The Migrating Motor Complex: The Biological Janitor of the Gut
The Migrating Motor Complex (MMC) is a distinct electromechanical wave that clears residual debris and bacteria from the small intestine during fasting. Dysfunction in this biological mechanism is the primary reason for SIBO recurrence in the UK population.
Overview
In the intricate landscape of human physiology, the gastrointestinal tract is often reduced to a mere conduit for nutrient absorption and waste excretion. However, for those of us at INNERSTANDING, the gut represents a sophisticated electromechanical system that requires constant, rhythmic maintenance to prevent biological collapse. At the heart of this maintenance system lies the Migrating Motor Complex (MMC)—a cyclic, inter-digestive motility pattern that functions as the "biological janitor" of the small intestine.
The MMC is not merely a digestive movement; it is a distinct, highly coordinated sequence of electromechanical waves that occur only during the fasted state. Its primary evolutionary purpose is to sweep residual undigested food, cellular debris, and, most crucially, opportunistic bacteria out of the small intestine and into the colon. When this janitorial service fails, the result is stagnation. In the world of clinical gastroenterology, this stagnation provides the perfect ecological niche for Small Intestinal Bacterial Overgrowth (SIBO).
For the British population, the failure of the MMC is arguably the most significant undiagnosed health crisis of the modern era. While the mainstream medical establishment focuses on the eradication of bacteria through broad-spectrum antibiotics, they consistently fail to address the underlying mechanical failure that allowed the bacteria to colonize the small intestine in the first place. This systemic oversight explains why SIBO recurrence rates in the UK remain staggeringly high, often exceeding 60% within six months of treatment.
The MMC is the barrier between a healthy, sterile small intestine and a pathological state of chronic fermentation. To understand the MMC is to understand the root cause of the "IBS" epidemic currently sweeping through the UK, burdening the NHS and diminishing the quality of life for millions. This article will dissect the biological, cellular, and environmental factors that govern this complex, exposing the truths that the pharmaceutical-industrial complex often overlooks.
According to recent data from the British Society of Gastroenterology, "IBS" affects up to 15% of the UK population, yet independent research suggests that up to 78% of these cases are actually SIBO, driven primarily by a deficient Migrating Motor Complex.
---
The Biology — How It Works
The Migrating Motor Complex is a masterpiece of biological orchestration. Unlike the peristalsis that occurs while we eat—which is designed to mix food with enzymes and push it slowly through the tract for absorption—the MMC is an "inter-digestive" event. It only wakes up when the stomach and small intestine are empty.
The MMC operates in a cycle that typically lasts between 90 and 120 minutes. It originates in the stomach or the proximal duodenum and migrates slowly toward the ileocaecal valve, the gateway to the large intestine. This cycle is divided into four distinct phases, each with a specific physiological role.
Phase I: The Quiescent Period
Phase I is a period of absolute stillness. It lasts approximately 45 to 60 minutes, accounting for nearly half of the total cycle. During this time, there is virtually no contractile activity. It is a period of "recharging," where the enteric nervous system prepares for the subsequent waves of activity. In a healthy individual, this silence is necessary, but in a dysfunctional gut, this phase can become pathologically extended, leading to prolonged stagnation.
Phase II: The Random Contractile Period
Phase II lasts about 30 to 45 minutes. During this phase, we see irregular electrical activity and sporadic contractions. These contractions are not yet coordinated enough to move material over long distances, but they begin the process of "shuffling" residual contents. It is during Phase II that we often see the influence of hormones like ghrelin—the "hunger hormone"—which begins to prime the system for the big sweep.
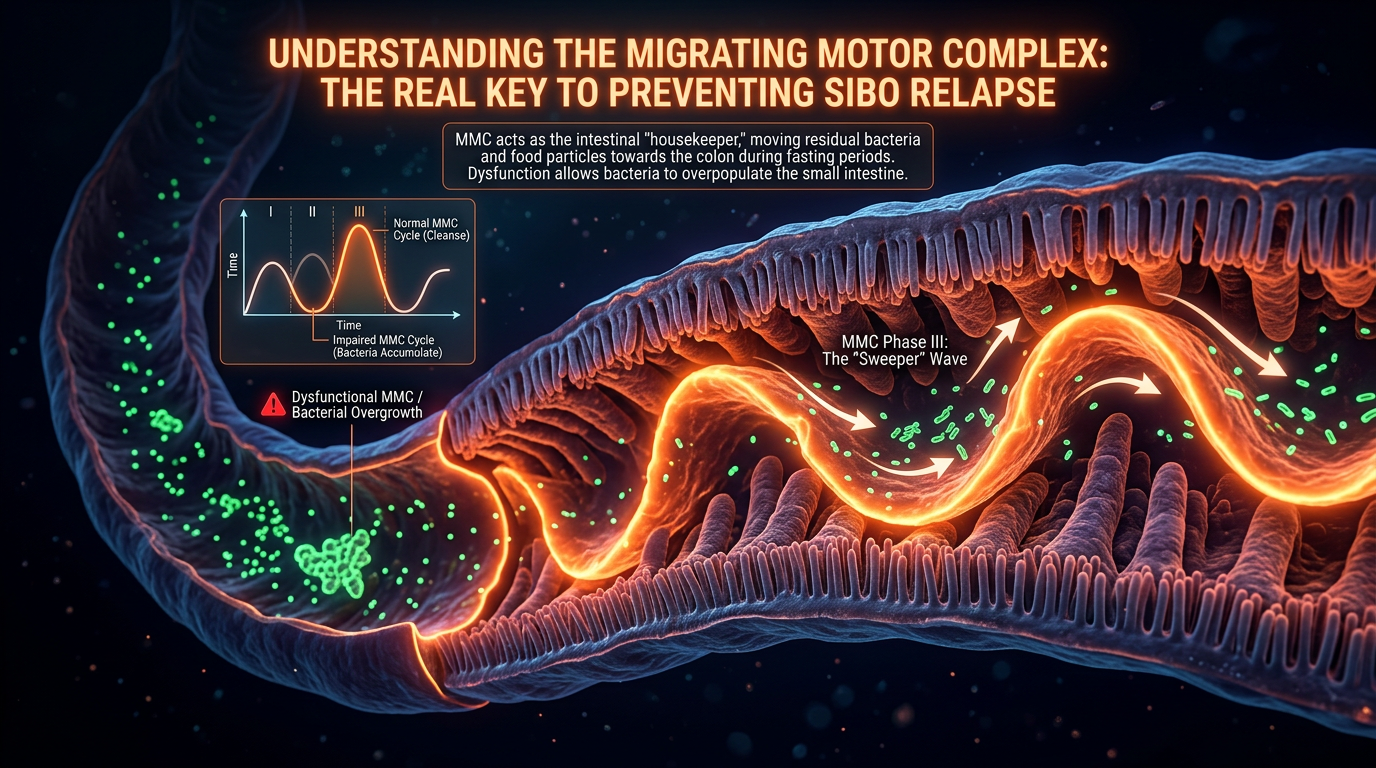
Phase III: The Housekeeper Wave
This is the most critical phase for intestinal health. Phase III consists of high-amplitude, rhythmic contractions that occur at the maximal frequency for the specific segment of the gut. In the stomach, this occurs at a rate of 3 contractions per minute; in the duodenum, it reaches 11 to 12 contractions per minute.
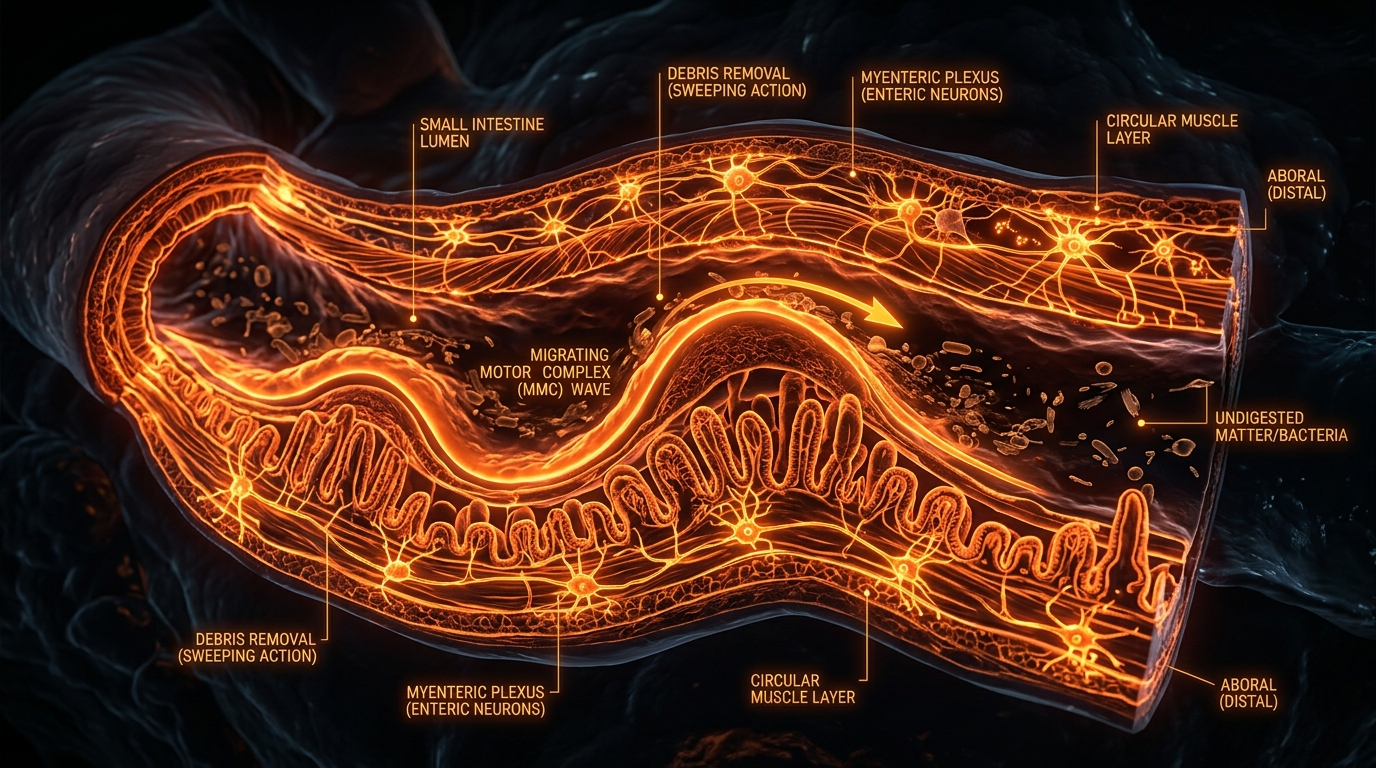
Phase III is the "Biological Janitor" in full force. It creates a powerful pressure gradient that acts like a physical broom, clearing out large particles of undigested fibre, sloughed-off epithelial cells, and, crucially, the bacterial colonies that have attempted to migrate upwards from the colon. Without a robust Phase III, the small intestine becomes a stagnant pond, ripe for bacterial fermentation and the production of toxic gases like hydrogen and methane.
Phase IV: The Transition
Phase IV is a brief period of transition between the intense activity of Phase III and the return to the silence of Phase I. It serves as a physiological "cool down," ensuring that the mechanical energy of the sweep is dissipated before the cycle resets.
The entire process is governed by a delicate hormonal and neural balance. The hormone Motilin, secreted by M-cells in the upper small intestine, is the primary chemical trigger for the MMC. Motilin levels rise and fall in perfect synchrony with the MMC phases, peaking just before Phase III begins. However, the moment you consume even a small amount of calories—be it a biscuit, a sugary tea, or a snack—motilin production is instantly suppressed, the MMC is aborted, and the body shifts back into the digestive mode. This is why the "snacking culture" of the modern UK is a direct threat to gut motility.
---
Mechanisms at the Cellular Level
To truly understand why the MMC fails, we must look deeper than the muscular walls of the intestine. We must look at the "pacemakers" of the gut: the Interstitial Cells of Cajal (ICCs).
The Interstitial Cells of Cajal (ICCs)
The ICCs are specialised cells that sit between the nerve endings and the smooth muscle cells of the gut. They are the electrical conductors of the gastrointestinal tract. Just as the heart has a pacemaker to ensure a regular heartbeat, the gut has ICCs to generate the "slow waves" of electrical activity that allow the MMC to occur.
If the ICCs are damaged or diminished in number, the electrical signal cannot propagate. This results in a "broken circuit." Even if the muscles are healthy and the hormones are present, the coordination required for Phase III contractions is lost. Research into chronic SIBO patients has consistently shown a significant reduction in the density of ICCs, particularly in the jejunum and ileum. This loss of cellular architecture is often irreversible if the underlying cause is not addressed, leading to permanent motility deficits.
The Enteric Nervous System (ENS) and the Myenteric Plexus
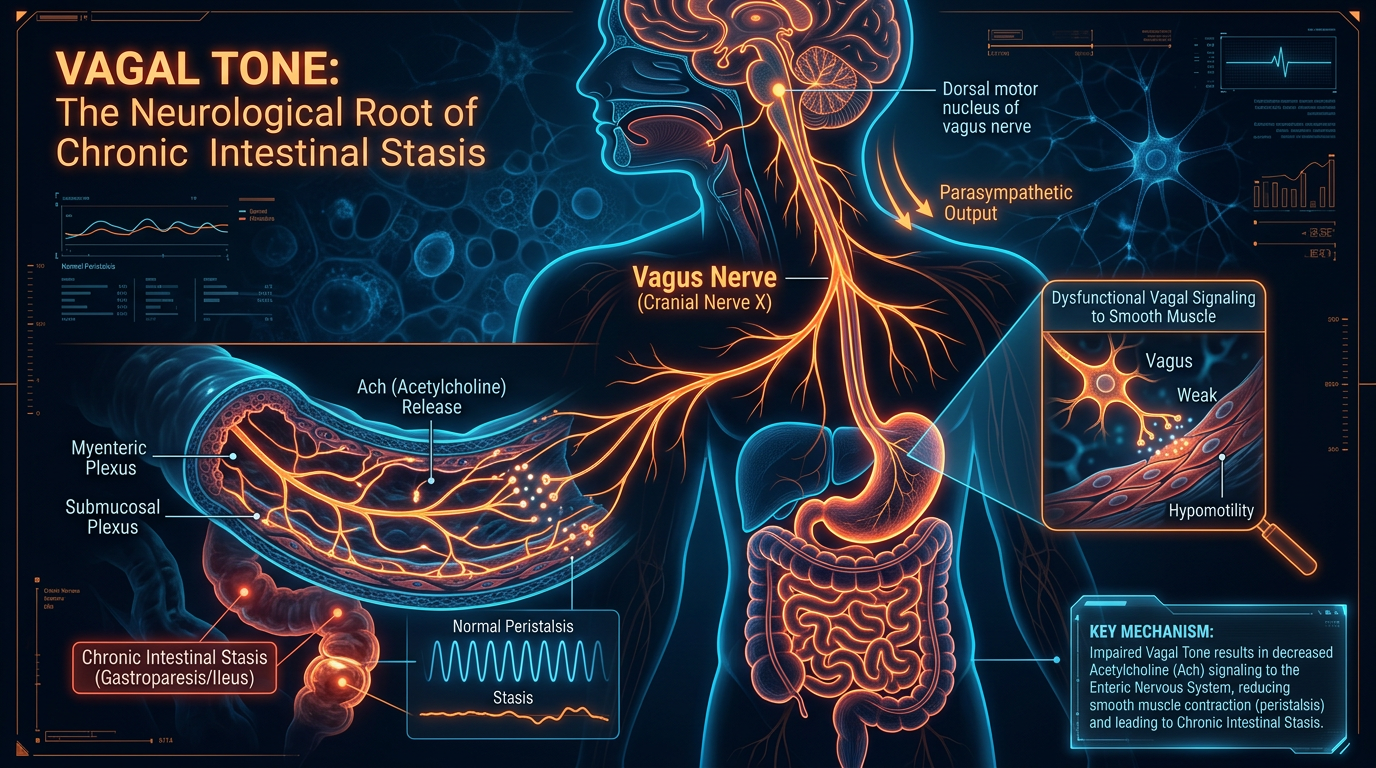
The MMC is also regulated by the Enteric Nervous System (ENS), often referred to as the "second brain." The myenteric plexus (Auerbach’s plexus), situated between the longitudinal and circular muscle layers, acts as the local command centre.
During the inter-digestive state, the ENS integrates signals from the central nervous system (via the Vagus Nerve) and local chemical sensors to initiate the MMC. The Vagus Nerve acts as the "master switch." When the body is in a Parasympathetic state (Rest and Digest), the Vagus Nerve sends signals that promote MMC activity. Conversely, when the Sympathetic Nervous System (Fight or Flight) is dominant, the Vagus Nerve is inhibited, and the MMC is shut down.
The Role of Motilin Receptors
Motilin does not act in a vacuum. It must bind to specific receptors located on the smooth muscle cells and the enteric neurons. In states of chronic inflammation—common in the UK diet of ultra-processed foods—these receptors can become "downregulated" or desensitised. This means that even if the body produces enough Motilin, the gut fails to respond to the signal. This is a form of "Motilin Resistance," analogous to Insulin Resistance in Type 2 Diabetes, and it represents a major hurdle in recovering gut function.
Crucial Fact: The loss of Interstitial Cells of Cajal (ICCs) is now considered a hallmark of "Post-Infectious IBS." This cellular destruction is frequently triggered by a common bout of food poisoning, which most Britons dismiss as a "24-hour bug."
---
Environmental Threats and Biological Disruptors
The modern environment is systematically designed to destroy the Migrating Motor Complex. From the way we eat to the chemicals we are exposed to, the "Biological Janitor" is under constant assault.
The Snacking Epidemic and "Grazing"
The most immediate threat to the MMC is the frequency of eating. As established, the MMC only occurs during a fasted state, typically beginning 90 to 120 minutes after a meal is fully cleared from the stomach. In the UK, the culture of "grazing"—eating small snacks throughout the day—means that many individuals never enter a true inter-digestive state.
Every time you consume a snack, you reset the clock. If you eat every three hours, your body may never complete a full Phase III housekeeper wave. This leaves the "trash" in the small intestine for the entire day, allowing bacteria to feast and multiply.
Ultra-Processed Foods (UPFs) and Emulsifiers
The British diet is the most processed in Europe. Ultra-processed foods contain emulsifiers (like carboxymethylcellulose and polysorbate 80) designed to give products a long shelf life. However, these chemicals have been shown to degrade the protective mucus layer of the gut. When the mucus layer is thinned, the underlying ENS and ICCs are exposed to bacterial toxins and inflammatory markers, leading to the cellular damage that halts the MMC.
Glyphosate and Pesticides
Glyphosate, the active ingredient in many common weedkillers used in UK agriculture, is a potent antimicrobial and an endocrine disruptor. It has been shown to interfere with the Shikimate pathway in gut bacteria, but its impact on human motility is equally concerning. Glyphosate can act as a "pseudo-neurotransmitter," interfering with the acetylcholine signals required for muscle contraction in the gut. By disrupting the neural signalling of the myenteric plexus, glyphosate effectively "paralyses" the MMC.
The Stress Response
The UK is currently facing a mental health crisis, with record levels of cortisol-driven stress. Stress is the natural enemy of the MMC. When the body perceives a threat (whether it’s a deadline at work or traffic in London), it prioritises blood flow to the limbs and the heart, away from the digestive tract. The Sympathetic Nervous System inhibits the Vagus Nerve, which in turn inhibits the release of Motilin. Chronic stress equals a chronic lack of janitorial service in the gut.
---
The Cascade: From Exposure to Disease
How does a healthy person transition into a chronic SIBO patient? The journey is a predictable cascade of biological failures, often beginning with a single event: Food Poisoning.
The CdtB Toxin and Molecular Mimicry
Most cases of SIBO in the UK can be traced back to an episode of gastroenteritis caused by bacteria such as *Salmonella*, *E. coli*, *Campylobacter*, or *Shigella*. These bacteria release a specific toxin called Cytolethal Distending Toxin B (CdtB).
When the body’s immune system detects CdtB, it produces antibodies to fight it. However, due to a phenomenon known as molecular mimicry, the CdtB toxin looks remarkably similar to a human protein called Vinculin. Vinculin is a critical structural protein found in the Interstitial Cells of Cajal (ICCs) and the enteric nerves.
The Autoimmune Turn
In many individuals, the immune system becomes "confused." After the initial infection is cleared, the body continues to produce anti-CdtB antibodies, which then begin to attack the Vinculin in the gut’s own pacemaker cells. This is an autoimmune reaction. The result is the destruction of the ICCs.
As the density of ICCs drops, the MMC weakens. The "housekeeper wave" becomes shallow, infrequent, or disappears entirely. This is the "Smoking Gun" of SIBO recurrence. You can take all the Rifaximin (antibiotics) you want, but if your pacemakers are gone and your MMC is dead, the bacteria *will* return. They are simply moving into an empty, uncleaned house.
The Stagnation-Fermentation Loop
Once the MMC is compromised, the small intestine begins to accumulate debris. Bacteria from the colon (where they belong) sense the lack of activity and begin to migrate upward through the ileocaecal valve. They colonize the small intestine, where they find a steady supply of undigested carbohydrates from the host’s diet.
These bacteria ferment the food, producing hydrogen, methane, or hydrogen sulfide gases. These gases don't just cause bloating; they further inhibit motility. Methane, in particular, has been shown to act as a local anaesthetic to the gut wall, slowing down transit even further. This creates a vicious cycle: poor motility leads to SIBO, and SIBO produces gases that worsen poor motility.
---
What the Mainstream Narrative Omits
The current medical approach to gut health in the UK is fundamentally flawed. If you visit a GP with symptoms of bloating, abdominal pain, and altered bowel habits, you will likely be diagnosed with "IBS" and told to "manage your stress" or try a "Low FODMAP diet."
This narrative omits three crucial truths:
- —IBS is a symptom, not a cause. It is a label used when doctors don't know what is wrong. In the vast majority of cases, the "IBS" is actually SIBO caused by MMC dysfunction.
- —Antibiotics are not a cure. Standard medical practice treats SIBO as an infection to be killed. But SIBO is not a primary infection; it is a secondary consequence of mechanical failure. Treating SIBO with antibiotics without addressing the MMC is like mopping up water from a leaking pipe without fixing the pipe itself.
- —The "Eat Little and Often" Advice is Dangerous. Many dieticians still recommend eating small meals frequently to "keep the metabolism going." For someone with SIBO or a compromised MMC, this is the worst possible advice. It ensures the MMC never turns on, effectively guaranteeing that the bacteria will remain in the small intestine.
The mainstream narrative serves the interests of pharmaceutical companies that profit from the repeated sale of antibiotics and "symptom management" drugs. It does not serve the patient who is seeking a permanent resolution to their digestive suffering.
---
The UK Context
The situation in the United Kingdom is uniquely challenging. The National Health Service (NHS), while a cornerstone of British society, is ill-equipped to handle the nuances of MMC dysfunction and SIBO.
Lack of Diagnostic Access
Getting a SIBO breath test on the NHS is notoriously difficult. Most Trusts do not offer them, and many GPs are not even aware they exist. Consequently, patients are left to suffer for years with an "IBS" diagnosis, unaware that their "janitor" has been on strike since they had food poisoning in Magaluf five years ago.
The "IBS" Dustbin
In the UK, "IBS" has become a "dustbin diagnosis"—a place where patients are put when basic blood tests and colonoscopies come back clear. This "all in your head" approach ignores the very real, measurable autoimmune destruction of the gut’s nervous system.
The Antibiotic Paradox
The UK has made great strides in reducing unnecessary antibiotic prescriptions for respiratory infections, yet we still over-prescribe them for vague "gut issues" without proper testing. Ironically, certain antibiotics (like erythromycin) can actually *stimulate* the MMC in low doses, but because they are only used at high doses to kill bacteria, their potential as motility agents is largely ignored by mainstream practitioners.
---
Protective Measures and Recovery Protocols
If the MMC is the key to gut health, how do we protect it, and more importantly, how do we restore it?
1. Strategic Meal Spacing
The most powerful tool for activating the MMC costs nothing. You must stop snacking. Aim for at least 4 to 5 hours between meals, and a minimum of 12 hours of overnight fasting. This provides the necessary "window" for the MMC to complete multiple Phase III cycles. During these windows, you must consume only water, black coffee, or plain tea. Any caloric intake—even a splash of milk—will abort the process.
2. Prokinetic Therapy
For those with damaged ICCs, the body needs a "nudge" to initiate the MMC. This is where prokinetics come in. Unlike laxatives, which simply irritate the colon to force a bowel movement, prokinetics work on the enteric nervous system to stimulate Phase III of the MMC.
- —Natural Prokinetics: Ginger root and Artichoke leaf extract have been clinically shown to stimulate gastric emptying and MMC activity.
- —Pharmaceutical Prokinetics: Low-dose Naltrexone (LDN), low-dose Erythromycin, or Prucalopride (Resolor) are often necessary for those with severe autoimmune-driven motility failure.
3. Vagal Toning
Since the Vagus Nerve is the "master switch" for the MMC, stimulating it is essential. Cold water immersion (cold showers), deep diaphragmatic breathing, and even singing or humming can stimulate the Vagus Nerve and shift the body into the parasympathetic state required for the "janitor" to start working.
4. Stress Decoupling
You cannot heal the gut in a state of high anxiety. Integrating "non-negotiable" periods of nervous system regulation into your day is as important as any supplement. This is not "self-care"; it is biological necessity.
5. Addressing the Autoimmune Component
If you suspect post-infectious SIBO, getting tested for anti-CdtB and anti-Vinculin antibodies (the IBS-Smart test) is crucial. If these antibodies are present, it confirms that your MMC failure is autoimmune. This knowledge changes the treatment strategy from "killing bacteria" to "long-term motility management."
---
Summary: Key Takeaways
The Migrating Motor Complex is the most under-appreciated mechanism in human health. It is the biological barrier that prevents the small intestine from becoming a graveyard of fermented waste and pathogenic bacteria.
- —The MMC is an inter-digestive event. It only works when you are NOT eating.
- —Phase III is the "Housekeeper Wave." It is the intense muscular sweep that clears the gut.
- —Interstitial Cells of Cajal (ICCs) are the pacemakers. Damage to these cells (often via food poisoning) is the leading cause of chronic gut issues.
- —Snacking is the enemy. Constant eating prevents the MMC from ever starting.
- —The UK "IBS" epidemic is largely SIBO. Most cases are driven by a mechanical failure of the MMC, not a lack of fibre or "stress" in the traditional sense.
- —Recovery requires a shift in focus. Stop trying to "kill" the bacteria and start trying to "move" the gut.
At INNERSTANDING, we believe that true health comes from aligning with our biological rhythms, not suppressing symptoms with chemicals. The MMC is a rhythm that modern life has tried to silence. It is time we started listening to it. The "Biological Janitor" is ready to work; we just need to give it the time, the space, and the cellular support it needs to clean house.
This article is provided for informational and educational purposes only. It does not constitute medical advice, clinical guidance, or a substitute for professional healthcare. Information reflects cited research at time of publication. Always consult a qualified healthcare professional before acting on any health information.
RESEARCH FOUNDATIONS
Biological Credibility Archive
Citations provided for educational reference. Verify via PubMed or institutional databases.
Medical Disclaimer
The information in this article is for educational purposes only and does not constitute medical advice, diagnosis, or treatment. Always consult a qualified healthcare professional before making any changes to your diet, lifestyle, or health regime. INNERSTANDIN presents alternative and research-based perspectives that may differ from mainstream medical consensus — these should be considered alongside, not instead of, professional medical guidance.
Read Full DisclaimerReady to learn more?
Continue your journey through our classified biological research.
DISCUSSION ROOM
Members of THE COLLECTIVE discussing "The Migrating Motor Complex: The Biological Janitor of the Gut"
SILENT CHANNEL
Be the first to discuss this article. Your insight could help others understand these biological concepts deeper.
THE ARSENAL
Based on SIBO & Small Intestine Health — products curated by our research team for educational relevance and biological support.

Magnesium Blend – The Most Important Mineral

Clean Slate – Detoxes thousands of chemicals,heavy metals, pesticides, allergens, mold spores and fungus

Vegan Essential Amino Acids – Plant-Powered Protein Building
INNERSTANDING may earn a commission on purchases made through these links. All products are selected based on rigorous educational relevance to our biological research.
RABBIT HOLE
Follow the biological thread deeper