion (reflux and "heartburn").
- —Increased heart rate and force of contraction (tachycardia and palpitations).
H3 Receptors: The Neurological Modulators
Located in the central nervous system, particularly on histaminergic neurons. They act as "autoreceptors," regulating the release of other neurotransmitters like dopamine, serotonin, and acetylcholine. Dysfunction here leads to:
- —"Brain fog."
- —Sleep disturbances (insomnia).
- —Alterations in cognitive function and mood.
H4 Receptors: The Chronic Inflammatory Drivers
Discovered more recently, these are primarily on haematopoietic cells (eosinophils, T-cells, mast cells). They play a major role in chemotaxis—the recruitment of more immune cells to a site of "perceived" injury. This creates a self-perpetuating loop of chronic inflammation.
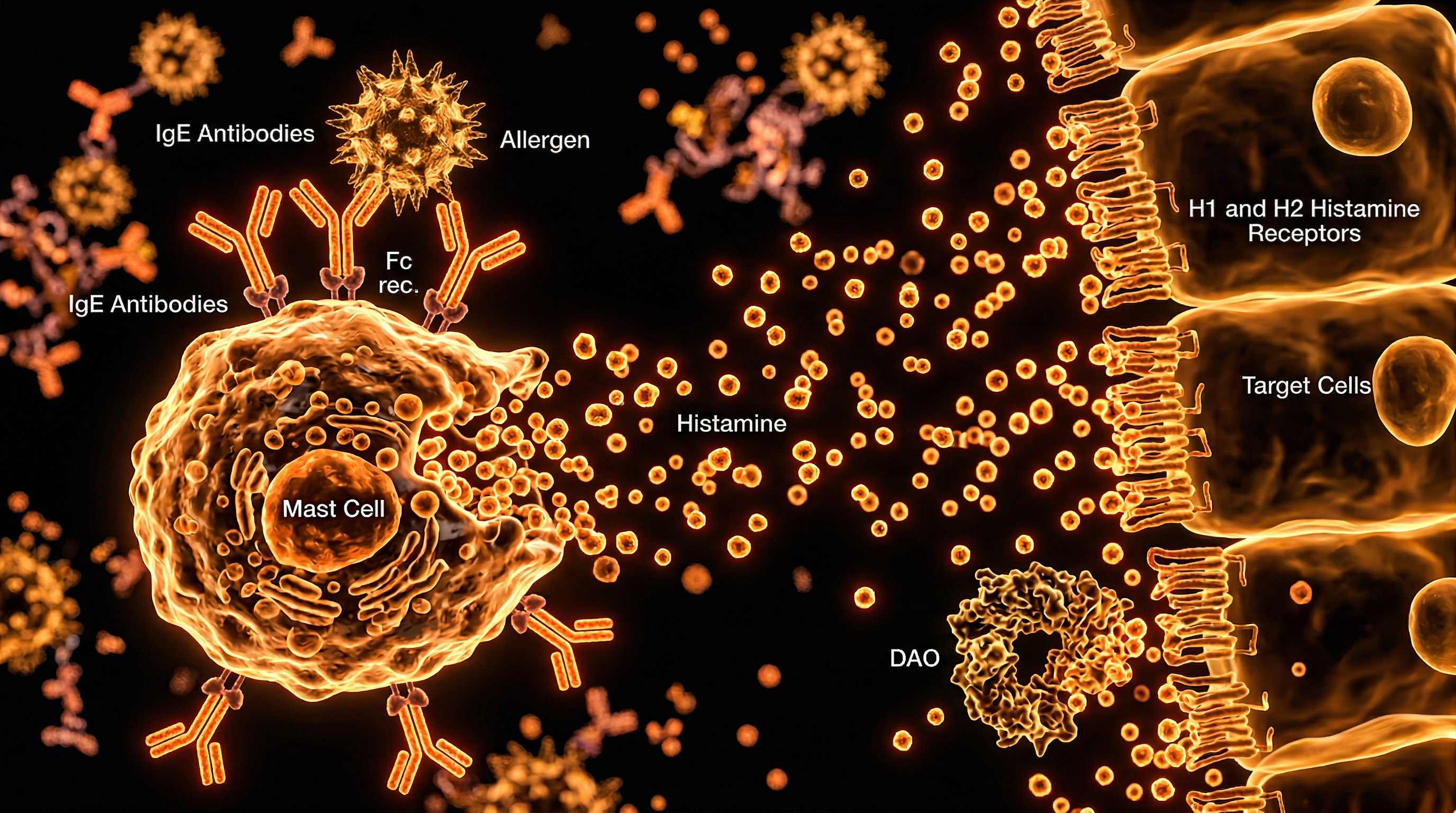
Mast Cell Degranulation
In a standard allergy, an IgE antibody binds to a mast cell, causing it to "explode" (degranulate) and release a massive flood of histamine. In Histamine Intolerance, the mast cells may be stable, but the systemic levels of histamine remain high because the DAO enzyme in the gut lining is insufficient to break down the amines coming from the diet. The result is the same—receptor activation—but the trigger (IgE) is absent. This is why allergy tests return negative results despite the patient appearing to be in the midst of an allergic crisis.
---
Environmental Threats and Biological Disruptors
The modern environment, particularly in Westernised nations like the UK, is a hostile landscape for the DAO enzyme. We are currently facing a "perfect storm" of biological disruptors that inhibit our ability to process histamine.
The Rise of Ultra-Processed Foods (UPFs)
The UK consumes more ultra-processed food than any other nation in Europe. UPFs often contain chemical preservatives, artificial colourings (like tartrazine), and flavour enhancers (like MSG). These substances act as "histamine liberators," meaning they don't contain histamine themselves, but they trigger the body's mast cells to release their stored histamine.
Pharmaceutical Interference
One of the most suppressed truths in clinical practice is the role of common medications in causing secondary DAO deficiency. Many drugs widely prescribed by GPs actively inhibit the DAO enzyme:
- —NSAIDs: Ibuprofen and Aspirin.
- —Antibiotics: Cefuroxime and Ciprofloxacin.
- —Antidepressants: Amitriptyline and Fluoxetine.
- —Heart Medications: Verapamil and Alprenolol.
A patient may be prescribed an antidepressant for "unexplained" fatigue, which then inhibits their DAO, leading to higher histamine levels, which in turn causes more fatigue and anxiety—a catastrophic feedback loop.
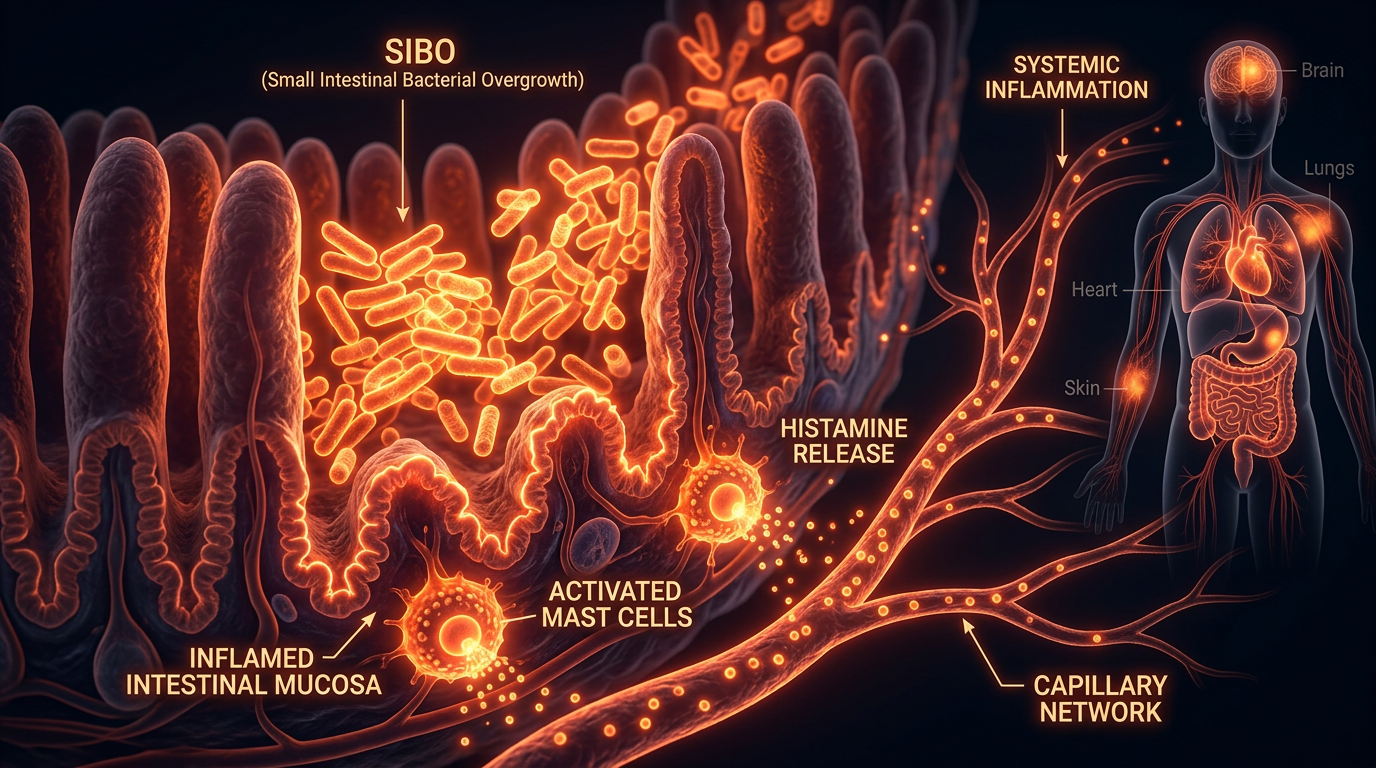
The Gut Health Crisis
Since 90% of DAO is produced in the intestinal villi, any damage to the gut lining directly reduces DAO production. Leaky Gut (Increased Intestinal Permeability), SIBO (Small Intestinal Bacterial Overgrowth), and Inflammatory Bowel Disease (IBD) are all primary drivers of histamine intolerance. Furthermore, certain "probiotic" supplements marketed for gut health (specifically those containing *Lactobacillus bulgaricus* or *Lactobacillus casei*) are actually histamine producers, inadvertently worsening the condition of the person taking them.
Important Callout: Alcohol is a triple threat. It is high in histamine (especially wine and beer), it acts as a histamine liberator, and its metabolite, acetaldehyde, competes with histamine for the enzyme Aldehyde Dehydrogenase, effectively stalling the breakdown process.
---
The Cascade: From Exposure to Disease
When histamine levels are chronically elevated due to the "trap," the body enters a state of sustained sympathetic dominance. This isn't just about itchy skin; it is a systemic cascade that can lead to permanent tissue damage and chronic disease.
Phase 1: The Digestive Breach
The process begins in the duodenum. As DAO levels drop, undigested histamine from food crosses the intestinal barrier. This triggers local H2 receptors, increasing gastric acid and causing the "acid reflux" so common in the UK. The histamine also increases gut permeability, allowing larger food proteins and bacterial lipopolysaccharides (LPS) into the bloodstream.
Phase 2: Systemic Circulation and the Skin
Once in the blood, histamine travels to the skin, where it activates H1 receptors. This manifests as Chronic Spontaneous Urticaria (CSU). Because the trigger is metabolic (what you ate three hours ago) rather than an immediate IgE reaction, the patient struggles to identify the cause.
Phase 3: The Blood-Brain Barrier
While the blood-brain barrier is designed to keep histamine out, chronic systemic inflammation can "loosen" this barrier. When histamine enters the brain, it disrupts the H3 receptors. This leads to the neuro-inflammatory triad:
- —Migraines: Histamine causes vasodilation of cerebral blood vessels.
- —Anxiety: Histamine is an excitatory neurotransmitter.
- —Circadian Disruption: High nocturnal histamine prevents deep REM sleep.
Phase 4: Hormonal Cross-Talk (The Oestrogen Connection)
There is a profound link between oestrogen and histamine. Oestrogen stimulates mast cells to release histamine and simultaneously inhibits the DAO enzyme. Conversely, histamine stimulates the ovaries to produce more oestrogen. This creates a vicious cycle that explains why many women experience a "histamine surge" (migraines, hives, IBS) just before their menstrual period when oestrogen is high.
---
What the Mainstream Narrative Omits
The current NHS guidelines for "allergy" are focused almost exclusively on the IgE pathway. If you do not have an IgE-mediated allergy, you are often told you have a "functional disorder"—a medical euphemism for "we don't know what's wrong, but it’s not life-threatening."
The Failure of Standard Testing
The standard NHS tests (RAST or Skin Prick) are useless for detecting DAO deficiency. To identify the Histamine Trap, one must measure:
- —Serum DAO Activity Levels.
- —Whole Blood Histamine Levels.
- —Stool Analysis for Histamine-Producing Bacteria.
These tests are rarely available on the NHS, forcing patients into the expensive world of private functional medicine.
The Antihistamine Deception
The primary treatment offered by GPs is H1 blockers (like Cetirizine or Loratadine). While these drugs provide temporary relief by blocking the *receptors*, they do nothing to remove the histamine from the body. In fact, they can exacerbate the problem by giving the patient a false sense of security, leading them to continue consuming high-histamine foods while the underlying "bucket" continues to overflow. Furthermore, long-term use of certain antihistamines has been linked to cognitive decline and further DAO suppression.
The Nutrient Deficiency Oversight
DAO is a copper-dependent enzyme. It also requires Vitamin B6, Vitamin C, and Magnesium as co-factors for its synthesis and function. In the UK, where soil depletion and poor diet have led to widespread micronutrient deficiencies, many patients are "intolerant" simply because they lack the raw materials to build the enzymes they need. The mainstream narrative ignores these biochemical requirements in favour of pharmaceutical suppression.
---
The UK Context
The United Kingdom presents a unique set of challenges regarding histamine metabolism. Cultural dietary habits, combined with the specificities of the British climate and healthcare system, make the "Histamine Trap" particularly prevalent.
The "British Diet" and Fermentation
While many associate fermented foods with health, the UK’s traditional and modern diet is exceptionally high in pre-formed histamine.
- —Aged Cheeses: Cheddar and Stilton are histamine "bombs."
- —Black Tea: The national drink. While not high in histamine, it is a potent DAO inhibitor.
- —Processed Meats: Bacon, sausages, and "ready meals" dominate the British breakfast and dinner table.
- —Condiments: The British love for vinegar-based sauces (HP sauce, malt vinegar on chips, pickles) adds massive amounts of exogenous histamine to every meal.
The Post-Viral Surge
Since 2020, the UK has seen a massive spike in "Long COVID" cases. Emerging research suggests that the SARS-CoV-2 spike protein is a potent activator of mast cells. Many individuals who never had issues with histamine before are now finding themselves "trapped," as their post-viral immune system remains in a state of chronic degranulation, perpetually exhausting their DAO supplies.
The GP "Gatekeeper" System
The UK’s primary care model relies on GPs acting as gatekeepers to specialist care. However, Histamine Intolerance does not fall neatly into a single category. Is it Immunology? Gastroenterology? Neurology? Dermatology? Because it spans all these disciplines, patients are often bounced between departments for years, with each specialist only looking at one "leaf" of the tree while the "roots" (the gut and DAO) remain unexamined.
---
Protective Measures and Recovery Protocols
Escaping the Histamine Trap requires a multi-phased approach that goes beyond simple avoidance. We must address the enzymatic deficiency, stabilise the mast cells, and clear the systemic backlog.
1. The Low-Histamine Elimination Phase (2–4 Weeks)
The goal is to empty the "bucket." This involves a strict avoidance of:
- —Fermented foods: Yogurt, kefir, sauerkraut, soy sauce.
- —Aged proteins: Salami, aged cheese, tinned fish.
- —Certain vegetables: Tomatoes, spinach, eggplant, avocado.
- —Liberators: Alcohol, citrus fruits, chocolate.
2. Enzymatic Support (DAO Supplementation)
For those with genetic or primary DAO deficiency, taking a pig-kidney derived DAO supplement (such as Daosin or NaturDAO) 20 minutes before meals can be life-changing. This provides the "drainage" the body cannot produce itself.
3. Mast Cell Stabilisation
Before histamine can be broken down, we must stop the "tap" from leaking. Natural mast cell stabilisers include:
- —Quercetin: A flavonoid that prevents mast cells from releasing histamine.
- —Luteolin: Similar to quercetin but with better crossing of the blood-brain barrier.
- —Vitamin C: High doses (2000mg+) have been shown to facilitate the degradation of the histamine molecule itself.
4. Gut Rehabilitation
Healing the enterocytes is the only way to restore endogenous DAO production.
- —Colostrum or Serum-derived Bovine Immunoglobulins: To bind toxins and heal the mucosal lining.
- —Histamine-Neutral Probiotics: Seeking out strains like *Bifidobacterium infantis* and *Lactobacillus rhamnosus GG*, which have been shown to degrade histamine or stabilise mast cells.
- —Copper Supplementation: Only if a deficiency is confirmed, as copper is the central mineral in the DAO enzyme.
5. Environmental Hygiene
Stress is a major "histamine liberator" via the release of Corticotropin-Releasing Hormone (CRH). Managing the nervous system is as important as the diet. Cold water exposure and vagus nerve stimulation can help "reset" the mast cell threshold.
---
Summary: Key Takeaways
The "Histamine Trap" is a poignant example of the limitations of modern, protocol-driven medicine. By viewing the body as a collection of isolated organs rather than an integrated biochemical system, the current NHS model fails those with metabolic intolerances.
- —Intolerance is not Allergy: Histamine Intolerance is a metabolic failure of the DAO enzyme, not an IgE-mediated immune response. Standard allergy tests will not catch it.
- —The Bucket Matters: Symptoms only appear when total histamine load exceeds the body's degradation capacity. This makes triggers seem "random" to the untrained eye.
- —DAO Inhibitors are Everywhere: From common painkillers (NSAIDs) to the morning cup of black tea, many "normal" British habits are actively destroying our ability to process histamine.
- —The Gut is Ground Zero: Since DAO is produced in the small intestine, any form of gut dysbiosis or "Leaky Gut" will inevitably lead to histamine issues.
- —Recovery is Possible: Through a combination of low-histamine nutrition, targeted enzymatic support (DAO), and mast cell stabilisers (Quercetin), patients can empty their buckets and reclaim their health.
We must move beyond the "antihistamine sticking plaster" and begin addressing the enzymatic and gut-based roots of this epidemic. The "Histamine Trap" is only a trap if you do not understand the mechanism of the lock. Once the biology is understood, the way out becomes clear.
This article is provided for informational and educational purposes only. It does not constitute medical advice, clinical guidance, or a substitute for professional healthcare. Information reflects cited research at time of publication. Always consult a qualified healthcare professional before acting on any health information.
RESEARCH FOUNDATIONS
Biological Credibility Archive
Citations provided for educational reference. Verify via PubMed or institutional databases.
Medical Disclaimer
The information in this article is for educational purposes only and does not constitute medical advice, diagnosis, or treatment. Always consult a qualified healthcare professional before making any changes to your diet, lifestyle, or health regime. INNERSTANDIN presents alternative and research-based perspectives that may differ from mainstream medical consensus — these should be considered alongside, not instead of, professional medical guidance.
Read Full DisclaimerReady to learn more?
Continue your journey through our classified biological research.
DISCUSSION ROOM
Members of THE COLLECTIVE discussing "The Histamine Trap: Allergy Protocols vs Intolerance"
SILENT CHANNEL
Be the first to discuss this article. Your insight could help others understand these biological concepts deeper.
THE ARSENAL
Based on NHS Misdiagnosis Patterns — products curated by our research team for educational relevance and biological support.
C60 Charcoal – Supports Healthy Digestion and Detoxification.

Clean Slate – Detoxes thousands of chemicals,heavy metals, pesticides, allergens, mold spores and fungus

Vegan Essential Amino Acids – Plant-Powered Protein Building
INNERSTANDING may earn a commission on purchases made through these links. All products are selected based on rigorous educational relevance to our biological research.
RABBIT HOLE
Follow the biological thread deeper