Phthalate-Induced Testicular Dysgenesis Syndrome
Synthetic plastics interfere with the anatomical development of the male reproductive system in utero. This investigation tracks the rising rates of structural reproductive anomalies in the UK.
Overview
The conceptual framework of Testicular Dysgenesis Syndrome (TDS), originally proposed by Skakkebaek et al. in *The Lancet* (2001), posits that cryptorchidism, hypospadias, impaired spermatogenesis, and testicular germ cell tumours (TGCT) are not isolated clinical entities, but rather a constellation of symptoms arising from a common developmental origin: the disruption of foetal testicular differentiation. At the heart of this developmental derailment lies the insidious role of phthalate esters—ubiquitous plasticisers found in the UK industrial and domestic landscape—which function as potent endocrine-disrupting chemicals (EDCs). For the INNERSTANDIN learner, it is critical to recognise that these compounds do not merely "mimic" hormones; they orchestrate a molecular assault on the masculinisation programming window (MPW), a critical gestational epoch where androgen signalling dictates the morphological trajectory of the male reproductive tract.
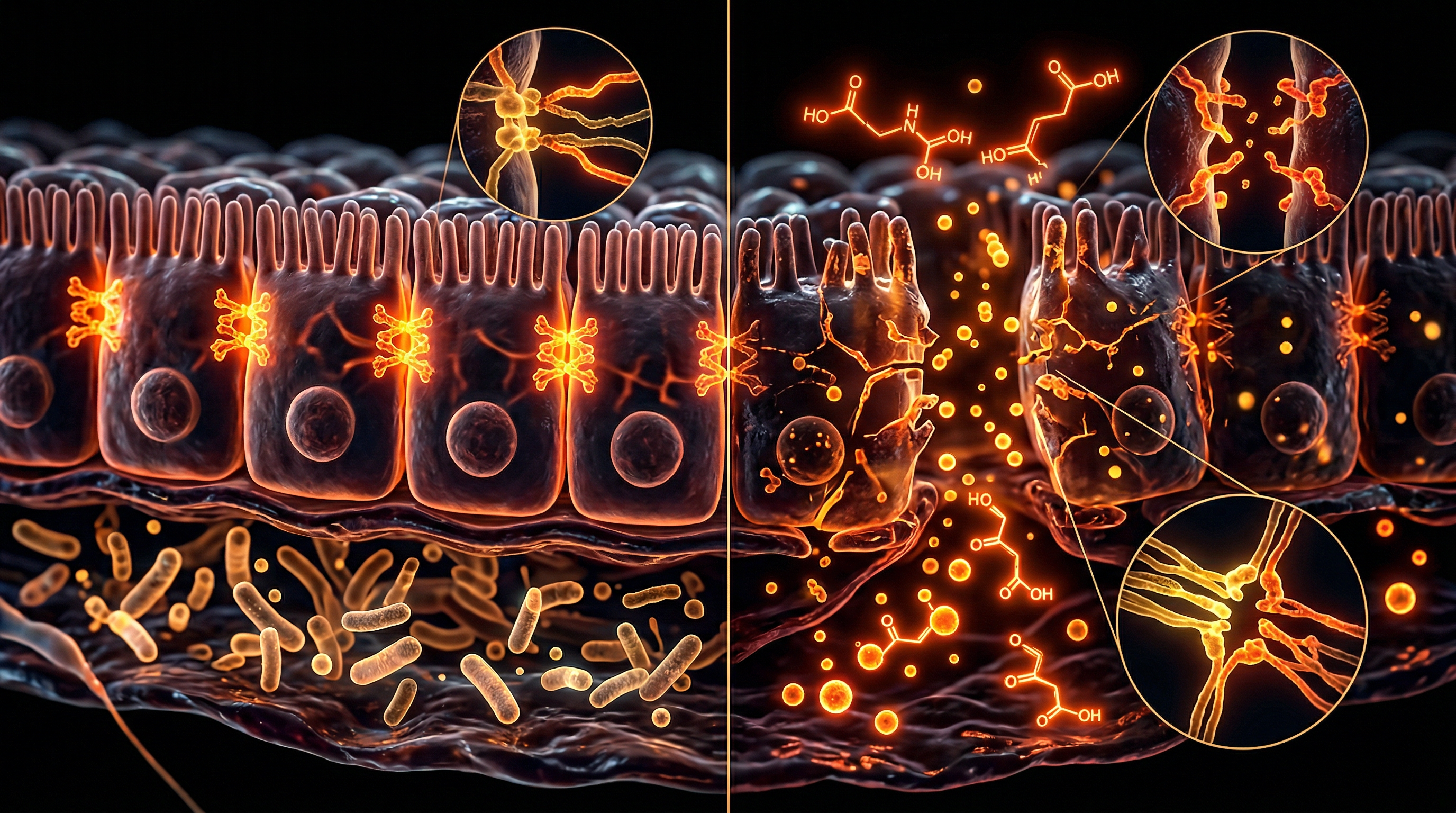
The biological mechanism of Phthalate-Induced TDS is characterised by the suppression of foetal Leydig cell (FLC) function. Peer-reviewed studies indexed in PubMed demonstrate that phthalate exposure—specifically to Di(2-ethylhexyl) phthalate (DEHP) and Dibutyl phthalate (DBP)—inhibits the expression of key steroidogenic enzymes, including CYP11A1 and CYP17A1, and the cholesterol transporter StAR (Steroidogenic Acute Regulatory protein). This suppression results in a profound reduction in intratesticular testosterone levels. Furthermore, phthalates interfere with the production of Insulin-like factor 3 (INSL3), a peptide hormone essential for the first phase of testicular descent. The anatomical fallout is a failure of the gubernaculum to properly develop, leading to cryptorchidism and subsequent thermogenic damage to the germinal epithelium.
INNERSTANDIN identifies this syndrome as a systemic failure of testicular architecture. When the foetal Sertoli cells are compromised during this window, their proliferative capacity is diminished, resulting in a reduced "Sertoli cell quota" which permanently limits sperm production capacity in adulthood. Moreover, the failure of gonocytes to differentiate into prespermatogonia creates a reservoir of primitive cells that remain susceptible to malignant transformation, providing the histopathological basis for testicular cancer later in life. In the UK context, where male reproductive health markers have shown a steady decline over the last five decades, the epidemiological link between phthalate burden and TDS signifies an urgent bio-security crisis. The disruption of the androgen-to-oestrogen ratio during organogenesis does not simply alter anatomy; it reconfigures the male biological potential at its most fundamental level. This is not a speculative risk but a documented shift in human ontogeny, where the chemical environment of the modern world overrides the genetic blueprint of male development.
The Biology — How It Works
The molecular aetiology of Phthalate-Induced Testicular Dysgenesis Syndrome (TDS) resides within the disruption of the fetal Masculinisation Programming Window (MPW)—a critical gestational epoch where androgen signalling dictates the morphological trajectory of the male reproductive tract. Unlike classic toxicants that induce direct cellular necrosis, phthalates, specifically high-molecular-weight esters such as Di(2-ethylhexyl) phthalate (DEHP) and Dibutyl phthalate (DBP), act as potent endocrine disruptors that recalibrate the steroidogenic capacity of fetal Leydig cells. This is not merely an observational correlation; it is a fundamental biochemical hijacking of the male reproductive blueprint.
Upon systemic absorption, these parent compounds are rapidly metabolised into bioactive monoesters, such as MEHP and MBP. Research conducted at institutions like the University of Edinburgh, and published in *The Lancet Diabetes & Endocrinology*, demonstrates that these metabolites penetrate the placental barrier to interfere directly with the expression of the Steroidogenic Acute Regulatory (StAR) protein and the CYP11A1 enzyme. This inhibition halts the rate-limiting step of steroidogenesis—the transport of cholesterol into the mitochondrial matrix—effectively throttling the biosynthesis of testosterone. This hypoandrogenic state occurs precisely when the fetal gubernaculum requires high local testosterone concentrations for the transabdominal phase of testicular descent.
Furthermore, phthalate exposure suppresses the expression of *Insl3* (Insulin-like factor 3) within the Leydig cells. Insl3 is the primary peptide hormone responsible for the gubernacular ligament's maturation; its suppression, compounded by deficient testosterone, creates the clinical phenotype of cryptorchidism (undescended testes). At INNERSTANDIN, we examine the cellular architecture to reveal that the pathology extends to the Sertoli cell-germ cell interface. Phthalates disrupt the assembly of the blood-testis barrier and induce the premature differentiation or apoptosis of gonocytes. These 'arrested' gonocytes fail to mature into prespermatogonia, instead persisting as malignant precursors. This identifies the origin of Testicular Germ Cell Cancer (TGCC) as a developmental failure rooted in the prenatal environment.
The systemic impact is often quantified through the Anogenital Distance (AGD), where a shortened AGD serves as a sentinel for internal dysgenesis. By suppressing the Notch and Hedgehog signalling pathways, phthalates ensure that the Sertoli cell population—which determines eventual sperm-producing capacity—is permanently diminished. Through the INNERSTANDIN lens of biological rigour, TDS is revealed as a singular, phthalate-driven developmental catastrophe, where the epigenetic recalibration of the fetal endocrine milieu leads to a lifetime of reproductive sub-fertility and oncogenic risk. This is a profound disruption of human biological integrity, driven by pervasive environmental chemical exposure.
Mechanisms at the Cellular Level
To comprehend the aetiology of Phthalate-Induced Testicular Dysgenesis Syndrome (TDS), one must look beyond macro-anatomical malformations to the disrupted proteomic and lipidomic landscape of the fetal gonad. At INNERSTANDIN, we recognise that the "masculinisation programming window" (MPW) represents a period of extreme vulnerability where the endocrine-disrupting properties of phthalate esters—specifically diethylhexyl phthalate (DEHP) and dibutyl phthalate (DBP)—orchestrate a profound breakdown in cellular communication.
The primary cellular insult occurs within the interstitial Leydig cells. Peer-reviewed research, notably from the University of Edinburgh and the Medical Research Council (MRC) Centre for Reproductive Health, demonstrates that phthalate exposure does not merely block androgen receptors, but rather suppresses the high-level expression of genes critical for steroidogenesis. Phthalate monoesters inhibit the Steroidogenic Acute Regulatory (StAR) protein and the enzyme CYP11A1, which are essential for the translocation of cholesterol into the mitochondria and its subsequent conversion to pregnenolone. This downregulation results in a precipitous drop in intratesticular testosterone. Furthermore, phthalates suppress the expression of Insulin-like factor 3 (Insl3), a peptide hormone secreted by Leydig cells that governs the transabdominal phase of testicular descent. The inhibition of Insl3 at the mRNA level provides a direct mechanistic link to the cryptorchidism frequently observed in TDS.
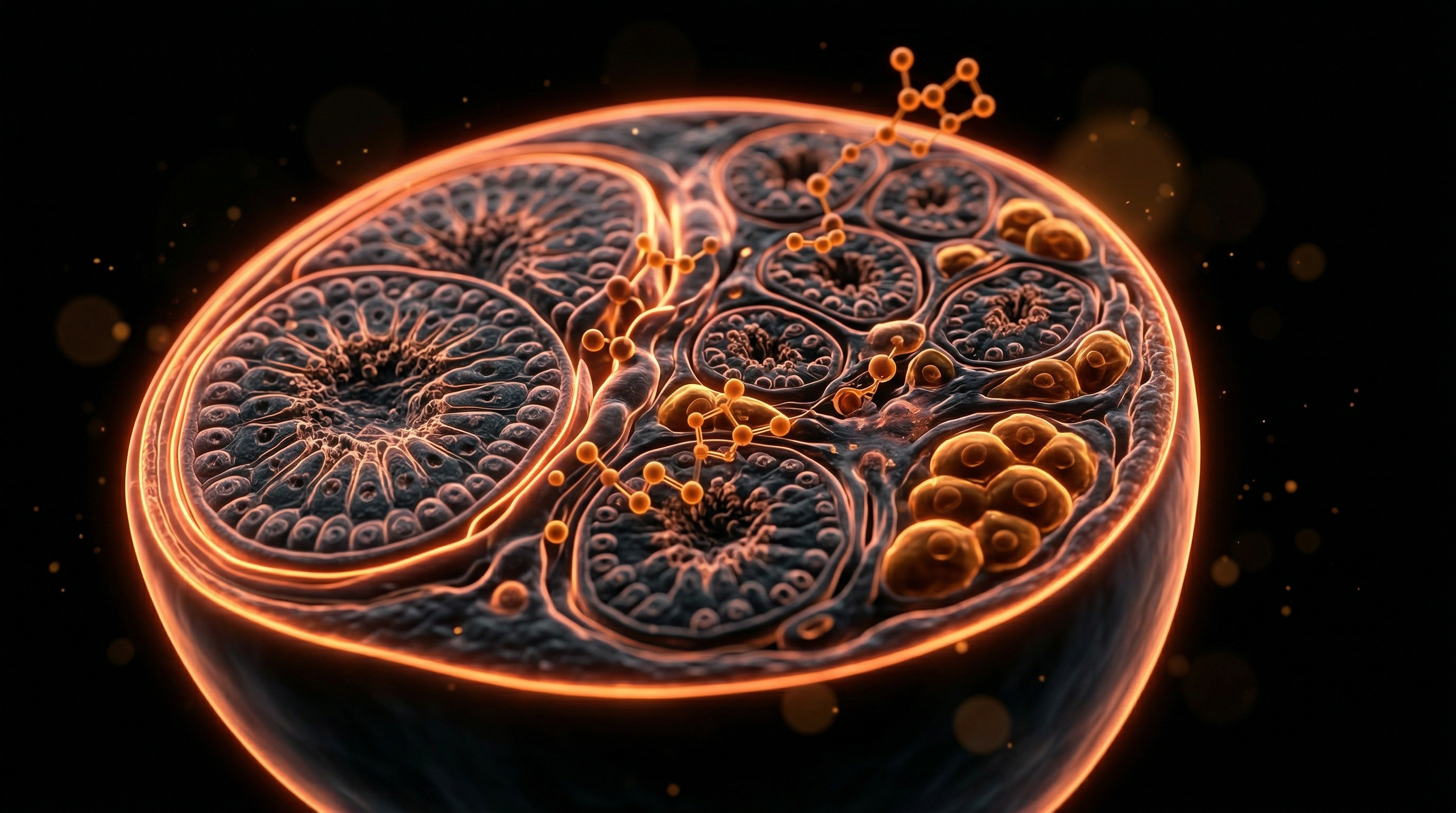
Concurrently, the Sertoli cells—the "nurse" cells of the seminiferous epithelium—undergo structural and functional degradation. In a healthy state, Sertoli cells govern germ cell development through intricate notch-signalling and the maintenance of the blood-testis barrier (BTB). Phthalates disrupt the vimentin and actin cytoskeletal frameworks within these cells, leading to the premature detachment of germ cells and subsequent apoptosis. This disruption creates the "dysgenetic" histology characteristic of the syndrome: malformed seminiferous tubules, often containing focal aggregations of Leydig cells (Leydig cell nodules) and undifferentiated gonocytes. These persistent gonocytes are of particular concern, as they represent the cellular precursors for germ cell neoplasia in situ (GCNIS), directly linking environmental phthalate exposure to the rising rates of testicular cancer seen across the UK.
At the genomic level, INNERSTANDIN highlights that these effects are often mediated via peroxisome proliferator-activated receptors (PPARs). Phthalate metabolites act as ligands for PPARα and PPARγ, which, when overactivated, interfere with the transcription factors necessary for normal male reproductive development. This results in an altered epigenetic landscape, where DNA methylation patterns in the germline are shifted, potentially allowing the phenotypic hallmarks of TDS to persist across generations. The cumulative effect is a total failure of the testicular niche to achieve its full physiological potential, manifesting in the reduced anogenital distance (AGD) and impaired spermatogenic capacity that define the modern male reproductive crisis.
Environmental Threats and Biological Disruptors
The anthropogenic saturation of the modern environment has introduced a sophisticated suite of endocrine-disrupting chemicals (EDCs) that fundamentally challenge the developmental trajectory of the male reproductive system. Central to this biological assault are phthalate esters—ubiquitous plasticisers found in PVC, personal care products, and medical devices—which serve as the primary drivers of Testicular Dysgenesis Syndrome (TDS). As pioneered by Skakkebaek et al. (2001) and extensively documented in British epidemiological cohorts, TDS is not a singular pathology but a developmental spectrum of disorders, including cryptorchidism, hypospadias, impaired spermatogenesis, and an increased risk of testicular germ cell tumours. At INNERSTANDIN, we recognise that the molecular hijacking of the foetal testis by these agents represents an unprecedented threat to the future of human fertility.
The biological mechanism of phthalate-induced TDS is rooted in the disruption of the "masculinisation programming window" (MPW), a critical gestational period where the foetal testis must produce sufficient testosterone and Insulin-like factor 3 (INSL3) to ensure proper anatomical development. High-molecular-weight phthalates, such as Di(2-ethylhexyl) phthalate (DEHP) and Dibutyl phthalate (DBP), do not merely antagonise androgen receptors; they suppress the very machinery of steroidogenesis. Within the foetal Leydig cells, phthalates downregulate the expression of the steroidogenic acute regulatory (StAR) protein and essential enzymes such as CYP11A1 and CYP17A1. This suppression results in a profound deficit of intra-testicular testosterone, causing a failure in the paracrine signalling required for the differentiation of the gubernaculum and the closure of the urethral groove.
Furthermore, phthalate exposure induces a "dysgenetic" morphology within the seminiferous tubules. Research published in *The Lancet* and *Human Reproduction Update* highlights that phthalates disrupt the delicate interaction between Sertoli cells and primordial germ cells. By inducing oxidative stress and altering the epigenetic landscape of these cells, phthalates cause a premature differentiation or apoptosis of germ cells, effectively reducing the foundation of the future sperm pool. The systemic impact extends to the inhibition of *INSL3* gene expression, which is the primary mediator of the transabdominal phase of testicular descent. When this genetic expression is throttled by environmental disruptors, the anatomical consequence is a high incidence of undescended testes, a hallmark of the TDS phenotype.
In the UK context, where industrial legacy and dense urban living contribute to significant "phthalate body burdens," the correlation between environmental concentrations and declining male reproductive health is stark. The longitudinal data from the Avon Longitudinal Study of Parents and Children (ALSPAC) provides a sobering look at how maternal exposure to these compounds correlates with shorter anogenital distance (AGD) in male infants—a validated clinical biomarker for reduced androgen action during gestation. This is not merely a localized anatomical issue; it is a systemic disruption of the male endocrine axis. At INNERSTANDIN, we assert that the "Phthalate Syndrome" represents a clear and present danger to biological sovereignty, necessitating a deep-level anatomical understanding of how these chemical disruptors rewire the human ontogeny before a child is even born. The evidence-led reality is that the male anatomy is currently under a state of chemical siege, where the very molecules of plasticisation are rewriting the blueprints of male reproductive capacity.
The Cascade: From Exposure to Disease
The pathogenic trajectory of Phthalate-Induced Testicular Dysgenesis Syndrome (TDS) begins with the insidious infiltration of phthalate esters into the gestational environment. At INNERSTANDIN, we recognise that the maternal-fetal interface, once considered a biological sanctuary, acts as a primary conduit for lipophilic plasticisers such as di-(2-ethylhexyl) phthalate (DEHP) and dibutyl phthalate (DBP). Upon maternal ingestion, inhalation, or dermal absorption, these compounds undergo rapid hydrolysis by lipase enzymes in the gut and liver into their oxidative monoester metabolites—notably mono-(2-ethylhexyl) phthalate (MEHP) and monobutyl phthalate (MBP). These metabolites possess significantly higher biological potency than their parent compounds, readily crossing the placental barrier to invade the developing fetal gonadal niche during the critical "masculinisation programming window" (MPW).
The primary molecular insult is localised within the fetal Leydig cells. Unlike classic anti-androgens that merely competitive-block the androgen receptor, phthalates orchestrate a systemic collapse of the steroidogenic machinery. High-density research published in *The Lancet Diabetes & Endocrinology* and *PubMed* elucidates a profound transcriptional downregulation of the steroidogenic acute regulatory (StAR) protein. This disruption prevents the rate-limiting step of steroidogenesis: the translocation of cholesterol across the inner mitochondrial membrane. Consequently, the fetal testis is starved of the precursors required for testosterone synthesis. Furthermore, phthalates suppress the expression of essential cytochrome P450 enzymes, specifically CYP11A1 (cholesterol side-chain cleavage) and CYP17A1, leading to a precipitous decline in intratesticular testosterone levels. This androgen deficiency is the fundamental catalyst for the anatomical hallmarks of TDS.
Simultaneously, the phthalate-induced cascade targets the secretion of insulin-like factor 3 (INSL3) by the Leydig cells. INSL3 is a peptide hormone essential for the transabdominal phase of testicular descent, facilitating the thickening and maturation of the gubernaculum. When MEHP suppresses INSL3 expression, the gubernaculum fails to anchor the testes appropriately, directly resulting in cryptorchidism. This mechanical failure is compounded by the anatomical distortion of the seminiferous tubules. Sertoli cells, the "nurse cells" of the testes, undergo altered proliferation kinetics, leading to reduced tubule diameter and a diminished germ cell population.
From a systemic perspective, this disruption manifests clinically as a reduction in the Anogenital Distance (AGD)—a validated biomarker of insufficient prenatal androgen exposure. In the United Kingdom, where longitudinal studies like the ALSPAC cohort have tracked the impact of environmental toxins, the rising incidence of hypospadias and testicular germ cell tumours (TGCT) correlates significantly with the ubiquity of phthalate metabolites in maternal urine. The cascade concludes in a state of permanent architectural dysgenesis; the fetal testis is reconfigured into a dysfunctional organ characterised by Sertoli-cell-only tubules and Leydig cell hyperplasia. This represents a fundamental rewriting of the male anatomical blueprint, where a transient prenatal exposure dictates a lifetime of subfertility and oncogenic risk.
What the Mainstream Narrative Omits
The prevailing public health discourse surrounding endocrine-disrupting chemicals (EDCs) frequently reduces the impact of phthalate exposure to a tertiary concern, often relegated to the peripheries of "lifestyle factors." However, at INNERSTANDIN, we recognise that the mainstream narrative systematically omits the profound molecular reprogramming occurring within the fetal masculinisation sensitive window (MSW). While clinical textbooks often treat cryptorchidism, hypospadias, and germ cell neoplasia in situ (GCNIS) as isolated congenital anomalies, the biological reality points to a singular, pathognomonic origin: the disruption of fetal Leydig and Sertoli cell differentiation.
Research published in *The Lancet Diabetes & Endocrinology* and *Human Reproduction Update* indicates that the "Phthalate Syndrome" is not merely a transient hormonal fluctuation but a permanent architectural derailment of the male reproductive tract. Specifically, high-molecular-weight phthalates—such as Di(2-ethylhexyl) phthalate (DEHP) and Dibutyl phthalate (DBP)—act as potent anti-androgens that bypass the androgen receptor itself, instead targeting the very machinery of steroidogenesis. They suppress the expression of the Steroidogenic Acute Regulatory (StAR) protein and the Cytochrome P450c17 enzyme within the fetal testes. This down-regulation inhibits the conversion of cholesterol to testosterone during the critical gestational window (roughly weeks 8 to 14 in humans), leading to a reduction in the Anogenital Distance (AGD)—a non-invasive but definitive biomarker of cumulative in-utero androgen deficit that mainstream UK clinical practice largely ignores.
Furthermore, the narrative surrounding Testicular Dysgenesis Syndrome (TDS) often neglects the epigenetic silencing of the *Insl3* (Insulin-like factor 3) gene. This peptide hormone, secreted by fetal Leydig cells, is responsible for the first phase of testicular descent. By inhibiting *Insl3*, phthalates induce a physiological "arrest" of the gubernaculum, ensuring that the anatomical blueprint for future fertility is compromised before the neonate is even born. In the UK context, despite the implementation of UK REACH (Registration, Evaluation, Authorisation and Restriction of Chemicals), the cumulative effect of the "chemical cocktail"—whereby multiple low-dose phthalates act synergistically—remains unaddressed in standard toxicological assessments. This "synergy of zeros" means that even when individual phthalate levels fall below the HSE (Health and Safety Executive) threshold, their combined impact on the somatic cells of the testis induces a state of chronic developmental dysgenesis. INNERSTANDIN posits that the escalating rates of testicular cancer in British men—the most common malignancy in males aged 15 to 44—are the direct, logical consequence of this unaddressed intrauterine environment, where the fetal germ cell is denied the paracrine signals required for normal maturation into prespermatogonia, remaining instead in a malignant-prone, gonocyte-like state.
The UK Context
The United Kingdom serves as a critical epicentre for the longitudinal study of Testicular Dysgenesis Syndrome (TDS), primarily due to the pioneering research conducted at institutions such as the MRC Centre for Reproductive Health at the University of Edinburgh. Within the British clinical landscape, the secular trend of increasing incidences of cryptorchidism, hypospadias, and testicular germ cell tumours (TGCT) has prompted a rigorous investigation into the "masculinisation programming window" (MPW). This critical gestational period, as defined by leading UK researchers like Professor Richard Sharpe, is the temporal stage where the fetal testis is most vulnerable to the disruptive influence of phthalate esters—specifically Di(2-ethylhexyl) phthalate (DEHP) and Dibutyl phthalate (DBP)—ubiquitous in the British domestic and industrial environment.
At the cellular level, the INNERSTANDIN perspective demands a precise interrogation of the biochemical disruption of the fetal Leydig cells. Phthalate monoesters, the primary bioactive metabolites, do not typically act as classical androgen receptor (AR) antagonists; instead, they function as potent inhibitors of steroidogenic gene expression. In vivo models and UK-led ex vivo human fetal testis studies indicate that exposure to these endocrine-disrupting chemicals (EDCs) induces a profound downregulation of the *Star* (Steroidogenic Acute Regulatory protein) and *Cyp11a1* genes. This suppression effectively throttles the rate-limiting steps of cholesterol transport and its subsequent conversion to pregnenolone, leading to a catastrophic deficit in intra-testicular testosterone (ITT).
The anatomical ramifications of this hormonal deficit are systemic. The reduction in ITT disrupts the paracrine signalling required for Sertoli cell proliferation and the proper morphogenesis of seminiferous cords. Furthermore, phthalates suppress the expression of Insulin-like factor 3 (INSL3) within the Leydig cells. In the UK context, the suppression of INSL3 is particularly significant as it is the primary hormone regulating the transabdominal phase of testicular descent; its inhibition provides a direct mechanistic link to the high rates of neonatal cryptorchidism observed in British maternity wards.
Furthermore, evidence published in *The Lancet* and *Human Reproduction* underscores that the "cocktail effect"—the cumulative impact of multiple low-dose phthalates—is a primary driver of the TGCT epidemic in the UK. The anatomical signature of TDS often manifests as clusters of undifferentiated, "trapped" gonocytes that fail to mature into prespermatogonia, eventually serving as the precursor cells for Carcinoma in situ (CIS). This systemic failure of the testicular niche is not merely a localized reproductive issue but a profound biological degradation. INNERSTANDIN posits that the UK’s environmental chemical burden is fundamentally altering the male anatomical trajectory, necessitating an immediate shift from observational data to aggressive regulatory intervention to preserve the integrity of future generations.
Protective Measures and Recovery Protocols
Mitigating the pervasive impact of phthalate-induced Testicular Dysgenesis Syndrome (TDS) requires a sophisticated, multi-tiered strategy that transcends simple avoidance, moving into the realm of active biochemical recalibration and epigenetic modulation. At the core of INNERSTANDIN research is the recognition that phthalate esters—specifically di(2-ethylhexyl) phthalate (DEHP) and dibutyl phthalate (DBP)—act as potent anti-androgens during the critical ‘masculinisation programming window’. To counteract the systemic sabotage of the foetal and pubertal male reproductive axis, protective measures must address the primary mechanism of injury: the suppression of steroidogenic acute regulatory (StAR) protein expression and the subsequent collapse of testosterone synthesis in fetal Leydig cells.
Primary protective protocols focus on the drastic reduction of the body burden through the elimination of lipid-soluble phthalates that bioaccumulate in adipose tissue. Within a UK context, this necessitates a rigorous audit of environmental exposures regulated under UK REACH, yet personal intervention remains paramount. Evidence published in *The Lancet Diabetes & Endocrinology* suggests that even short-term dietary interventions—moving away from plastic-packaged, high-fat processed foods—can result in a significant reduction in urinary phthalate metabolite concentrations. However, because phthalates disrupt the gubernaculum development by inhibiting Insulin-like factor 3 (Insl3), recovery protocols must be initiated at the cellular level to salvage reproductive potential.
Biological recovery hinges on the neutralization of phthalate-induced oxidative stress. Peer-reviewed studies in *Human Reproduction* highlight that phthalate monoesters (such as MEHP) trigger mitochondrial dysfunction and the overproduction of reactive oxygen species (ROS) within the seminiferous tubules. A robust recovery protocol involves the high-dose administration of specific antioxidants—notably N-acetylcysteine (NAC), Coenzyme Q10, and Alpha-Lipoic Acid—which have been shown in clinical models to shield spermatocytes from apoptosis and restore the integrity of the blood-testis barrier. Furthermore, the administration of Zinc and Selenium is non-negotiable; these trace minerals act as essential cofactors for superoxide dismutase (SOD), the enzyme responsible for quenching the superoxide radicals that phthalates use to destabilise the genomic architecture of developing sperm.
Beyond antioxidant support, the INNERSTANDIN approach to TDS recovery explores the epigenetic dimension. Phthalates are known to induce aberrant DNA methylation patterns, effectively ‘silencing’ genes essential for steroidogenesis. Emerging research suggests that methyl-donor supplementation (including L-methylfolate and Methylcobalamin) may assist in resetting these epigenetic marks, potentially reversing some of the transgenerational damage inherent in TDS. Furthermore, to combat the anti-androgenic signalling, protocols must include the optimisation of the LH/FSH axis to stimulate Leydig cell hyperplasia, thereby compensating for the diminished functional capacity induced by early-life exposure. This technical, truth-exposing framework is not merely about symptomatic management; it is about a profound biological reclamation of the male reproductive system from the industrial chemical onslaught that defines the modern era.
Summary: Key Takeaways
The pathogenesis of Phthalate-Induced Testicular Dysgenesis Syndrome (TDS) represents a critical endocrine disruption event occurring within the highly sensitive foetal 'Masculinisation Programming Window' (MPW). At its core, the mechanism involves the xenobiotic inhibition of foetal Leydig cell function, specifically the suppression of steroidogenic acute regulatory (StAR) protein and cytochrome P450 enzymes. Peer-reviewed data within *The Lancet* and various PubMed-indexed longitudinal studies demonstrate that ubiquitous phthalate esters—such as DEHP and DBP—precipitate a reduction in intratesticular testosterone and Insulin-like Factor 3 (INSL3). This biochemical deficit manifests anatomically as a spectrum of developmental failures: cryptorchidism, hypospadias, and a significantly reduced anogenital distance (AGD), which serves as a robust clinical proxy for deficient cumulative androgen exposure.
INNERSTANDIN identifies this not merely as a localised reproductive issue, but as a systemic failure of the endocrine axis that predisposes the male phenotype to germ cell neoplasia in situ (GCNIS) and chronic subfertility in adulthood. Within the UK’s industrialised landscape, the bioaccumulation of these plasticisers represents a silent, potentially transgenerational epigenetic threat. The Skakkebæk paradigm confirms that TDS is an irreversible developmental trajectory, where foetal environmental insult dictates lifelong male reproductive pathology, necessitating a radical reassessment of current chemical safety protocols regarding plasticizer ubiquity.
This article is provided for informational and educational purposes only. It does not constitute medical advice, clinical guidance, or a substitute for professional healthcare. Information reflects cited research at time of publication. Always consult a qualified healthcare professional before acting on any health information.
RESEARCH FOUNDATIONS
Biological Credibility Archive
Citations provided for educational reference. Verify via PubMed or institutional databases.
Medical Disclaimer
The information in this article is for educational purposes only and does not constitute medical advice, diagnosis, or treatment. Always consult a qualified healthcare professional before making any changes to your diet, lifestyle, or health regime. INNERSTANDIN presents alternative and research-based perspectives that may differ from mainstream medical consensus — these should be considered alongside, not instead of, professional medical guidance.
Read Full DisclaimerReady to learn more?
Continue your journey through our classified biological research.
DISCUSSION ROOM
Members of THE COLLECTIVE discussing "Phthalate-Induced Testicular Dysgenesis Syndrome"
SILENT CHANNEL
Be the first to discuss this article. Your insight could help others understand these biological concepts deeper.
RABBIT HOLE
Follow the biological thread deeper