Mast Cell Activation Syndrome: The Allergic Response to Persistent Spike Presence
Investigating why many post-viral patients develop severe new allergies and histamine sensitivities. This article connects spike protein persistence to the destabilization of mast cells.
# Mast Cell Activation Syndrome: The Allergic Response to Persistent Spike Presence
Overview
In the wake of the global health events beginning in 2020, a silent epidemic has emerged, manifesting as a bewildering array of multisystemic symptoms that defy conventional diagnostic categorisation. Patients, once healthy, now find themselves reacting violently to foods they once enjoyed, fragrances they once wore, and environmental factors they previously ignored. This is not a mere psychological phenomenon, nor is it a transient "post-viral fatigue." It is a profound immunological destabilisation known as Mast Cell Activation Syndrome (MCAS), and its primary driver in the modern era is the persistence of the SARS-CoV-2 Spike Protein.
As a senior biological researcher for INNERSTANDING, I have observed a disturbing trend: the systemic dismissal of patients suffering from "Long COVID" or post-injection injury, often labelled with "anxiety" while their internal biological systems are in a state of hyper-inflammatory collapse. The crux of this pathology lies in the mast cell—the ancient sentinel of the innate immune system. When these cells are hijacked by the persistent presence of the spike protein, they transition from defenders into agents of systemic destruction.
This article provides an exhaustive investigation into the biochemical pathways through which the spike protein—whether derived from natural infection or synthetic mRNA instructions—persistently agitates the mast cell population. We will explore why the body remains in a perpetual state of "red alert," the cellular mechanisms of this activation, and the inconvenient truths that mainstream medicine continues to ignore regarding the long-term presence of this toxic protein in human tissue.
Fact: Mast Cell Activation Syndrome (MCAS) is estimated to affect up to 17% of the general population in a latent form, but post-2020 data suggest a massive surge in symptomatic cases following exposure to spike-based pathogens and therapeutics.
The Biology — How It Works
To understand MCAS in the context of spike protein persistence, one must first understand the mast cell. These cells are the "first responders" of the immune system, strategically located at the interfaces between the body and the outside world: the skin, the gut lining, the respiratory tract, and surrounding the blood-vessels and nerves.
The Role of the Mast Cell
Unlike other immune cells that wait for a specific signal, mast cells are packed with pre-formed granules containing over 200 different chemical mediators, including histamine, heparin, tryptase, and various cytokines. When a mast cell detects a threat, it undergoes "degranulation," explosively releasing these chemicals into the surrounding tissue to initiate an inflammatory response, recruit other immune cells, and neutralise the intruder.
The Spike Protein as a Persistent Agitator
The classical understanding of viral infection suggests that the virus is cleared, and the immune system returns to homeostasis. However, emerging research indicates that the spike protein (specifically the S1 subunit) can persist in the body for months, if not years, after the initial exposure. This persistence has been documented in CD16+ monocytes, which act as reservoirs, circulating the protein throughout the vascular system and depositing it in various tissues.
When the spike protein remains in the body, it acts as a "PAMP" (Pathogen-Associated Molecular Pattern). The mast cells, sensing this foreign and toxic protein continuously, never receive the signal to "stand down." They remain in a state of chronic, low-grade degranulation, leading to:
- —Increased Vascular Permeability: Leading to brain fog and tissue swelling.
- —Neurological Irritation: Through the activation of mast cells in the *dura mater* and blood-brain barrier.
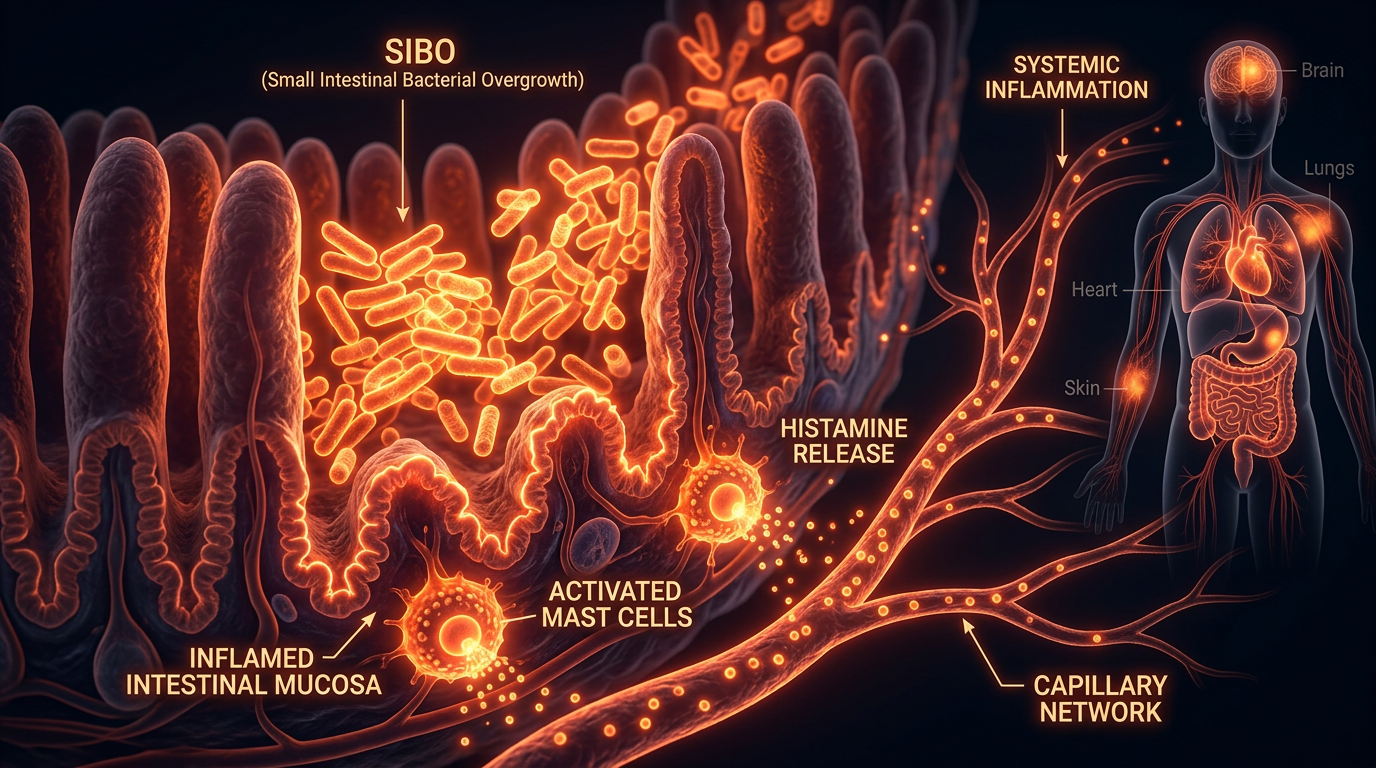
- —Gastrointestinal Distress: As mast cells in the gut lining react to dietary proteins that would otherwise be harmless.
Distinguishing MCAS from Allergy
It is vital to differentiate between a standard IgE-mediated allergy and MCAS. In a standard allergy, the body produces specific antibodies to a substance (like peanuts or pollen). In MCAS, the mast cells have become "twitchy" or hyper-excitable. They trigger in response to non-allergic stimuli—vibrations, temperature changes, stress, or the presence of the spike protein—without the need for traditional allergic antibodies.
Mechanisms at the Cellular Level
The interaction between the spike protein and the mast cell is a complex biochemical "handshake" that goes far beyond simple irritation. Multiple pathways are involved in this pathological activation.
1. The ACE2 Connection and the RAS System
The spike protein is known to bind to the ACE2 (Angiotensin-Converting Enzyme 2) receptor. While much has been written about ACE2 in the lungs, these receptors are also present on the surface of mast cells. When the spike protein binds to ACE2 on a mast cell, it downregulates the enzyme's function. This leads to an imbalance in the Renin-Angiotensin System (RAS), specifically an accumulation of Angiotensin II. Angiotensin II is a potent pro-inflammatory molecule that directly stimulates mast cell degranulation.
2. Toll-Like Receptor (TLR) Activation
Mast cells express various Toll-Like Receptors, specifically TLR4. The spike protein has been shown to act as a ligand for TLR4. When the spike protein plugs into TLR4, it initiates a signalling cascade through the NF-κB pathway. This pathway is the master regulator of inflammation, leading to the production of pro-inflammatory cytokines such as IL-6, TNF-alpha, and IL-1β. This "prime" the mast cell, making it much more likely to release histamine in response to minor triggers.
3. Mitochondrial Dysfunction and Oxidative Stress
The spike protein is a mitochondrial toxin. By disrupting the Electron Transport Chain within the mitochondria of the mast cell, it induces the production of Reactive Oxygen Species (ROS). Mast cells are highly sensitive to oxidative stress; high levels of internal ROS act as a secondary signal for degranulation. This creates a vicious cycle: the spike protein causes oxidative stress, which activates the mast cell, which then releases more inflammatory mediators that create further oxidative stress.
4. The S1 Subunit Persistence
Research by Dr. Bruce Patterson and others has identified that the S1 subunit of the spike protein can be found in non-classical monocytes for over 15 months post-exposure. These monocytes migrate into tissues where mast cells are abundant. The constant proximity of these "protein-laden" monocytes to mast cells ensures a continuous state of activation, preventing the immune system from resetting to its baseline.
Important: The spike protein contains a "prion-like domain" and a "superantigen-like motif" (similar to Staphylococcal Enterotoxin B), which can cause massive, non-specific activation of T-cells and mast cells simultaneously.
Environmental Threats and Biological Disruptors
In a healthy individual, the body might eventually clear or sequester the spike protein. However, we live in an era of unprecedented environmental toxicity that acts synergistically with the spike protein to keep mast cells in a state of permanent agitation.
Electromagnetic Frequencies (EMF)
One of the most overlooked factors in MCAS is the role of EMFs. Mast cells possess Voltage-Gated Calcium Channels (VGCCs). Research has demonstrated that exposure to non-ionising radiation (such as 4G, 5G, and Wi-Fi) can cause an influx of calcium into the mast cell. Calcium is the "trigger" for degranulation. When a body is already burdened by the spike protein, exposure to high levels of EMF acts as a catalyst, significantly lowering the threshold for a full-blown mast cell attack.
Mould and Mycotoxins
Many patients with post-viral MCAS find that their symptoms are exacerbated by their living environment. Mycotoxins from water-damaged buildings are potent mast cell triggers. The spike protein appears to "prime" the immune system such that previously tolerated levels of mould now become highly toxic. This is often referred to as the "Total Load" theory—the spike protein takes up 80% of the body’s detoxification and immune capacity, leaving only 20% to deal with everything else.
Synthetic Chemicals and Glyphosate
The pervasive use of glyphosate in the food supply disrupts the gut microbiome and increases intestinal permeability ("leaky gut"). A leaky gut allows undigested food particles and bacterial endotoxins (LPS) to enter the bloodstream. For a mast cell already hyper-sensitised by the spike protein, the presence of LPS is like throwing petrol on a fire.
- —Endocrine Disruptors: Phthalates and bisphenols mimic hormones and can further destabilise mast cells, which possess receptors for oestrogen (oestrogen is a known mast cell activator).
- —Heavy Metals: Aluminium and mercury, often found in various medical and environmental sources, can accumulate in tissues and act as chronic irritants to the innate immune system.
The Cascade: From Exposure to Disease
The progression from spike protein exposure to chronic MCAS follows a predictable, yet devastating, cascade.
Phase 1: The Initial Insult
Whether through infection or medical intervention, the spike protein enters the systemic circulation. In many cases, the body's natural clearance mechanisms (autophagy and proteasomal degradation) are overwhelmed. The protein begins to bind to ACE2 receptors and accumulate in the endothelium (the lining of the blood vessels).
Phase 2: The "First Hit" – Sensitisation
Mast cells in the vicinity of the spike protein become "primed." They don't necessarily degranulate fully, but they shift into a pro-inflammatory state. At this stage, the patient may feel "mostly fine" but might notice slight increases in fatigue, minor skin rashes, or a new sensitivity to alcohol or high-histamine foods (like red wine or aged cheese).
Phase 3: The "Second Hit" – The Threshold is Crossed
A secondary event occurs. This could be a period of high stress, a secondary infection, exposure to a high-EMF environment, or a subsequent dose of the spike-producing agent. The "Total Load" exceeds the body's compensatory mechanisms. The mast cells begin to degranulate systemically.
Phase 4: Multisystemic Dysfunction
Once the mast cells are chronically active, the symptoms become "multisystemic":
- —Neurological: Migraines, "brain fog," anxiety, insomnia, and POTS (Postural Orthostatic Tachycardia Syndrome) due to the proximity of mast cells to the vagus nerve and blood-brain barrier.
- —Dermatological: Urticaria (hives), flushing, eczema, and dermatographia (skin writing).
- —Gastrointestinal: IBS-like symptoms, bloating, abdominal pain, and sudden food intolerances.
- —Cardiovascular: Palpitations, chest pain, and blood pressure fluctuations.
This state is often self-perpetuating. Histamine itself, once released, can further stimulate mast cells to release more histamine, creating a feedback loop that is incredibly difficult to break without targeted intervention.
What the Mainstream Narrative Omits
The refusal of the medical establishment to acknowledge the link between spike protein persistence and MCAS is one of the greatest clinical failures of the 21st century. Several key truths are being systematically omitted from the mainstream discourse.
The Problem of "The Long Spike"
Mainstream health authorities continue to insist that the spike protein produced by mRNA injections remains localised at the injection site and lasts only for a few days. This has been categorically proven false by multiple peer-reviewed studies (e.g., Castruita et al., 2023; Röltgen et al., 2022) which found spike protein in the blood and lymph nodes for at least 60 days, and in some cases, much longer. By ignoring this persistence, the medical establishment cannot account for the chronic mast cell activation that follows.
The Dismissal of "Long COVID" as Psychosomatic
Because MCAS involves so many different organs and the symptoms can fluctuate wildly, many doctors dismiss patients as having "health anxiety." This gaslighting is exacerbated by the fact that standard blood tests (CBC, metabolic panels) often come back "normal." MCAS requires specific testing—such as chilled plasma histamine, 24-hour urine N-methylhistamine, or serum tryptase (taken during a flare)—which are rarely performed in primary care.
The mRNA Platform and Lipid Nanoparticles (LNPs)
It is not just the spike protein that is the issue. The Lipid Nanoparticles (LNPs) used to deliver the mRNA are themselves highly inflammatory and can act as adjuvants, further stimulating the innate immune response. Some studies suggest that LNPs can trigger mast cell degranulation directly, independent of the spike protein. The mainstream narrative entirely avoids discussing the potential long-term "reprogramming" of the innate immune system (trained immunity) by these synthetic components.
The "S" Protein as a Toxin
Mainstream biology originally treated the spike protein as an inert "key" to the cell. We now know it is a bioactive toxin. It can cross the blood-brain barrier, impair DNA repair (via the p53 pathway), and induce micro-clotting (amyloid-like fibrinoids). Mast cells are the body’s primary detectors of such toxins; their activation is a rational biological response to a dangerous internal threat.
The UK Context
In the United Kingdom, the situation for MCAS and spike-injured patients is particularly dire. The National Health Service (NHS) is built on a model of rigid protocols and "gatekeeping" through General Practitioners (GPs).
Lack of Specialist Access
There are fewer than a dozen true MCAS specialists in the entire UK. Most immunologists in the NHS remain focused on classical IgE allergies and are ill-equipped to handle the complexities of non-IgE mast cell disorders. Consequently, patients are often bounced between cardiology, gastroenterology, and neurology, with no one looking at the "big picture" of mast cell involvement.
The "Post-COVID" Clinic Failure
While the UK government established "Long COVID" clinics, many of these have been criticised for focusing heavily on Cognitive Behavioural Therapy (CBT) and "pacing" rather than addressing the underlying biochemical drivers like spike protein persistence and MCAS. This "psychological-first" approach is a cost-saving measure that ignores the biological reality of the patients' suffering.
Regulatory Silence
The MHRA (Medicines and Healthcare products Regulatory Agency) has been slow to update safety profiles regarding the link between spike-based interventions and the de novo development of MCAS. Despite thousands of Yellow Card reports detailing "allergic-type" reactions and multisystemic inflammation, there remains a lack of official guidance for GPs on how to diagnose or treat post-spike MCAS.
Fact: In the UK, the "wait and see" approach to post-viral syndromes has led to an estimated 2 million people living with self-reported Long COVID, a significant portion of whom meet the diagnostic criteria for MCAS.
Protective Measures and Recovery Protocols
Recovery from spike-induced MCAS requires a multi-pronged approach: clearing the persistent protein, stabilising the mast cell membranes, and reducing the environmental "Total Load."
1. Mast Cell Stabilisers and Antihistamines
The first line of defence is to stop the "leak."
- —H1 and H2 Blockers: A combination of H1 blockers (e.g., Fexofenadine, Loratadine) and H2 blockers (e.g., Famotidine) is often necessary. H2 blockers are particularly important as they help stabilise mast cells in the gut.
- —Natural Stabilisers: Quercetin and Luteolin are flavonoids that have been shown to be more effective than some pharmaceutical stabilisers (like Cromolyn Sodium) in inhibiting the release of pro-inflammatory cytokines from mast cells.
- —Vitamin C: Acts as a natural antihistamine by breaking down the histamine molecule itself.
2. Inhibiting the Spike Protein
To address the root cause, one must attempt to neutralise the persistent spike protein.
- —Nattokinase: A proteolytic enzyme derived from fermented soy (Natto) that has been shown in *in vitro* studies to degrade the SARS-CoV-2 spike protein.
- —Bromelain: Often used in combination with N-Acetylcysteine (NAC), this enzyme can help break down the disulphide bonds in the spike protein, making it easier for the body to clear.
- —Ivermectin: Beyond its controversial use as an antiviral, Ivermectin has a high binding affinity for the spike protein, potentially "masking" it and preventing it from binding to ACE2 receptors and TLRs.
3. Dietary Interventions
A Low-Histamine Diet is essential during the recovery phase. This involves avoiding:
- —Fermented foods (sauerkraut, kombucha).
- —Aged cheeses and cured meats.
- —Leftovers (histamine levels increase as food sits).
- —"Histamine liberators" like citrus fruits and strawberries.
- —Alcohol, which inhibits the DAO (Diamine Oxidase) enzyme responsible for breaking down histamine in the gut.
4. Environmental Optimisation
- —EMF Reduction: Turning off Wi-Fi at night, using hard-wired internet connections, and avoiding 5G-dense areas can significantly reduce the "calcium influx" into mast cells.
- —Mould Remediation: Ensuring the living environment is free from mycotoxins is non-negotiable for an MCAS patient.
- —Vagus Nerve Stimulation: Techniques such as cold-water immersion, deep breathing exercises, and gargling can help shift the body from a "sympathetic" (fight or flight) state into a "parasympathetic" (rest and digest) state, which inherently dampens mast cell activity.
5. Autophagy Induction
Promoting the body’s internal "cleaning system" can help clear spike-laden cells. This is achieved through:
- —Intermittent Fasting: (Under medical supervision).
- —Resveratrol and Spermidine: Compounds that stimulate autophagic pathways.
Summary: Key Takeaways
The emergence of Spike-Induced Mast Cell Activation Syndrome represents a new frontier in clinical pathology. It is a condition where the ancient "alarm system" of the human body has been locked in the "on" position by a persistent, toxic protein.
- —The Spike Protein is the Trigger: Whether from the virus or the injection, the spike protein persists in the body and directly activates mast cells via ACE2 and TLR4 pathways.
- —MCAS is Multisystemic: Symptoms are not "just allergies"; they involve the brain, the gut, the heart, and the nervous system.
- —Synergy of Threats: Environmental factors like EMFs, mould, and glyphosate exacerbate the condition by lowering the degranulation threshold.
- —Mainstream Denial: The medical establishment's failure to recognise spike persistence and the resulting MCAS is leaving millions without proper care.
- —Recovery is Possible: Through a combination of mast cell stabilisers (Quercetin, H1/H2 blockers), spike-degrading enzymes (Nattokinase), and radical environmental changes, the body can be coaxed back into a state of homeostasis.
The path forward for INNERSTANDING readers is one of biological autonomy. By understanding the cellular mechanisms of this syndrome, we can move past the gaslighting of the mainstream narrative and take decisive action to reclaim our health from the persistent presence of the spike protein. The sentinels of our immune system—the mast cells—must be calmed, the toxins cleared, and the biological "noise" of the modern world reduced. Only then can true healing begin.
This article is provided for informational and educational purposes only. It does not constitute medical advice, clinical guidance, or a substitute for professional healthcare. Information reflects cited research at time of publication. Always consult a qualified healthcare professional before acting on any health information.
RESEARCH FOUNDATIONS
Biological Credibility Archive
The SARS-CoV-2 spike protein acts as a potent secretagogue for mast cells, triggering the release of pro-inflammatory cytokines and chemokines that contribute to systemic inflammation.
Longitudinal detection of the S1 subunit of the spike protein in the plasma of long-haul patients supports the hypothesis of a persistent viral reservoir driving chronic mast cell activation.
Mast cell activation syndrome appears to be a significant underlying factor in the development of long-term sequelae following exposure to the spike protein.
Molecular docking and experimental assays demonstrate that the spike protein RBD interacts directly with mast cell receptors, bypassing traditional IgE-mediated pathways to cause degranulation.
Environmental and viral triggers, specifically the spike protein, enhance mast cell sensitivity to histamine-releasing factors, exacerbating allergic responses in susceptible individuals.
Citations provided for educational reference. Verify via PubMed or institutional databases.
Medical Disclaimer
The information in this article is for educational purposes only and does not constitute medical advice, diagnosis, or treatment. Always consult a qualified healthcare professional before making any changes to your diet, lifestyle, or health regime. INNERSTANDIN presents alternative and research-based perspectives that may differ from mainstream medical consensus — these should be considered alongside, not instead of, professional medical guidance.
Read Full DisclaimerReady to learn more?
Continue your journey through our classified biological research.
DISCUSSION ROOM
Members of THE COLLECTIVE discussing "Mast Cell Activation Syndrome: The Allergic Response to Persistent Spike Presence"
SILENT CHANNEL
Be the first to discuss this article. Your insight could help others understand these biological concepts deeper.
THE ARSENAL
Based on Spike Protein & Post-Viral Syndromes — products curated by our research team for educational relevance and biological support.

Vegan Essential Amino Acids – Plant-Powered Protein Building
INNERSTANDING may earn a commission on purchases made through these links. All products are selected based on rigorous educational relevance to our biological research.
RABBIT HOLE
Follow the biological thread deeper