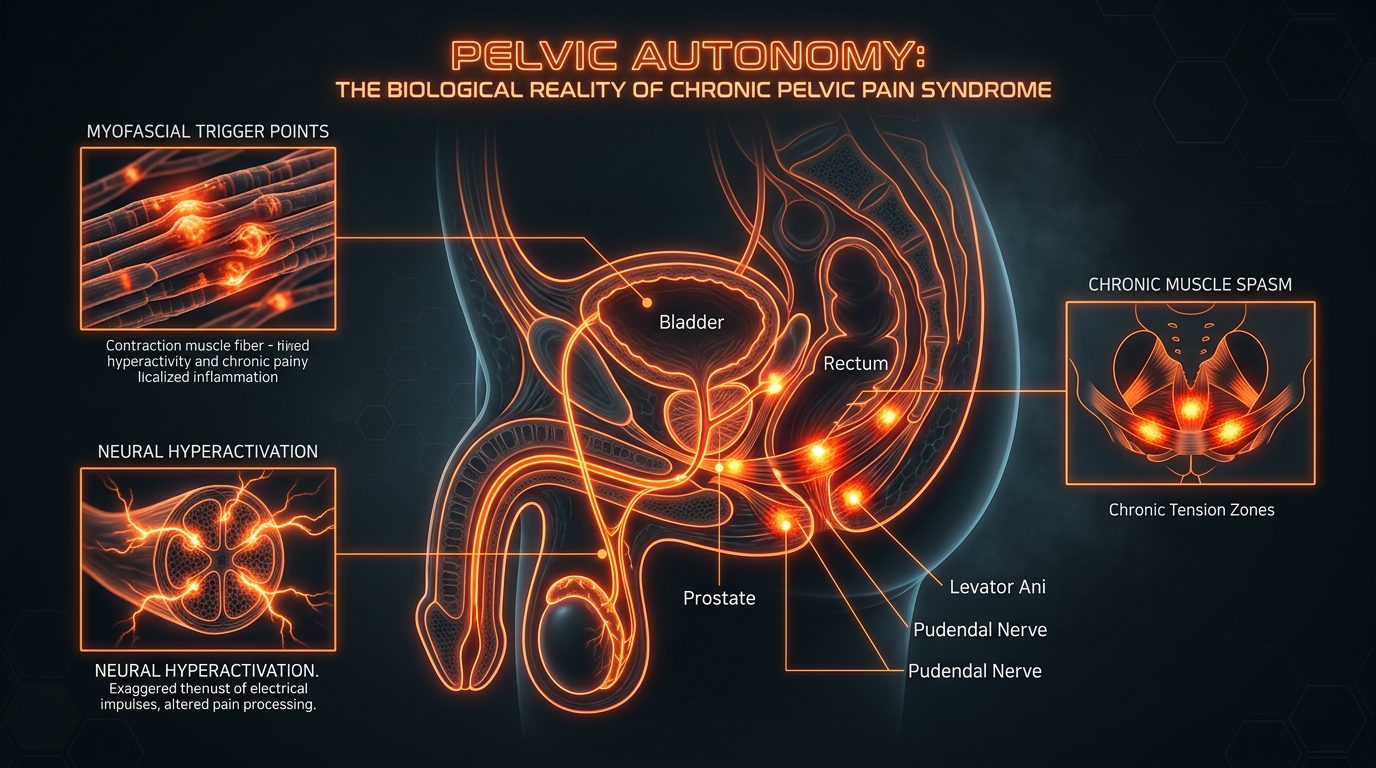
Pelvic Autonomy: The Biological Reality of Chronic Pelvic Pain Syndrome
Chronic pelvic pain is frequently misdiagnosed as an infection when it is actually a neuromuscular and fascial dysfunction. We explore the biological triggers that lead to the 'tension-pain' cycle in the pelvic bowl.
Overview
The human pelvis is not merely a structural basin for the lower abdominal organs; it is a sophisticated, highly reactive neurological epicentre. Yet, for millions of individuals globally—and particularly within the United Kingdom—the pelvis has become a site of unexplained, chronic torment. We are currently witnessing a silent epidemic of Chronic Pelvic Pain Syndrome (CPPS), a condition that is frequently and erroneously reduced to a simple "infection" by the mainstream medical establishment. This diagnostic myopia has led to a catastrophic reliance on repeat antibiotic prescriptions for non-existent bacterial pathogens, while the true biological culprit—a complex interplay of neuromuscular dysfunction and fascial constriction—remains unaddressed.
To understand Pelvic Autonomy, one must first accept that the pelvic floor is an emotional barometer. It is the only skeletal muscle group in the body that functions both voluntarily and involuntarily, reacting instantaneously to psychological stress, physical trauma, and postural habits. When this system enters a state of chronic hypertonicity, the "tension-pain cycle" begins. This is not a "headcase" disease, nor is it a bacterial invasion; it is a biological "short circuit" where the muscles of the pelvic bowl have forgotten how to relax.
In this exhaustive exploration, we move beyond the superficial urological narratives. We examine the fascia, the pudendal nerve, and the cellular mitochondrial stress that defines the CPPS experience. We seek to reclaim the biological autonomy of the patient by exposing the mechanisms that keep the body trapped in a state of perceived emergency.
In the UK, it is estimated that up to 15% of men will experience symptoms of "prostatitis" in their lifetime, yet clinical studies show that over 90% of these cases are non-bacterial and do not respond to antibiotics.
##
The Biology — How It Works
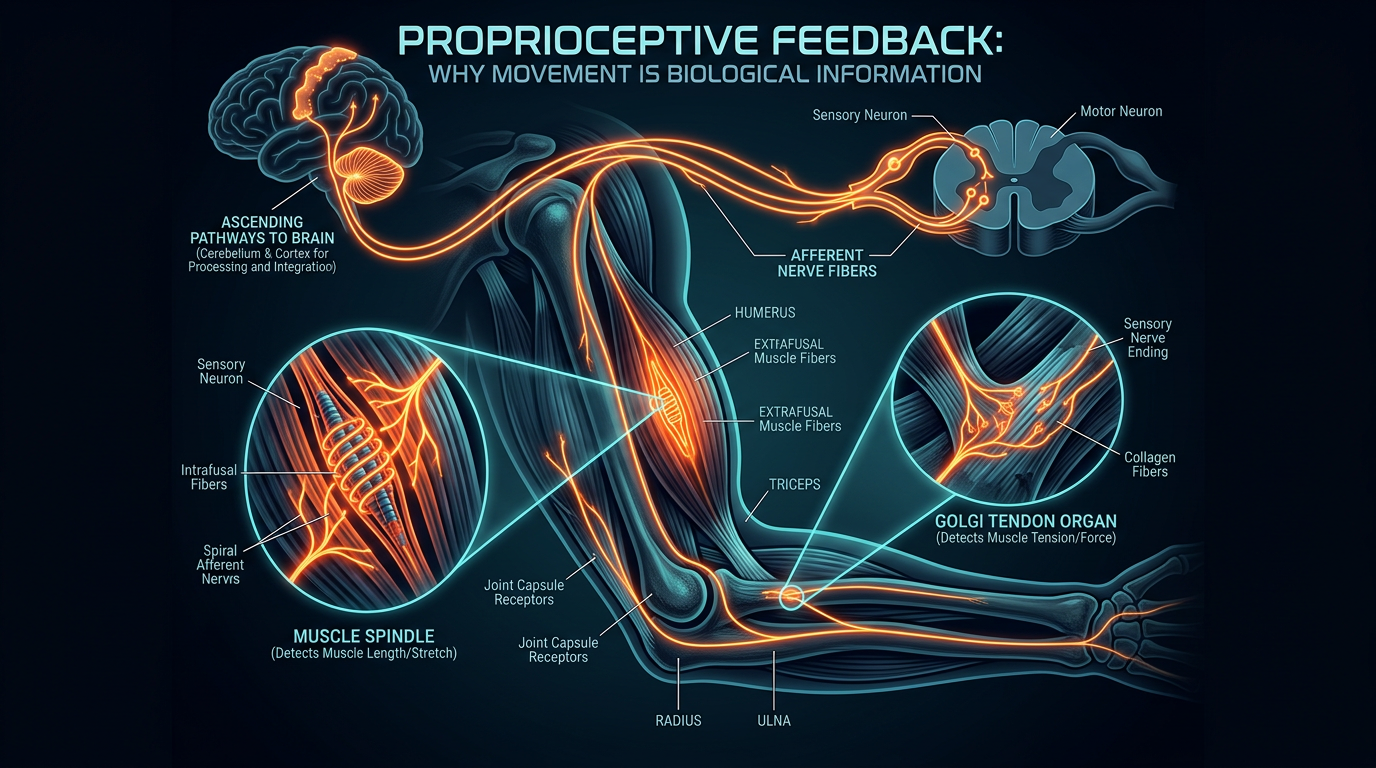
The pelvic floor is a complex "hammock" of muscles, including the *levator ani* (composed of the puborectalis, pubococcygeus, and iliococcygeus) and the *coccygeus*. These muscles do more than just support the bladder and bowels; they are intricately involved in core stability, sexual function, and intra-abdominal pressure regulation.
The Guarding Reflex
The biological root of CPPS often lies in what researchers term the "Guarding Reflex." When an animal perceives a threat, it instinctively tucks its tail and tightens its pelvic floor. This is a primitive, survival-based mechanism designed to protect the vulnerable soft tissues of the urogenital area. In modern humans, this threat is rarely a predator. Instead, it is the chronic "low-level" threat of workplace stress, postural collapse, or emotional repression. Over time, this temporary guarding becomes a permanent muscular habit.
Neuromuscular Dysregulation
When the pelvic muscles remain in a state of semi-contraction (hypertonicity) for months or years, the nervous system begins to recalibrate what it considers "normal." The Autonomic Nervous System (ANS), specifically the sympathetic branch (fight-or-flight), takes dominance over the parasympathetic branch (rest-and-digest). This creates a feedback loop: the brain senses tension in the pelvis and interprets it as a sign of danger, which in turn triggers more tension to "protect" the area.
The Fascial Web
Fascia is the connective tissue that wraps around every muscle fibre, nerve, and organ. In a healthy state, fascia is fluid and allows muscles to slide past one another effortlessly. In the CPPS patient, the fascia becomes "bound down" or "densified." This is a biological response to chronic tension. The fascia thickens and loses its elasticity, effectively encasing the pelvic nerves in a "suit of armour" that is several sizes too small. This fascial constriction is often what patients describe as a "golf ball" sensation in the perineum or a crushing weight in the pelvis.
##
Mechanisms at the Cellular Level
To truly understand why CPPS is so difficult to treat with traditional medicine, we must zoom in on the cellular landscape of the pelvic muscle fibres.
The Ischaemic-Pain Cycle
When a muscle is chronically contracted, it compresses the small capillaries that supply it with oxygen and nutrients. This leads to local ischaemia—a lack of blood flow. Without adequate oxygen, the mitochondria within the muscle cells cannot produce ATP (adenosine triphosphate) efficiently. ATP is required not just for muscle contraction, but also for muscle *relaxation*.
Without sufficient ATP, the "calcium pumps" in the muscle cells fail, leaving calcium trapped within the sarcomere. This prevents the muscle fibres from detaching, leading to a permanent state of contraction known as a "trigger point."
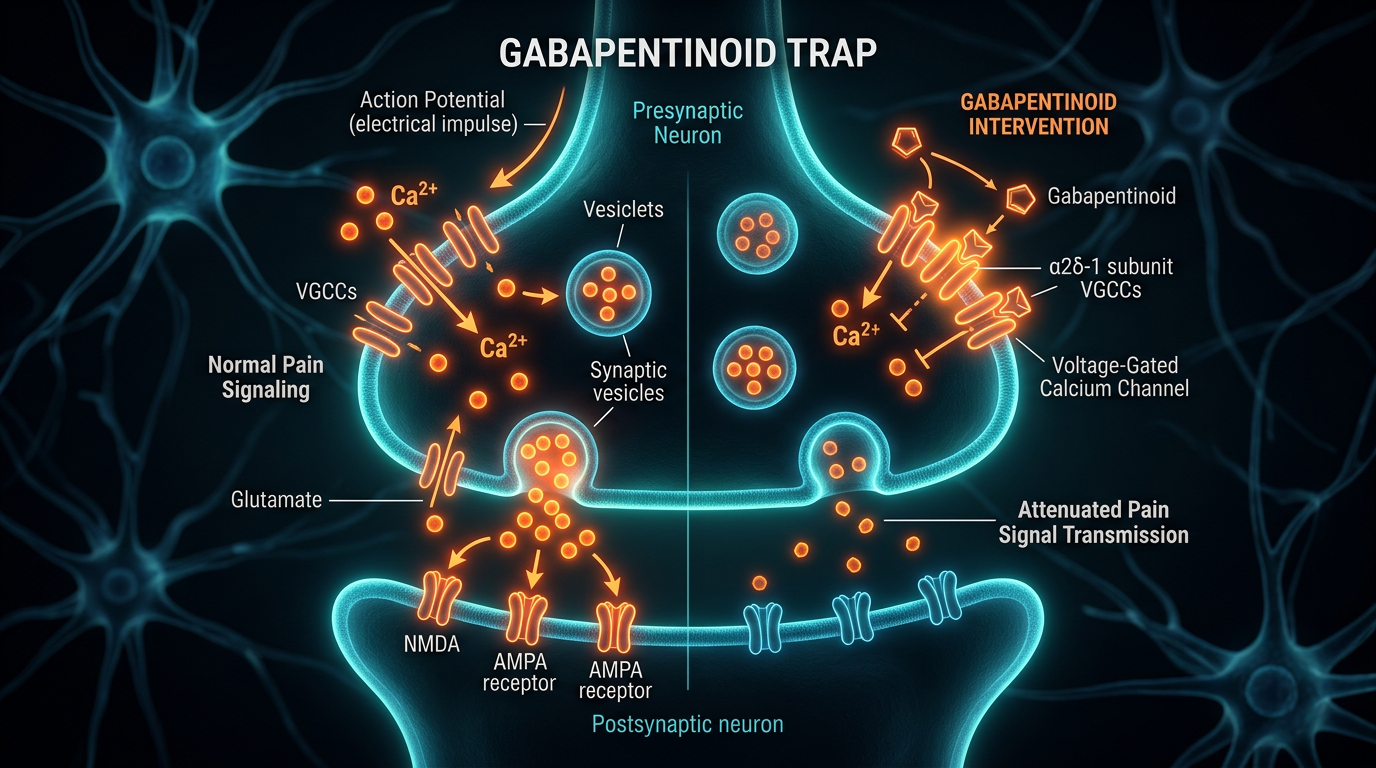
Lactic Acid and Metabolite Accumulation
Because the blood flow is restricted, the waste products of cellular metabolism—such as lactic acid, potassium ions, and substance P—cannot be washed away. These metabolites build up in the interstitial fluid of the pelvic bowl, lowering the local pH. This acidic environment irritates the nociceptors (pain-sensing nerves), causing them to fire more frequently. The brain receives a constant stream of "danger" signals, which it interprets as burning, stabbing, or aching pain.
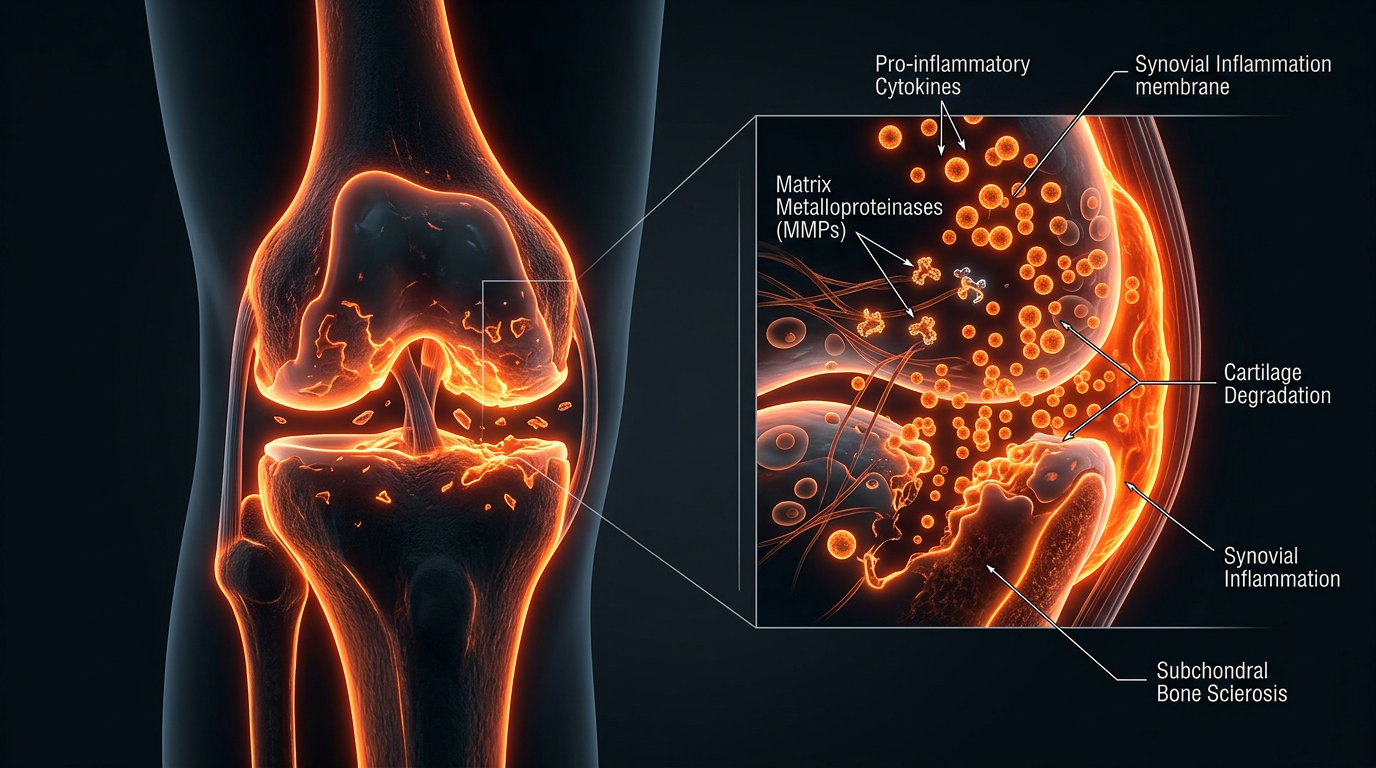
Mast Cell Activation
Recent biological research has identified an increased concentration of activated mast cells in the pelvic tissues of CPPS sufferers. Mast cells are part of the immune system and release histamine and pro-inflammatory cytokines when triggered. In CPPS, these cells appear to be triggered by the nervous system itself (neurogenic inflammation). This creates a "chemical soup" of inflammation that persists even in the absence of any bacteria or virus.
##
Environmental Threats and Biological Disruptors
The modern environment is fundamentally "anti-pelvic." Our biology evolved for movement, squatting, and varied physical exertion, yet we inhabit a world that demands stasis.
The Sedentary Siege
The act of sitting for 8–10 hours a day is a primary biological disruptor. When we sit on a standard chair, the pelvis is often tilted posteriorly, and the weight of the entire upper body is concentrated on the pelvic floor. This position creates chronic "mechanical ischaemia." Furthermore, the hip flexors (psoas) become shortened and tight, which pulls on the pelvic attachments, forcing the pelvic floor to work harder to maintain balance.
The "Computer Posture" and the Diaphragm
There is a direct biological link between the respiratory diaphragm and the pelvic diaphragm. They should move in tandem: as you inhale, both should drop; as you exhale, both should rise. However, most modern workers engage in "chest breathing" due to stress and slumped posture. This disconnects the pelvic floor from its natural rhythmic movement, causing it to become stagnant and rigid.
Chemical Irritants and the Bladder-Brain Axis
The pelvic floor is highly sensitive to the state of the bladder. Dietary irritants common in the UK—high-caffeine tea/coffee, artificial sweeteners, and alcohol—can irritate the bladder lining (the urothelium). An irritated bladder sends urgent signals to the brain, which responds by tensing the pelvic muscles to "hold" or "guard." Over time, the brain can no longer distinguish between a full bladder, an irritated bladder, and a tight pelvic muscle.
Psychosocial Stress: The Invisible Trigger
We must acknowledge the role of the amygdala. In individuals with a history of anxiety or trauma, the pelvic floor acts as a "physical container" for unexpressed emotion. This is not "all in the head"; it is a tangible biological reality where the limbic system communicates directly with the pelvic nerves. The "stiff upper lip" culture often prevents the release of this tension, leading to a physiological "locking" of the pelvic bowl.
##
The Cascade: From Exposure to Disease
The progression into full-blown CPPS is rarely a single event. It is a biological cascade of cascading failures.
Stage 1: The Initial Trigger
This could be a minor urinary tract infection, a period of extreme stress, a sports injury, or even a surgical procedure. The body responds with a "protective guarding" of the pelvis.
Stage 2: Failed Resolution
In a healthy system, once the threat (the infection or stress) passes, the muscles should return to their baseline length. In the CPPS-prone individual, the nervous system remains in a "high alert" state. The guarding persists.
Stage 3: Central Sensitisation
This is the "tipping point." After months of constant pain signals, the dorsal horn of the spinal cord and the brain itself undergo neuroplastic changes. The nervous system becomes hypersensitive. Light touch or normal bladder filling is now interpreted by the brain as intense pain. This is known as "wind-up" or central sensitisation. At this stage, the pain is no longer just in the muscles; it is "hardwired" into the central nervous system.
Stage 4: Systemic Manifestation
The chronic pain begins to affect other systems. The patient develops "IBS-like" symptoms as the pelvic tension affects bowel motility. Sleep is disrupted, leading to lower pain thresholds. The patient becomes hyper-vigilant, constantly "scanning" their pelvis for sensations, which further reinforces the neural pathways of pain.
Research indicates that 50% of men with CPPS also suffer from medically unexplained symptoms in other parts of the body, suggesting a systemic failure of the Autonomic Nervous System's "rest" function.
##
What the Mainstream Narrative Omits
The current medical model for pelvic pain is fundamentally broken because it is built on the Germ Theory rather than Systems Biology.
The Antibiotic Treadmill
When a patient presents with pelvic pain, the default urological response is to test for bacteria. If none are found (which is the case in 90-95% of patients), they are often prescribed antibiotics "just in case" or for their supposed anti-inflammatory effects. This is a biological disaster. Repeated cycles of Ciprofloxacin or Doxycycline decimate the gut and vaginal/prostatic microbiome, leading to systemic inflammation and, ironically, increased sensitivity to pain.
The "Organ-Centric" Fallacy
Urologists are trained to look at the prostate, the bladder, and the kidneys. They are rarely trained to look at the *muscles* and *fascia* that surround these organs. If the "parts" look healthy on a scan or through a cystoscope, the patient is told nothing is wrong. This dismisses the fact that the "housing" of the organs—the pelvic floor—is in a state of crisis.
The Failure of "Kegels"
For decades, the standard advice for any pelvic issue was "do more Kegels" (pelvic floor contractions). For a CPPS patient, this is akin to telling someone with a clenched fist to squeeze their hand harder. CPPS is a disorder of too much tone, not too little. Standard Kegel exercises exacerbate the ischaemia and reinforce the pain cycle. The mainstream narrative has failed to differentiate between the "weak" pelvis and the "short/tight" pelvis.
##
The UK Context
In the United Kingdom, the management of CPPS is particularly fraught with systemic hurdles. The National Health Service (NHS), while noble in intent, is ill-equipped for the "slow medicine" required to unravel chronic neuromuscular conditions.
The Postcode Lottery of Care
Access to specialised Pelvic Health Physiotherapists—the true "front line" for CPPS recovery—is notoriously inconsistent across the UK. While London and major hubs may have dedicated clinics, patients in rural areas or smaller trusts may wait years for a referral, or be told that "men don't have pelvic floors," a biological absurdity that still persists in some clinical circles.
The NHS spends millions of pounds annually on unnecessary urological investigations (cystoscopies, prostate biopsies) for CPPS patients, while specialized pelvic physiotherapy remains underfunded and under-referred.
The "Stiff Upper Lip" and Male Silence
British culture, particularly among men, often discourages the discussion of "down there" pain. This leads to a significant delay in seeking help. When help is finally sought, the psychological toll of being dismissed or misdiagnosed often leads to severe depression and anxiety, which, as we have established, only serves to tighten the pelvic floor further.
The Impact of the UK Workplace
The UK has some of the longest sitting hours in Europe. The "commute-desk-couch" lifestyle is a primary driver of the physical component of CPPS. Without systemic changes in workplace ergonomics and "movement culture," the biological triggers for pelvic dysfunction will remain ubiquitous.
##
Protective Measures and Recovery Protocols
Recovery from CPPS is not about "killing a bug"; it is about re-educating a system. It requires a multi-modal approach that addresses the biology, the neurology, and the psychology of the pelvic bowl.
1. Paradoxical Relaxation
Developed by Dr. David Wise and Dr. Rodney Anderson at Stanford University, this technique is the gold standard for CPPS recovery. It involves "accepting" the tension rather than fighting it. By bringing conscious, non-judgmental awareness to the pelvic floor, the patient can slowly inhibit the "Guarding Reflex." This is not simple relaxation; it is a neurological "reset."
2. Myofascial Release (Internal and External)
The "knots" (trigger points) in the pelvic floor must be physically deactivated. This is often done by a specialised physiotherapist using internal manual therapy (rectally or vaginally). By applying sustained pressure to these points, the therapist can manually break the ischaemic cycle, allowing fresh, oxygenated blood to return to the tissue and the "calcium pumps" to reset.
3. The "Reverse Kegel" and Diaphragmatic Breathing
Patients must learn to "drop" the pelvic floor. This is achieved through diaphragmatic breathing.
- —The Practice: Inhale deeply into the belly, imagining the pelvic floor expanding downwards like a blooming flower.
- —The Biological Goal: This provides a gentle, internal stretch to the levator ani and recalibrates the relationship between the two diaphragms.
4. Neuroplastic Reframing
Because the brain has become "sensitised" to pelvic signals, the patient must engage in "Pain Reprocessing Therapy." This involves teaching the brain that the sensations in the pelvis—while uncomfortable—are not dangerous. When the brain stops interpreting the tension as a threat, the sympathetic nervous system "stands down," allowing the muscles to eventually follow suit.
5. Movement as Medicine
Static stretching is not enough. The pelvis needs dynamic movement to maintain fascial health. Activities like Yoga (specifically Yin Yoga), swimming, and "unstructured" walking help to break the sedentary patterns that lock the pelvis in place. Crucially, the focus should be on "opening" the hips and "lengthening" the psoas.
6. Nutritional Support for the Nervous System
To support the healing of the nerves and the reduction of mast cell activation, certain biological supports are recommended:
- —Magnesium Glycinate: To aid muscle relaxation and ATP production.
- —Quercetin: A natural mast-cell stabiliser that has shown significant efficacy in CPPS clinical trials.
- —Omega-3 Fatty Acids: To reduce systemic neuro-inflammation.
- —Avoiding Bladder Triggers: Temporary elimination of spicy foods, caffeine, and concentrated alcohol to lower the "input" to the bladder-brain axis.
##
Summary: Key Takeaways
The biological reality of Chronic Pelvic Pain Syndrome is far removed from the "prostatitis" myths of the 20th century. It is a systemic, neuromuscular, and fascial crisis that requires a total paradigm shift in treatment.
- —CPPS is Neuromuscular, Not Microbial: In 95% of cases, there is no infection. The pain is caused by hypertonic muscles and "locked" fascia.
- —The Guarding Reflex is Central: The pelvis reacts to stress by tightening. Chronic stress leads to chronic tightening, which creates a self-perpetuating pain cycle.
- —Cellular Ischaemia is the Root: Chronically contracted muscles starve themselves of oxygen, leading to trigger points and the accumulation of painful metabolites.
- —The NHS Model is Flawed: The reliance on antibiotics and "organ-only" urology fails CPPS patients. We need a "Systems Biology" approach that includes Pelvic Physiotherapy.
- —Recovery is a Process of "Unlearning": Healing requires physical release of the muscles, neurological desensitisation, and a fundamental change in how the patient inhabits their body.
The path to Pelvic Autonomy is one of reclaiming the body from the "protection" of the nervous system. It is a journey from a state of "perpetual emergency" back to a state of fluid, painless function. By understanding the biological reality of CPPS, we strip away the fear and the "mystery" of the condition, empowering the individual to begin the work of biological restoration. At INNERSTANDING, we advocate for this radical shift—away from the antibiotic treadmill and toward a deep, scientific understanding of the human pelvic bowl.
This article is provided for informational and educational purposes only. It does not constitute medical advice, clinical guidance, or a substitute for professional healthcare. Information reflects cited research at time of publication. Always consult a qualified healthcare professional before acting on any health information.
RESEARCH FOUNDATIONS
Biological Credibility Archive
Citations provided for educational reference. Verify via PubMed or institutional databases.
Medical Disclaimer
The information in this article is for educational purposes only and does not constitute medical advice, diagnosis, or treatment. Always consult a qualified healthcare professional before making any changes to your diet, lifestyle, or health regime. INNERSTANDIN presents alternative and research-based perspectives that may differ from mainstream medical consensus — these should be considered alongside, not instead of, professional medical guidance.
Read Full DisclaimerReady to learn more?
Continue your journey through our classified biological research.
DISCUSSION ROOM
Members of THE COLLECTIVE discussing "Pelvic Autonomy: The Biological Reality of Chronic Pelvic Pain Syndrome"
SILENT CHANNEL
Be the first to discuss this article. Your insight could help others understand these biological concepts deeper.
RABBIT HOLE
Follow the biological thread deeper