Pelvic Floor Avulsion: The Biomechanics of Birth Injuries
Forceful delivery techniques can cause pelvic floor avulsion, where the muscle is torn from the bone. This biological trauma is often overlooked in UK postnatal care, leading to chronic dysfunction.
# Pelvic Floor Avulsion: The Biomechanics of Birth Injuries
Overview
In the landscape of modern obstetrics, a silent and structurally devastating epidemic is unfolding. While the medical establishment focuses heavily on neonatal outcomes and immediate maternal survival, a profound biological failure is being systematically overlooked: Pelvic Floor Avulsion. This is not a mere "weakness" or a "laxity" that can be rectified with routine exercises; it is a traumatic detachment of the muscle from the bone—a structural catastrophe that alters the female biomechanical blueprint forever.
For decades, women suffering from post-delivery incontinence, pelvic organ prolapse (POP), and chronic pelvic pain have been told that these are the "natural" consequences of motherhood. At INNERSTANDING, we reject this reductionist narrative. Pelvic floor avulsion—specifically the avulsion of the Levator Ani Muscle (LAM)—represents a mechanical failure of the biological scaffolding, often induced by aggressive iatrogenic interventions and a fundamental misunderstanding of the viscoelastic limits of human tissue.
Recent studies indicate that up to 15-30% of women who deliver vaginally sustain some form of levator ani injury, with the incidence skyrocketing in cases involving forceps. Despite this, the standard UK postnatal check-up involves no specialized imaging or diagnostic protocols to identify these injuries. We are witnessing a systemic failure to diagnose a "broken" pelvic architecture, leaving millions of women to navigate a life of functional disability under the guise of "normal" recovery.
Fact: A levator ani avulsion increases the risk of developing significant pelvic organ prolapse by three to fifteen times, yet it remains undiagnosed in over 90% of clinical cases.
The Biology — How It Works
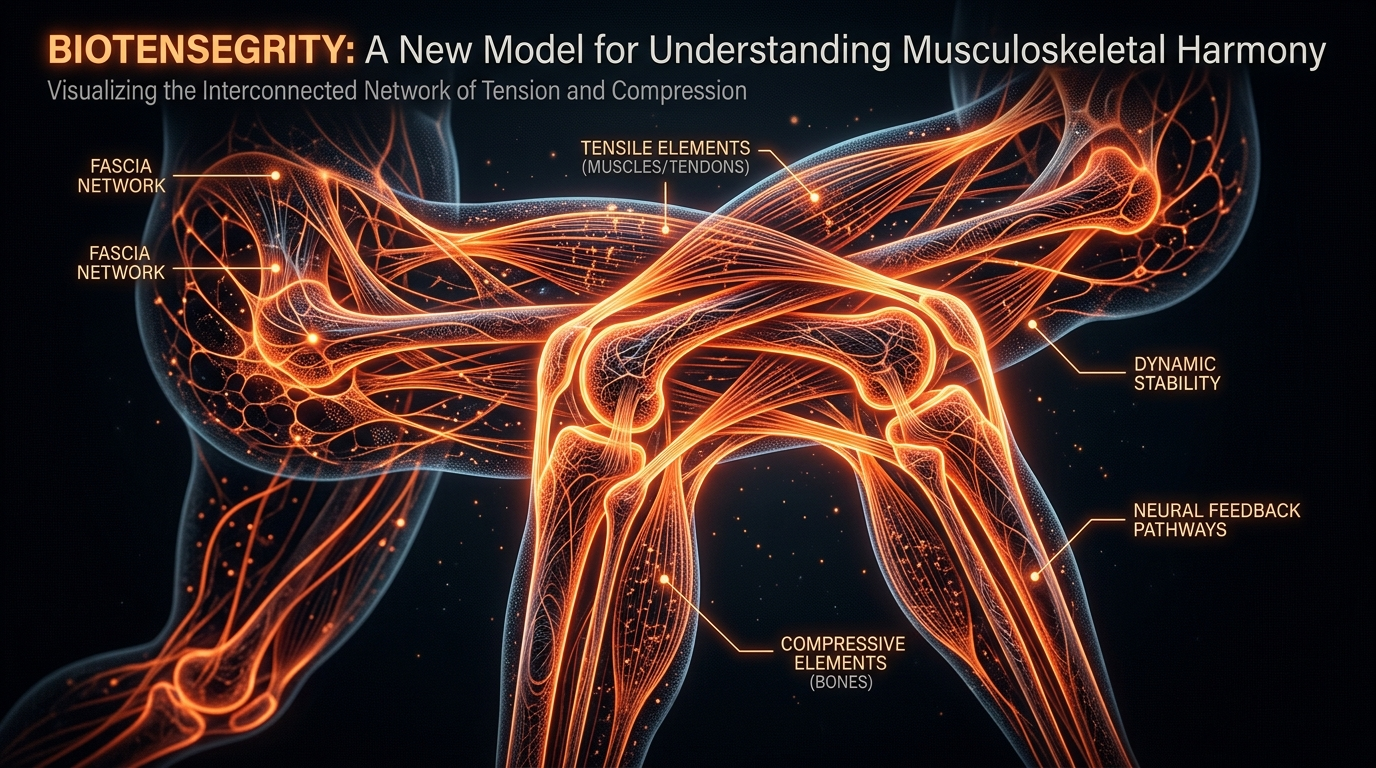
To understand avulsion, one must first understand the architecture of the Levator Ani Muscle (LAM) complex. The LAM is not a single muscle but a sophisticated, multi-layered "hammock" consisting of the pubococcygeus, puborectalis, and iliococcygeus. Together, they maintain the "levator hiatus"—the gateway through which the urethra, vagina, and rectum pass.
The Anchor Point: The Pubic Bone
The most critical structural point is the attachment of the pubovisceral muscle to the posterior surface of the inferior pubic ramus. This is the "anchor." In a healthy state, this attachment provides the tension necessary to keep the pelvic floor closed and the organs supported against gravity and intra-abdominal pressure.
The Biomechanics of Crowning
During the second stage of labour, the fetal head must pass through the levator hiatus. For this to occur, the levator ani must undergo extreme stretching. Biomechanical modelling suggests that the pubovisceral muscle must stretch by a factor of up to 3.2 to 1.
In biological terms, this is an extraordinary demand. Most skeletal muscles reach their "point of failure" or permanent deformation long before they reach a 300% stretch ratio. The female pelvic floor is biologically adapted for this, but it operates on a razor-thin margin of safety. When that margin is exceeded—due to the speed of the birth, the size of the fetal head, or the use of metal instruments—the muscle does not simply stretch; it reaches its ultimate tensile strength and fails.
Avulsion vs. Tearing
It is imperative to distinguish between a "perineal tear" and an "avulsion."
- —Perineal Tears: Occur in the soft tissues and skin of the perineum (1st to 4th degree). These are usually visible and are sutured immediately after birth.
- —Avulsion: This is an internal, "hidden" injury. The muscle is literally ripped off the pubic bone. It is a disinsertion. Because the skin remains intact, the injury is invisible to the naked eye.
Mechanisms at the Cellular Level
At the microscopic scale, pelvic floor avulsion is a collapse of the Extracellular Matrix (ECM) and the failure of the Enthesis—the specialized tissue zone where tendon or muscle attaches to bone.
The Failure of the Enthesis
The enthesis is designed to dissipate stress between two vastly different materials: the compliant, elastic muscle and the rigid, mineralised bone. This zone is rich in Type I Collagen and fibrocartilage. During an avulsion event, the mechanical load exceeds the cohesive strength of the collagen fibres. The cellular "glue" (proteoglycans and integrins) that binds the muscle fibres to the periosteum of the bone snaps.
Ischaemia-Reperfusion Injury
While the mechanical tear is the primary event, the cellular damage is compounded by hypoxia. During a prolonged second stage of labour, the levator ani is subjected to intense compression by the fetal head. This creates a state of ischaemia (lack of blood flow). When the pressure is finally released (the birth), a surge of oxygen returns to the tissues, triggering the production of Reactive Oxygen Species (ROS). This oxidative stress damages the mitochondria within the remaining muscle cells, hindering their ability to regenerate or compensate for the lost attachment.
The Role of Elastin and Matrix Metalloproteinases (MMPs)
The ability of the pelvic floor to recover from the massive stretch depends on the balance of Elastin and the activity of enzymes called Matrix Metalloproteinases (MMPs). MMPs are responsible for remodelling the tissue after trauma. In women with certain genetic predispositions or nutritional deficiencies, an overactive MMP response can lead to the excessive breakdown of the ECM, turning a "stretch" into a permanent "sag" or total structural failure.
Statistic: Women with lower levels of total pelvic collagen or altered collagen ratios (Type III vs Type I) are significantly more susceptible to avulsion and subsequent prolapse.
Environmental Threats and Biological Disruptors
In the context of birth trauma, "environmental threats" are not merely external toxins, but the obstetric environment and the interventions that disrupt the natural biological rhythm of birth.
The Iatrogenic Factor: Forceps
The single greatest environmental threat to the integrity of the levator ani is the obstetric forceps. Forceps are rigid steel blades inserted into the birth canal. They occupy space, further distending the already maximally stretched levator hiatus. When "traction" is applied, the force is often sudden and exceeds the viscoelastic adaptation time of the muscle.
- —Forceps delivery increases the risk of levator ani avulsion by 300% to 400% compared to a spontaneous vaginal birth.
- —The use of forceps essentially "bypass" the body's protective mechanisms, forcing a diameter through a space that has not yet biologically prepared for it.
Synthetic Oxytocin (Syntocinon/Pitocin)
The use of synthetic oxytocin to "augment" labour creates uterine contractions that are often more frequent and forceful than natural contractions. This reduces the "rest periods" between contractions, depriving the pelvic floor muscles of the time needed to recover blood flow and slowly distend. This "hyper-stimulation" puts the levator ani under a relentless mechanical load, making cellular failure far more likely.
Maternal Positioning: The Lithotomy Position
The "standard" hospital position—lying on the back with legs in stirrups (lithotomy)—is a biological disruptor. This position narrows the pelvic outlet and forces the fetal head to be pushed "uphill" against the levator ani. In contrast, upright or squatting positions allow the pelvis to expand and the muscles to distend more symmetrically, reducing the concentrated stress on the pubic attachments.
The Cascade: From Exposure to Disease
The occurrence of an avulsion is the "Point Zero" of a long-term pathological cascade. Because the pelvic floor is a functional unit, the failure of one part (the LAM) triggers a domino effect across the entire system.
Phase 1: Loss of the "Levator Gate"
When the pubovisceral muscle is detached from the bone, the levator hiatus (the hole in the pelvic floor) widens permanently. This is known as "ballooning." The muscle can no longer "gate" the pelvic opening.
Phase 2: Pathological Load Shifting
With the primary muscular support gone, the burden of holding the pelvic organs (bladder, uterus, bowel) in place shifts entirely to the fascia and ligaments (such as the uterosacral ligaments). Unlike muscle, fascia is not contractile. Under the constant pressure of gravity and daily movement, these ligaments slowly stretch and thin out.
Phase 3: Pelvic Organ Prolapse (POP)
As the ligaments fail, the organs begin to descend into the widened levator hiatus.
- —Cystocele: The bladder falls into the vagina.
- —Uterine Prolapse: The uterus descends.
- —Rectocele: The rectum bulges forward.
Phase 4: Secondary Neuropathies
The structural sag often leads to the stretching of the Pudendal Nerve. This can cause a secondary layer of dysfunction: fecal incontinence, urinary urgency, and "pelvic floor desensitisation," where the woman loses the ability to "feel" or engage her pelvic muscles at all.
What the Mainstream Narrative Omits
The mainstream medical narrative regarding postnatal recovery is fraught with omissions, half-truths, and what many researchers now term "medical gaslighting."
The "Just Do Your Kegels" Fallacy
The most pervasive myth told to postpartum women is that pelvic floor exercises (Kegels) will fix their symptoms. Biomechanical Reality: You cannot strengthen a muscle that is no longer attached to the bone. If a woman has a full avulsion, performing Kegels is like trying to close a door that has been ripped off its hinges. The "motor" is running, but the "gears" are not engaged. Promoting Kegels as a cure-all for avulsion is not only scientifically inaccurate; it is psychologically damaging to the women who see no improvement.
The Invisible Injury
Standard postnatal care in the UK relies on a visual inspection of the perineum. If the skin is intact or the stitches have healed, the woman is told she is "fine." However, avulsion is internal. It cannot be seen with the naked eye. It can only be diagnosed via:
- —3D/4D Transperineal Ultrasound
- —MRI of the Pelvic Floor
- —Specialised Digital Palpation (by an expert pelvic physiotherapist)
By failing to screen for avulsion, the medical system ignores the structural cause of the patient's suffering, often attributing her symptoms to "postnatal depression" or "the new normal of being a mother."
The Economic Silence
There is a profound economic incentive to keep the "avulsion epidemic" quiet. Routine 4D ultrasound screening for every woman who has a forceps delivery would cost the NHS millions. Furthermore, acknowledging the high rate of permanent injury associated with forceps might lead to a surge in litigation and a demand for more expensive elective Caesarean sections.
The UK Context
The situation in the United Kingdom is particularly dire due to the systemic pressures on the National Health Service (NHS).
The "Normal Birth" Obsession
For years, the UK's maternity strategy was dominated by the "normal birth" ideology, which sought to minimise Caesarean sections at all costs. While avoiding unnecessary surgery is a noble goal, this ideology often led to "instrumental" vaginal deliveries (forceps/ventouse) being pushed as a "safer" alternative to a C-section. We now know that for the mother’s long-term pelvic health, a planned C-section is significantly safer than a traumatic forceps delivery.
The Postcode Lottery of Care
Access to a Pelvic Health Physiotherapist—the only professionals truly trained to identify these injuries—is a "postcode lottery" in the UK. Many women are never referred, and those who are often face waitlists of 6 to 12 months. By the time they are seen, the window for early intervention and "neuroplastic" recovery has often closed.
The Lack of Diagnostic Infrastructure
Most UK maternity units do not have the 4D ultrasound equipment or the trained sonographers required to diagnose levator ani avulsion. Women are trapped in a cycle of "reassurance" by General Practitioners who lack the specialist training to understand pelvic biomechanics.
Callout: In the UK, it is estimated that 1 in 10 women will require surgery for pelvic organ prolapse in their lifetime. A significant portion of these surgeries could be avoided if birth injuries were diagnosed and managed correctly in the first six months postpartum.
Protective Measures and Recovery Protocols
While the damage of an avulsion is structural, there are pathways to protection and recovery that circumvent the "wait and see" approach of mainstream medicine.
Prevention: Antenatal and Intrapartum
- —Epi-No and Perineal Massage: While controversial, some evidence suggests that gradual mechanical stretching of the levator hiatus in the weeks before birth can increase tissue "compliance" and reduce the risk of failure.
- —Advocating for "Warm Compresses": During the second stage, warm compresses applied to the perineum by midwives can increase local blood flow and tissue elasticity.
- —Informed Consent for Forceps: Women must be informed of the specific risk of levator avulsion *before* forceps are used. If the risk is too high (e.g., a large baby and a mother over 35), a C-section should be discussed as a protective measure for the pelvic floor.
- —Spontaneous Pushing: Avoiding "purple pushing" (Valsalva manoeuvre) and instead allowing the body’s "fetal ejection reflex" to work can prevent the sudden, explosive forces that cause avulsion.
Diagnosis: The Gold Standard
If you have had an instrumental delivery or an exceptionally fast/traumatic birth, do not wait for symptoms to appear.
- —Demand a Referral: Request a referral to a Urogynaecologist or a Specialist Pelvic Health Physiotherapist.
- —Private Imaging: If the NHS refuses, a private 3D transperineal ultrasound is the most cost-effective way to visualise the levator ani attachments.
Recovery: Beyond Kegels
- —Pessary Therapy: If an avulsion is present, a "pessary" (a silicone device inserted into the vagina) can provide the structural support that the missing muscle cannot. This prevents the "cascade" of prolapse by taking the weight off the ligaments.
- —Neuromuscular Electrical Stimulation (NMES): For partially damaged muscles, NMES can help "re-wake" the neural pathways.
- —Surgical Re-attachment: In severe cases, surgical procedures to "bridge" the gap or use mesh/grafts to support the hiatus may be necessary. However, "native tissue" repair remains the goal.
- —Hyperbaric Oxygen Therapy (HBOT): To combat the ischaemia-reperfusion injury and promote cellular repair in the immediate postnatal period.
Summary: Key Takeaways
The biological reality of birth trauma is far more complex than the medical establishment admits. Pelvic Floor Avulsion is a hidden crisis that demands a total paradigm shift in how we view maternal health.
- —Avulsion is a structural failure: It is the physical detachment of the levator ani muscle from the pubic bone, not a simple muscle weakness.
- —Forceps are the primary risk factor: The biomechanical load imposed by forceps frequently exceeds the ultimate tensile strength of human tissue.
- —The "Kegel" narrative is insufficient: Strengthening exercises cannot fix a detached muscle; structural support (pessaries) or surgical intervention may be required.
- —The UK system is failing women: The lack of routine diagnostic imaging and the "normalisation" of pelvic dysfunction leaves women with permanent, undiagnosed injuries.
- —Early diagnosis is critical: Identifying an avulsion in the "fourth trimester" allows for protective measures that prevent the long-term cascade into pelvic organ prolapse.
We must stop treating the female pelvic floor as an infinitely stretchable resource. It is a finely tuned biomechanical system that, once broken, requires more than "reassurance" to fix. It requires the truth.
This article is provided for informational and educational purposes only. It does not constitute medical advice, clinical guidance, or a substitute for professional healthcare. Information reflects cited research at time of publication. Always consult a qualified healthcare professional before acting on any health information.
RESEARCH FOUNDATIONS
Biological Credibility Archive
Levator ani muscle avulsion occurs in approximately 10-15% of primiparous women following vaginal delivery, significantly increasing the risk of pelvic organ prolapse.
Biomechanical modeling reveals that the pubococcygeus muscle undergoes maximal strain during the second stage of labor, exceeding the tissue's elastic threshold in operative vaginal births.
Use of three-dimensional pelvic floor ultrasound allows for the precise diagnosis of puborectalis muscle detachment from the pubic bone, a hallmark of major birth trauma.
Maternal age and the use of forceps are identified as primary independent risk factors for the mechanical failure of pelvic floor muscle attachments during childbirth.
The pathophysiology of pelvic floor avulsion involves acute structural disruption of the levator ani, which leads to long-term functional impairment and pelvic floor dysfunction.
Citations provided for educational reference. Verify via PubMed or institutional databases.
Medical Disclaimer
The information in this article is for educational purposes only and does not constitute medical advice, diagnosis, or treatment. Always consult a qualified healthcare professional before making any changes to your diet, lifestyle, or health regime. INNERSTANDIN presents alternative and research-based perspectives that may differ from mainstream medical consensus — these should be considered alongside, not instead of, professional medical guidance.
Read Full DisclaimerReady to learn more?
Continue your journey through our classified biological research.
DISCUSSION ROOM
Members of THE COLLECTIVE discussing "Pelvic Floor Avulsion: The Biomechanics of Birth Injuries"
SILENT CHANNEL
Be the first to discuss this article. Your insight could help others understand these biological concepts deeper.
THE ARSENAL
Based on Birth Trauma & Perinatal Health — products curated by our research team for educational relevance and biological support.

Magnesium Blend – The Most Important Mineral

Clean Slate – Detoxes thousands of chemicals,heavy metals, pesticides, allergens, mold spores and fungus

Vegan Essential Amino Acids – Plant-Powered Protein Building
INNERSTANDING may earn a commission on purchases made through these links. All products are selected based on rigorous educational relevance to our biological research.
RABBIT HOLE
Follow the biological thread deeper