Methane Overgrowth: Deciphering the Archaea-Induced Constipation Cycle
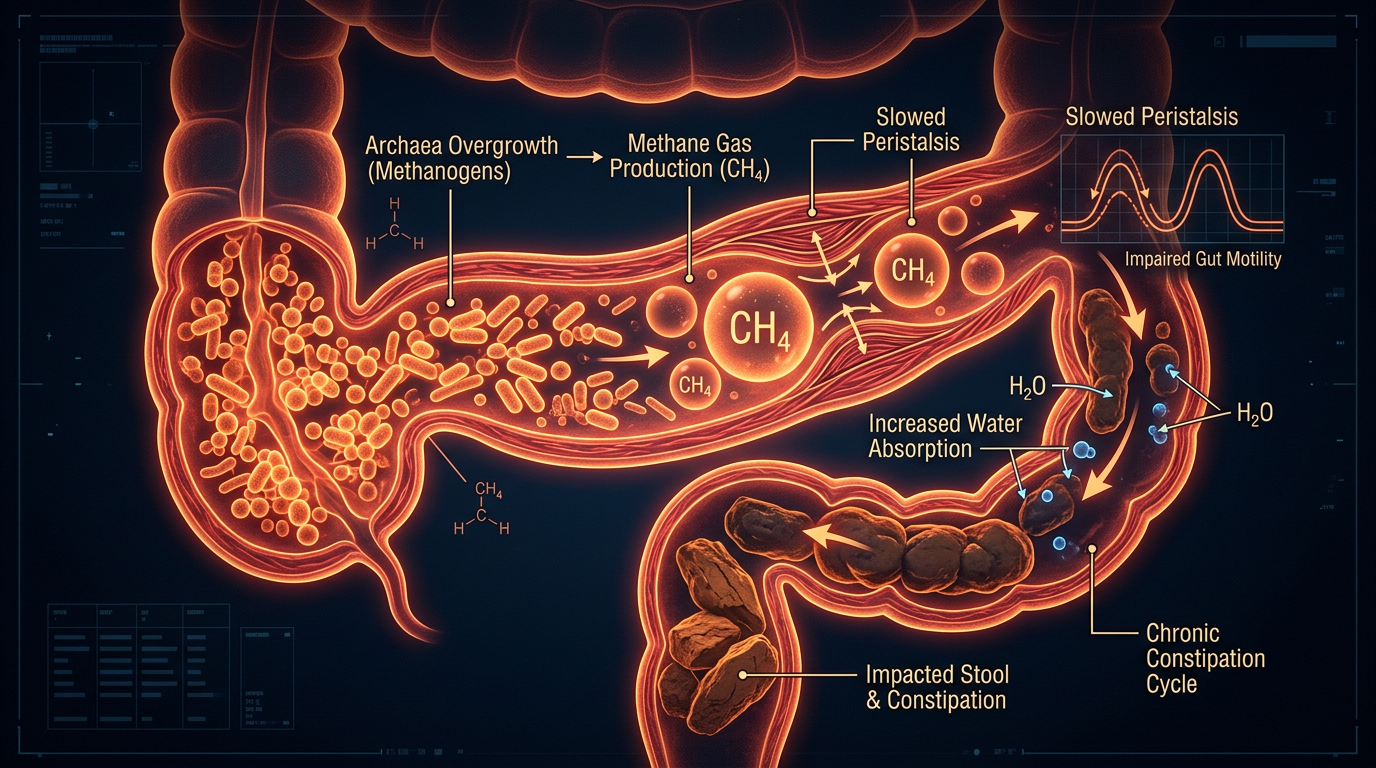
Intestinal Methanogen Overgrowth (IMO) involves archaea that produce methane gas, which acts as a local paralytic to the gut wall. This mechanism explains the intractable constipation often seen in chronic UK SIBO cases.
Overview
The modern landscape of gastroenterology is currently grappling with a phantom that has haunted the human digestive tract for millennia, yet has only recently been properly identified. For decades, millions of individuals—particularly within the United Kingdom—have been relegated to the diagnostic dustbin of "Irritable Bowel Syndrome" (IBS). They have been told that their chronic, intractable constipation, their relentless bloating, and their profound abdominal discomfort are merely functional disorders, often implying a psychological or "stress-related" origin.
However, at INNERSTANDING, we look deeper into the biological bedrock. We are witnessing the emergence of a specific, quantifiable, and devastating microbial imbalance known as Intestinal Methanogen Overgrowth (IMO). Unlike traditional Small Intestinal Bacterial Overgrowth (SIBO), which primarily involves hydrogen-producing bacteria, IMO is driven by a primitive domain of life: the Archaea.
These are not bacteria. They are ancient, single-celled organisms that predate most life forms on Earth. When they colonise the small intestine and over-populate the large intestine, they produce methane gas ($CH_4$) as a metabolic byproduct. This gas is far from an inert waste product; it is a potent, bioactive local paralytic. It acts directly upon the enteric nervous system and the smooth muscle of the gut wall, slowing transit time to a crawl. This creates a vicious, self-sustaining cycle: methane slows the gut, slow transit allows more time for fermentation, and more fermentation provides the fuel for more methane.
This article aims to deconstruct the "Methane Overgrowth" phenomenon. We will explore how these ancient organisms have exploited the weaknesses of the modern British lifestyle, why the mainstream medical narrative continues to fail those suffering from chronic constipation, and what the biological reality is for those trapped in the archaea-induced paralysis of the gastrointestinal tract.
##
The Biology — How It Works
To understand methane overgrowth, one must first understand the distinction between the domains of life. Archaea were once classified as bacteria, but genetic sequencing has revealed they are as different from bacteria as humans are from fungi. In the human gut, the primary culprit is *Methanobrevibacter smithii*.
The Scavengers of the Gut
Archaea are "hydrogen scavengers." They do not feed directly on the carbohydrates or fibres you ingest. Instead, they exist in a syntrophic (cross-feeding) relationship with hydrogen-producing bacteria (such as *Ruminococcus* or *Christensenellaceae*). When bacteria ferment dietary fibres, they release hydrogen gas ($H_2$) as a waste product. Under normal conditions, this gas is absorbed into the bloodstream or passed. However, in an IMO state, *M. smithii* consumes this hydrogen.
The biochemical equation for methanogenesis is: $4H_2 + CO_2 \rightarrow CH_4 + 2H_2O$
By consuming four molecules of hydrogen to produce just one molecule of methane, these archaea act as a "metabolic sink." They actually help bacteria ferment more efficiently by removing the hydrogen pressure that would otherwise inhibit bacterial metabolism. This synergy makes IMO particularly difficult to eradicate; you are not just fighting one organism, but an entire metabolic ecosystem.
The Small Intestine vs. The Large Intestine
While methane-producing archaea are natural inhabitants of the human colon (large intestine), they are not supposed to be present in high concentrations in the small intestine. The small intestine is the site of nutrient absorption. When *M. smithii* migrates upward or over-proliferates in this zone, the methane gas produced is immediately in contact with the most sensitive regulatory mechanisms of digestive motility.
UK STAT: Current estimates suggest that up to 35% of the UK population are "methane producers," yet fewer than 5% of those with chronic constipation have ever been screened for Intestinal Methanogen Overgrowth, leading to decades of mismanaged treatment.
##
Mechanisms at the Cellular Level
The most revolutionary finding in recent neuro-gastroenterology is that methane gas is a neuromuscular modulator. It does not just cause "gas"; it actively reconfigures how the gut moves.
The Paralytic Effect on the MMC
The Migrating Motor Complex (MMC) is the "inter-digestive housekeeper" of the gut. It is a wave of electromechanical activity that sweeps through the intestines every 90 to 120 minutes during fasting states, clearing out undigested food and microbial debris.
Methane gas has been shown in clinical models to slow intestinal transit by as much as 59%. It achieves this by inhibiting the firing of the cholinergic neurons within the enteric nervous system (ENS). When methane levels rise, the amplitude and frequency of the MMC waves decrease. The gut essentially enters a state of local paralysis. This is not a "lack of fibre" issue; it is a "signalling interference" issue.
The Serotonin Connection
Approximately 95% of the body's serotonin ($5-HT$) is produced in the gut, where it regulates motility and sensation. Methane overgrowth appears to disrupt the enterochromaffin cells' ability to release serotonin appropriately. By dampening the serotonergic response, the "push" required to move fecal matter through the colon is diminished. This leads to the characteristic "pellet-like" stools and the sensation of incomplete evacuation common in methane-dominant patients.
Ion Channel Interference
At the cellular level, methane may interfere with calcium-activated potassium channels in the smooth muscle cells of the intestine. By altering the electrical potential of these cells, methane increases the threshold required for a muscular contraction to occur. In simpler terms, the gut wall becomes "numb" to the presence of waste, failing to trigger the necessary contractions to move it forward.
##
Environmental Threats and Biological Disruptors
Why is this happening now? Why are we seeing an explosion of IMO in the 21st century? The answer lies in the systematic degradation of the human internal environment.
The Glyphosate Impact
The UK agricultural sector heavily utilises glyphosate-based herbicides. While marketed as safe for humans because we lack the "shikimate pathway," this pathway *is* present in our gut bacteria. Glyphosate acts as a selective antibiotic, killing off beneficial, diverse bacteria while allowing hardy organisms like archaea and certain pathogenic clades to thrive. When the microbial diversity of the gut is flattened, *M. smithii* finds an empty ecological niche to occupy.
The Pharmaceutical Trigger: PPIs and Antibiotics
The British medical system is overly reliant on Proton Pump Inhibitors (PPIs) for acid reflux. By suppressing stomach acid, we remove the primary chemical barrier that prevents the ingestion of environmental archaea and bacteria. Furthermore, repeated rounds of broad-spectrum antibiotics—often prescribed for minor respiratory infections—decimate the "policing" bacteria of the small intestine, paving the way for archaeal colonisation.
Water Quality and Heavy Metals
Archaea are known to thrive in environments high in certain minerals and heavy metals. The ageing piping infrastructure in many UK cities, combined with the presence of microplastics in drinking water, may provide the inorganic scaffolding necessary for archaeal biofilms to anchor themselves to the intestinal mucosa.
- —Microplastics: Act as "Trojan horses" for microbial attachment.
- —Chlorination: While necessary for safety, chronic exposure to chlorinated tap water can alter the delicate balance of the mucosal microbiome.
FACT: Archaea are extremophiles. They can survive boiling, freezing, and high-pressure environments. This makes them significantly more resilient to standard "gut cleanses" and mild herbal interventions than common bacteria.
##
The Cascade: From Exposure to Disease
The progression from a healthy gut to a methane-paralysed system follows a predictable, yet devastating, cascade.
- —The Initial Insult: This is usually a "trigger event"—a bout of food poisoning (post-infectious SIBO), a period of high chronic stress that shuts down the MMC, or a heavy course of antibiotics.
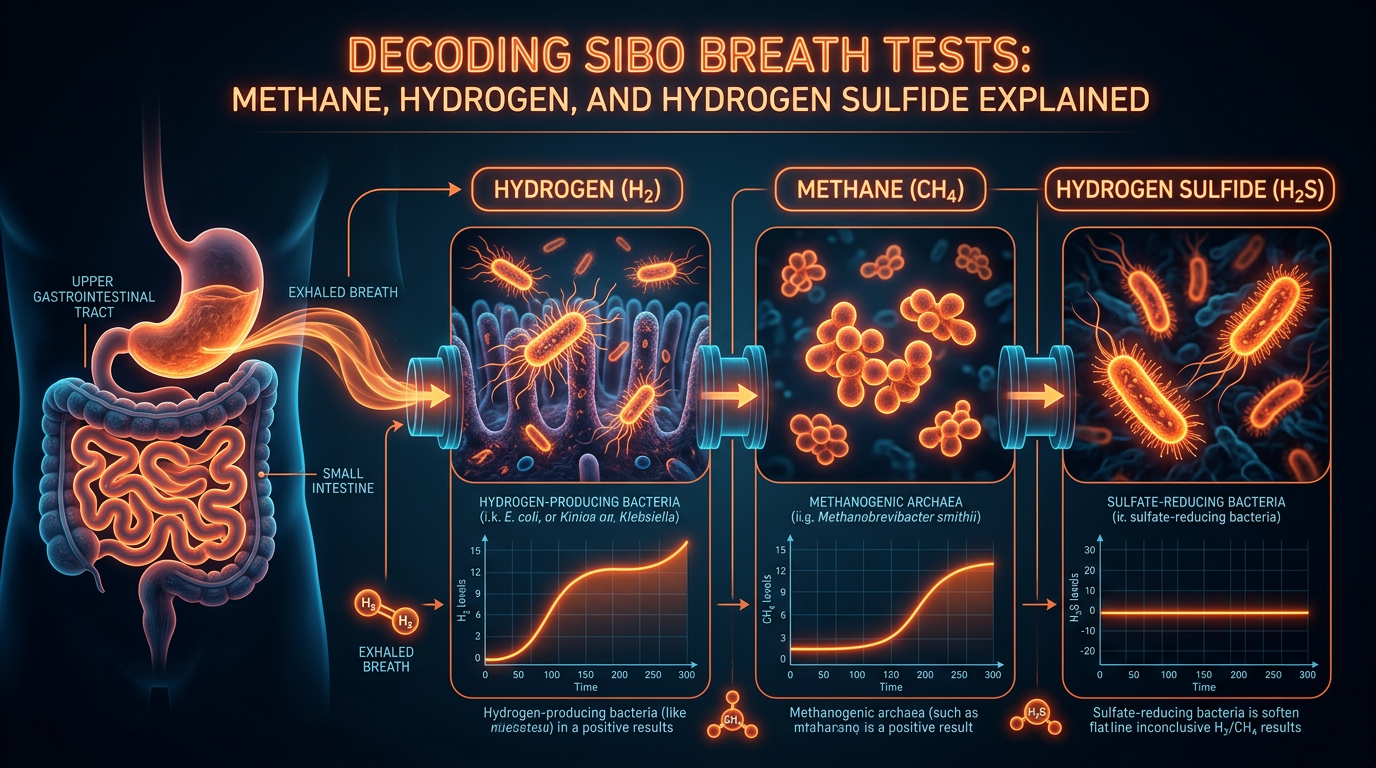
- —The Hydrogen Surge: Damaged motility leads to "stagnant loops" in the small intestine. Hydrogen-producing bacteria (like *E. coli* or *Klebsiella*) begin to overgrow, fermenting even small amounts of dietary sugars.
- —The Archaeal Recruitment: *M. smithii* and other methanogens sense the high hydrogen levels. They migrate from the colon into the small intestine to feed.
- —The Methane Feedback Loop: Methanogens produce methane. Methane slows the gut. The slowed gut causes more stagnation. More stagnation feeds more bacteria. More bacteria produce more hydrogen. More hydrogen feeds more methanogens.
- —Systemic Consequences: As the "clog" worsens, the intestinal lining becomes inflamed and permeable (Leaky Gut). Metabolic byproducts and endotoxins (LPS) leak into the bloodstream, leading to systemic symptoms: brain fog, chronic fatigue, and skin issues.
By the time a patient in the UK presents to their GP with "constipation," they are often already in Phase 4 of this cascade. The recommendation to "eat more bran" at this stage is akin to adding more cars to a motorway that is already blocked by a multi-car pile-up.
##
What the Mainstream Narrative Omits
The current standard of care for constipation in the UK (and much of the Western world) is fundamentally flawed because it ignores the gas-motility axis.
The "Fibre" Fallacy
Mainstream dietetics almost universally suggests increasing fibre intake for constipation. In the context of IMO, this is dangerous advice. Fibre is the primary fuel for the hydrogen-producing bacteria that feed the methanogens. Increasing fibre in a methane-overgrown gut often leads to "explosive" bloating and increased pain, as the production of methane gas accelerates.
The Misuse of Laxatives
The NHS spends millions annually on osmotic laxatives like Macrogol (Movicol). While these draw water into the stool to soften it, they do absolutely nothing to address the microbial overgrowth or the underlying paralytic effect of the methane. Patients become "laxative dependent," needing ever-higher doses to force waste through a gut that is biologically "turned off."
The Breath Test Gap
The "Gold Standard" for SIBO diagnosis in the UK is the glucose or lactulose breath test. However, many NHS trusts only measure Hydrogen. If a patient is a methane-producer, the methanogens will consume the hydrogen as fast as the bacteria produce it. This results in a "Flat Line" hydrogen reading, which is often misinterpreted as a "negative" test. The patient is told they are fine, while they are actually harbouring a massive methane overgrowth that was simply never measured.
ALARMING FACT: A "negative" hydrogen breath test in a patient with severe constipation is a classic clinical indicator of "Hydrogen-Stealing" by methanogens. Without measuring Methane ($CH_4$), the test is scientifically incomplete.
##
The UK Context
The United Kingdom presents a unique set of challenges for the IMO sufferer. The combination of our dietary habits, our healthcare structure, and our environmental stressors has created a "perfect storm" for archaeal overgrowth.
The "Beige Diet" and Processed Grains
The traditional British diet—high in processed wheats, "beige" carbohydrates, and pasteurised dairy—is a paradise for hydrogen-producing bacteria. These foods are rapidly fermented in the upper GI tract, providing a constant stream of $H_2$ for the *M. smithii* populations.
The NHS Wait-Times and Diagnostic Inertia
A patient with IMO will often wait months for a GP appointment, only to be given a 10-minute slot where their symptoms are dismissed as "stress." Referrals to gastroenterology can take up to a year, during which time the methanogen population becomes deeply entrenched in hardy biofilms. Private testing for methane is available but often prohibitively expensive for the average citizen, creating a two-tier system of digestive health.
Soil Health and Trace Minerals
British soils have been significantly depleted of selenium and magnesium over the last century of industrial farming. Magnesium is a natural calcium-channel blocker that assists in muscle relaxation and gut motility. A magnesium-deficient population is already predisposed to slower transit; add methane to that equation, and the results are catastrophic.
##
Protective Measures and Recovery Protocols
Recovery from IMO requires a sophisticated, multi-phase approach that goes beyond simple probiotics. In fact, most commercial probiotics (containing *Lactobacillus* and *Bifidobacterium*) can actually worsen the bloating in the short term.
Phase 1: Starve the Producers (Dietary Intervention)
The goal is not to starve the person, but to starve the hydrogen-producers.
- —The Biphasic Diet / Low FODMAP: Reducing fermentable carbohydrates (Fructans, GOS, Lactose, Fructose, Polyols) is essential to lower the hydrogen supply.
- —Meal Spacing: Allowing 4-5 hours between meals to permit the MMC to function. No "grazing."
Phase 2: Break the Biofilm and Eradicate
Archaea protect themselves with a "pseudo-murein" cell wall, which is much tougher than a bacterial cell wall.
- —Allicin (Garlic Extract): Concentrated allicin is the most researched natural agent against *M. smithii*. Unlike standard garlic (which is high in FODMAPs), allicin extract is highly effective at inhibiting methanogenesis.
- —Oregano Oil and Neem: These acts as broad-spectrum antimicrobials to reduce the hydrogen-producing bacterial load.
- —Specific Antibiotics: In clinical settings, a combination of Rifaximin (which stays in the gut) and Neomycin or Metronidazole is often required to "kill" the archaea.
Phase 3: Prokinetics (The "Spark Plug")
This is the most skipped step in the UK. Once you kill the overgrowth, you must ensure the "housekeeping wave" is restored, or the overgrowth will return within weeks.
- —Ginger and Artichoke Extracts: Natural prokinetics that stimulate the MMC.
- —Low-dose Erythromycin or Prucalopride: Pharmaceutical options that act as "motility stimulators" to keep the small intestine clear.
Phase 4: Environmental and Lifestyle Fortification
- —Vagus Nerve Stimulation: Techniques like cold-water immersion, deep diaphragmatic breathing, and gargling can help "re-set" the connection between the brain and the gut.
- —Magnesium Supplementation: Using magnesium citrate or oxide to support osmotic balance and muscle function.
- —Water Filtration: Using high-quality filters to remove chlorine and microplastics from daily intake.
##
Summary: Key Takeaways
The "Methane Overgrowth" crisis is a silent epidemic of paralysis. To truly understand why chronic constipation persists in the face of conventional treatment, we must shift our focus from "stool bulk" to "gas signalling."
- —Archaea are not bacteria. They are ancient, resilient organisms that require specific, targeted strategies for eradication.
- —Methane is a local paralytic. It inhibits the enteric nervous system, slowing the gut's "housekeeping" waves by over 50%.
- —Hydrogen is the fuel. To stop methane, you must address the hydrogen-producing bacteria and the dietary factors that feed them.
- —Mainstream medicine is lagging. The over-reliance on fibre and the failure to measure methane in breath tests leaves millions of UK citizens without an accurate diagnosis.
- —Motility is the key. Eradication is useless without a "prokinetic" strategy to keep the gut moving and prevent re-colonisation.
For the researcher and the sufferer alike, the message is clear: the gut is not just a tube; it is a sophisticated, bio-electric ecosystem. When we allow ancient organisms like *M. smithii* to hijack our internal signalling, we lose more than just digestive regularity—we lose our systemic vitality. True "inner standing" of our health begins with the realisation that the invisible gases within us are often the ones pulling the strings of our physiology. It is time to break the cycle of stagnation and reclaim the rhythm of the human body.
This article is provided for informational and educational purposes only. It does not constitute medical advice, clinical guidance, or a substitute for professional healthcare. Information reflects cited research at time of publication. Always consult a qualified healthcare professional before acting on any health information.
RESEARCH FOUNDATIONS
Biological Credibility Archive
Citations provided for educational reference. Verify via PubMed or institutional databases.
Medical Disclaimer
The information in this article is for educational purposes only and does not constitute medical advice, diagnosis, or treatment. Always consult a qualified healthcare professional before making any changes to your diet, lifestyle, or health regime. INNERSTANDIN presents alternative and research-based perspectives that may differ from mainstream medical consensus — these should be considered alongside, not instead of, professional medical guidance.
Read Full DisclaimerReady to learn more?
Continue your journey through our classified biological research.
DISCUSSION ROOM
Members of THE COLLECTIVE discussing "Methane Overgrowth: Deciphering the Archaea-Induced Constipation Cycle"
SILENT CHANNEL
Be the first to discuss this article. Your insight could help others understand these biological concepts deeper.
THE ARSENAL
Based on SIBO & Small Intestine Health — products curated by our research team for educational relevance and biological support.

Magnesium Blend – The Most Important Mineral

Clean Slate – Detoxes thousands of chemicals,heavy metals, pesticides, allergens, mold spores and fungus

Vegan Essential Amino Acids – Plant-Powered Protein Building
INNERSTANDING may earn a commission on purchases made through these links. All products are selected based on rigorous educational relevance to our biological research.
RABBIT HOLE
Follow the biological thread deeper