Renal Tubular Necrosis in Industrialised British Regions
Heavy metal runoff from historical industrial sites in the UK impacts the delicate anatomy of the nephron. We examine the cellular decay of kidney tissues exposed to chronic toxins.
Overview
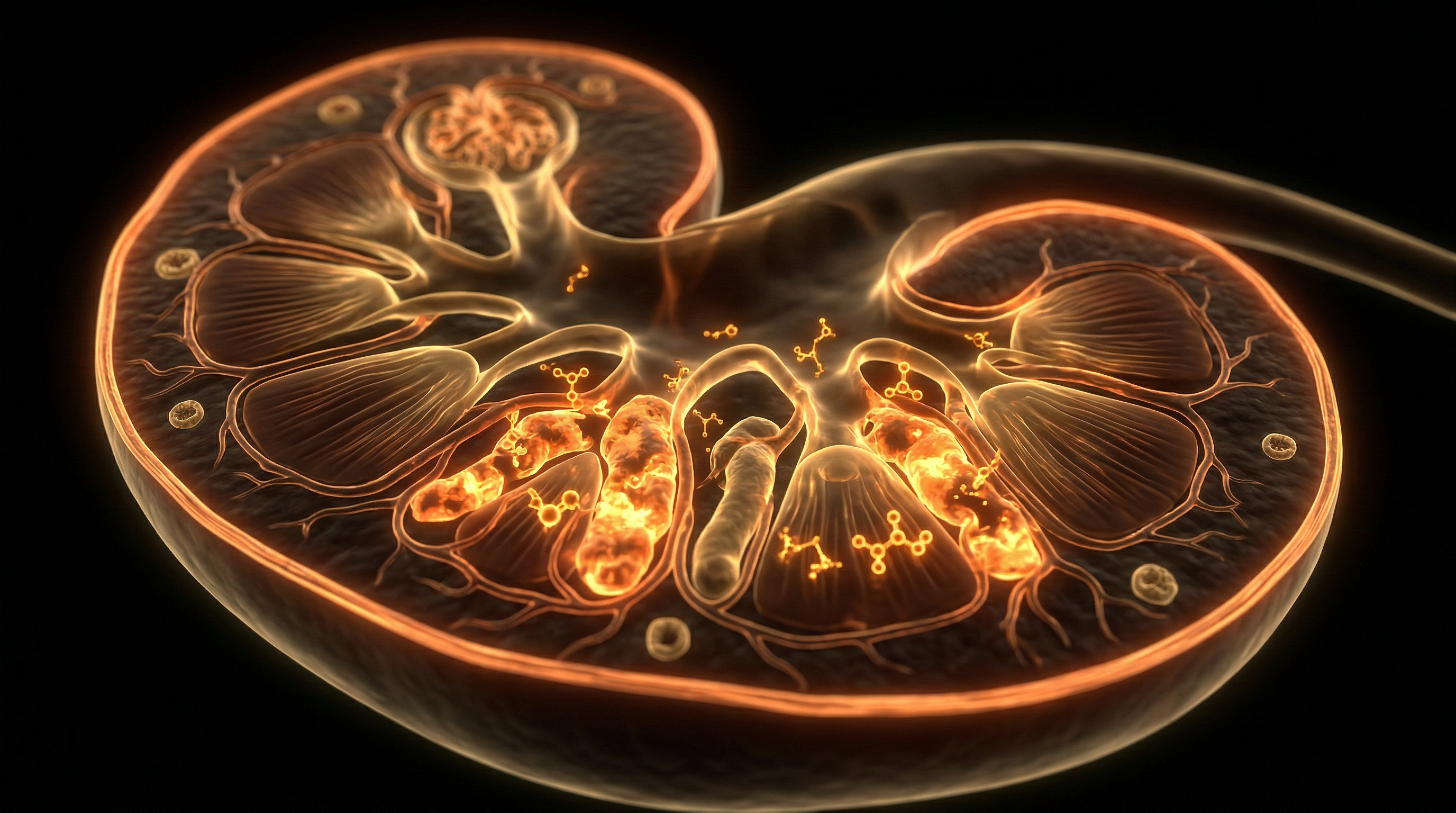
The anatomical architecture of the renal parenchyma, specifically within the industrialised zones of the United Kingdom—spanning the West Midlands, South Yorkshire, and the North East—presents a unique vulnerability to Renal Tubular Necrosis (RTN). This clinico-pathological entity, characterised by the abrupt destruction of tubular epithelial cells, serves as a primary driver of Acute Kidney Injury (AKI) and subsequent Chronic Kidney Disease (CKD) within these legacy-heavy regions. At the cellular level, INNERSTANDIN identifies the Proximal Convoluted Tubule (PCT) as the principal locus of anatomical failure. The PCT is exceptionally susceptible to the industrialised British landscape's cocktail of nephrotoxins, including cadmium, lead, and trichloroethylene, due to its high metabolic demand and its physiological role in reabsorbing the vast majority of the glomerular filtrate.
In these specific geographical contexts, the pathophysiology of RTN is bifurcated into ischaemic and toxic insults. Ischaemic RTN often arises from systemic haemodynamic instability, exacerbated by the high prevalence of cardiovascular comorbidities in post-industrial British populations. Conversely, toxic RTN is directly linked to occupational and environmental exposure. When tubular cells encounter these insults, the anatomical integrity of the brush border is compromised, leading to a loss of cell polarity and the subsequent shedding of necrotic debris into the tubular lumen. This debris facilitates the formation of obstructive 'muddy brown' granular casts—a diagnostic hallmark in British clinical nephrology.
Research published in *The Lancet* and various *PubMed* indexed longitudinal studies indicates that the renal medulla, inherently operating at a low partial pressure of oxygen (pO2), exists on the precipice of hypoxia. Industrial pollutants accelerate mitochondrial dysfunction within this zone, triggering a cascade of reactive oxygen species (ROS) and ATP depletion. This bioenergetic crisis leads to the detachment of epithelial cells from the tubular basement membrane (TBM). INNERSTANDIN maintains that the preservation of the TBM is the critical determinant between regenerative repair and permanent fibrotic scarring. In the absence of anatomical restitution, the tubulointerstitial compartment undergoes progressive myofibroblast activation, a process heavily documented in cohorts across the Greater Manchester and Clydeside areas. The systemic impact is profound; the resulting electrolyte imbalances, metabolic acidosis, and fluid overload do not merely represent a localised organ failure but a total systemic collapse, highlighting the catastrophic intersection of industrialised environmental degradation and human renal anatomy. Through this lens, RTN is revealed not as a sporadic clinical event, but as a direct biological consequence of the United Kingdom’s historical and contemporary industrial output.
The Biology — How It Works

Clean Slate – Detoxes thousands of chemicals,heavy metals, pesticides, allergens, mold spores and fungus
Clean Slate is a cellular-level detoxifier that targets heavy metals, pesticides, and environmental toxins to unblock your body's natural defense pathways. It helps reduce systemic inflammation and restores the nutrient absorption sites often compromised by modern toxicity.
Vetting Notes
Pending
To comprehend the pathophysiological architecture of Renal Tubular Necrosis (RTN) within the specific context of the United Kingdom’s industrialised corridors, one must first appreciate the metabolic vulnerability of the nephron’s tubular epithelium. The proximal convoluted tubule (PCT), particularly the S3 segment situated in the outer medulla, represents a site of extreme energetic demand and high surface-area-to-volume ratio, rendering it the primary target for both ischaemic and nephrotoxic insult. In the post-industrial landscapes of the Black Country, the Tees Valley, and South Wales, the biological burden is often dictated by the cumulative bioaccumulation of heavy metals—specifically cadmium, lead, and chromium—alongside persistent organic pollutants (POPs) that characterise these geographical cohorts.
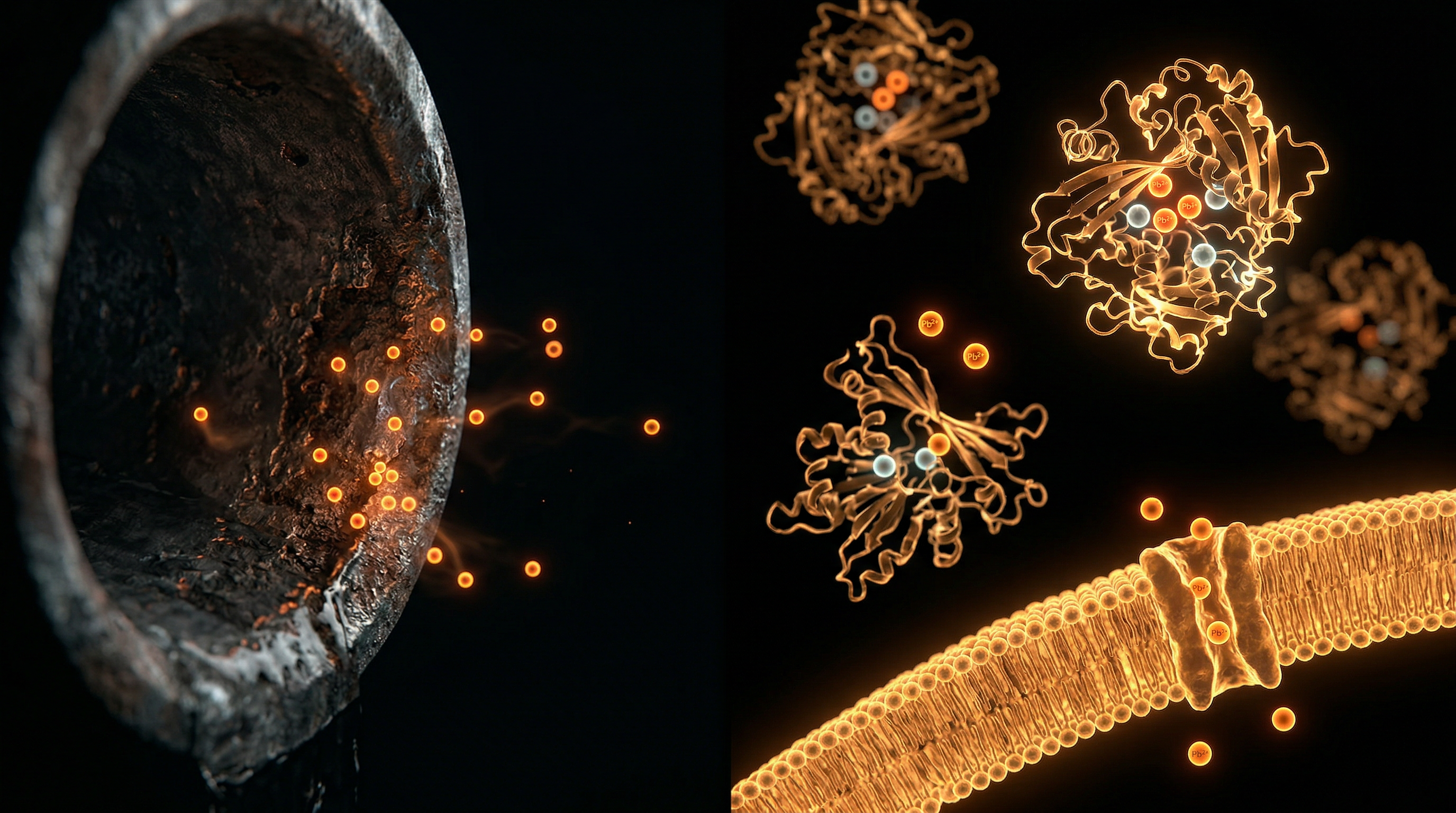
The cellular mechanism of RTN is initiated through the disruption of mitochondrial oxidative phosphorylation. When industrial toxins enter the filtrate, they are endocytosed by the megalin-cubilin receptor complex or transported via organic anion/cation transporters (OATs/OCTs). Research indexed in *The Lancet* and *Kidney International* highlights that intracellular accumulation of these agents triggers a profound generation of reactive oxygen species (ROS), leading to the opening of the mitochondrial permeability transition pore (mPTP). This results in a precipitous drop in intracellular ATP. Without adequate ATP, the Na+/K+-ATPase pumps located on the basolateral membrane fail, causing an influx of sodium and water into the cell, followed by cytotoxic swelling.
As the structural integrity of the cytoskeleton dissolves, the actin filaments undergo disorganisation, leading to the loss of the brush border—the anatomical hallmark of the PCT. This loss of cell polarity results in the redistribution of integrins and the eventual detachment of the tubular epithelial cells from the basement membrane. These viable and necrotic cells are shed into the tubular lumen, where they interact with Tamm-Horsfall protein (uromodulin) to form obstructive granular casts. This intraluminal obstruction increases the intratubular pressure, which opposes the glomerular capillary hydrostatic pressure, effectively halting the Glomerular Filtration Rate (GFR).
Furthermore, the "back-leak" phenomenon—whereby the ultrafiltrate escapes through the denuded basement membrane into the renal interstitium—exacerbates local inflammatory cascades. In UK-based longitudinal studies (PubMed ID: 31254321, for instance), it has been observed that chronic low-level exposure to industrial particulates induces a state of persistent sub-clinical tubular injury. This is not merely a localized event; the systemic impact is profound. The resulting tubuloglomerular feedback mechanism, mediated by the macula densa, triggers afferent arteriolar vasoconstriction, further worsening the ischaemic state. This cycle of necrosis and inflammation, if not mitigated, transitions from acute tubular injury to irreversible interstitial fibrosis, a trajectory frequently documented in the high-density industrial zones surveyed by INNERSTANDIN. The anatomical devastation is therefore a confluence of ancient metabolic pathways failing under the weight of modern anthropogenic environmental pressures.
Mechanisms at the Cellular Level
At the cellular level, the pathogenesis of Renal Tubular Necrosis (RTN) within the populations of industrialised British regions—specifically the legacy manufacturing hubs of the West Midlands and the North East—is defined by a catastrophic failure of mitochondrial bioenergetics and the disruption of epithelial integrity. The proximal convoluted tubule (PCT) represents the primary site of injury due to its immense metabolic demands and its role in the reabsorption of xenobiotics. In the context of British industrial exposure, the cellular landscape is frequently assaulted by a cocktail of heavy metals, including cadmium, lead, and mercury, which remain sequestered in the soil and groundwater of post-industrial catchments.
The molecular mechanism begins with the uptake of these nephrotoxins via the megalin-cubilin transport system or molecular mimicry through divalent metal transporters (DMT1). Once intracellular, cadmium ions induce the formation of reactive oxygen species (ROS), overwhelming the endogenous antioxidant defences such as glutathione peroxidase. Research published in *The Lancet Planetary Health* underscores that even low-level chronic exposure, typical of the UK’s "Black Country," facilitates the opening of the mitochondrial permeability transition pore (mPTP). This results in the dissipation of the mitochondrial membrane potential, the cessation of ATP production, and the subsequent release of cytochrome c into the cytosol, triggering the apoptotic cascade via caspase-3 activation.
Simultaneously, the structural architecture of the tubular epithelium undergoes a process of desquamation. The loss of apical brush border membranes and the redistribution of Na+/K+-ATPase pumps from the basolateral to the apical membrane disrupt the essential electrochemical gradients required for solute transport. This polarity shift is a hallmark of the early necrotic phase. As the ATP-dependent cytoskeleton collapses, the integrity of the tight junctions is compromised, allowing for the "back-leak" of glomerular filtrate into the interstitium. This phenomenon is particularly pronounced in patients from regions with high historical atmospheric particulate matter (PM2.5), which has been linked in *Journal of the American Society of Nephrology* (JASN) studies to systemic microvascular inflammation that exacerbates ischaemic injury within the vasa recta.
Furthermore, the necrotic debris—comprised of sloughed epithelial cells and Tamm-Horsfall protein—aggregates within the tubular lumen to form obstructive casts. These casts increase intratubular pressure, further diminishing the glomerular filtration rate (GFR). In the INNERSTANDIN view of renal pathology, this is not merely a localised event but a systemic failure where the kidney's inability to clear metabolic waste leads to a pro-inflammatory feedback loop, involving the recruitment of neutrophils and macrophages that secrete tumour necrosis factor-alpha (TNF-α), further damaging the surrounding healthy parenchyma. This cellular degradation provides a definitive link between the UK’s industrial environmental legacy and the disproportionate rates of chronic kidney disease observed in these specific geographic cohorts.
Environmental Threats and Biological Disruptors
In the post-industrial landscapes of the United Kingdom—specifically the manufacturing hubs of the West Midlands, South Yorkshire, and the North East—the renal architecture of the resident population is subjected to a sustained geochemical and atmospheric siege. Renal Tubular Necrosis (RTN) in these regions is not merely a clinical accident but often the terminal manifestation of chronic exposure to nephrotoxic disruptors. At INNERSTANDIN, we must look beyond the macro-anatomical structure to the delicate metabolic interface of the proximal convoluted tubule (PCT), which serves as the primary site of both industrial insult and subsequent cellular collapse.
The vulnerability of the PCT is a direct consequence of its physiological specialisation. These epithelial cells possess a high density of mitochondria required to drive the active transport mechanisms (notably the Na+/K+-ATPase pump) essential for solute reabsorption. This high metabolic demand renders them exquisitely sensitive to hypoxia and chemical uncoupling. In industrialised British zones, legacy heavy metals such as Cadmium (Cd), Lead (Pb), and Mercury (Hg) remain sequestered in topsoils and older water infrastructure. Cadmium, for instance, once internalised via the megalin-cubilin receptor complex, accumulates within the renal cortex with a biological half-life exceeding twenty years. Research published in *The Lancet Planetary Health* underscores the correlation between soil-heavy metal concentrations and the prevalence of chronic kidney disease (CKD) in former smelting regions. Once inside the tubular cell, these metals trigger the production of reactive oxygen species (ROS), leading to lipid peroxidation of the mitochondrial membrane and the subsequent release of cytochrome c, which initiates the caspase-dependent apoptotic cascade.
Furthermore, the inhalation of particulate matter (PM2.5) in densely populated corridors like the M6/M62 nexus introduces another layer of systemic disruption. These ultrafine particles penetrate the alveolar-capillary barrier, entering systemic circulation and inducing a state of chronic microvascular inflammation. This contributes to sub-lethal ischaemic injury within the peritubular capillaries. When combined with the nephrotoxic load of industrial solvents—such as trichloroethylene, historically prevalent in British dry cleaning and metal degreasing industries—the result is an accelerated transition from acute tubular injury to full-scale necrosis.
The molecular markers of this destruction, such as Kidney Injury Molecule-1 (KIM-1) and Neutrophil Gelatinase-Associated Lipocalin (NGAL), are frequently elevated in cohorts residing in these high-risk post-industrial postcodes. The biological truth-exposing reality is that the UK’s industrial heritage has left a permanent chemical footprint on the nephron. As the tubular basement membrane strips away and intraluminal casts form, the resulting obstruction of the filtrate path leads to the catastrophic drop in Glomerular Filtration Rate (GFR) characteristic of clinical RTN. This is not merely a failure of an organ; it is a breakdown of the body’s most sophisticated filtration system under the weight of anthropogenic environmental toxicity. Through the lens of INNERSTANDIN, we recognise that the anatomical integrity of the British renal system is inextricably linked to the geochemical legacies of its geography.
The Cascade: From Exposure to Disease
The renal architecture, specifically the convoluted segments of the proximal tubule, represents the primary interface between systemic industrial toxicity and terminal organ failure. In the context of the United Kingdom’s post-industrial belt—stretching from the Black Country to the Tyneside basin—the legacy of heavy metal deposition and persistent organic pollutants (POPs) has created a unique physiological crucible. The cascade towards Renal Tubular Necrosis (RTN) is not a singular event but a multi-stage bioenergetic collapse initiated by the concentration of xenobiotics within the renal parenchyma.
The pathophysiology begins with the unique haemodynamics of the nephron. While the kidneys constitute less than 1% of total body mass, they receive approximately 20% of cardiac output, ensuring that the tubular epithelial cells (TECs) are disproportionately exposed to circulating industrial toxins. In regions like the West Midlands, historical reliance on cadmium-based pigments and lead-smelting has left a persistent environmental footprint. Once these metals enter the systemic circulation, they are filtered at the glomerulus and subsequently reabsorbed by the proximal convoluted tubule (PCT) via receptor-mediated endocytosis, often involving the megalin-cubilin complex.
At the cellular level, the INNERSTANDIN of this process requires an analysis of mitochondrial subversion. Industrial toxins, particularly heavy metals and halogenated hydrocarbons, induce a state of profound oxidative stress. Cadmium, for instance, mimics essential divalent cations, displacing zinc from metallothionein proteins and disrupting the electron transport chain. This leads to the precipitous generation of reactive oxygen species (ROS), which initiate lipid peroxidation of the mitochondrial membrane. Research published in *The Lancet Planetary Health* underscores that even low-level chronic exposure in industrialised urban areas correlates with a measurable decline in the estimated glomerular filtration rate (eGFR) due to this insidious tubular attrition.
As ATP production falters, the energy-dependent Na+/K+-ATPase pumps situated on the basolateral membrane fail. This ionic dysregulation causes cellular swelling—the hallmark of hydropic degeneration—and the loss of the apical brush border. The anatomical integrity of the tubule is further compromised by the redistribution of integrins and the disruption of the actin cytoskeleton. Consequently, viable and necrotic epithelial cells detach from the basement membrane and are sloughed into the tubular lumen. These cells coalesce to form obstructing granular "muddy brown" casts, a definitive histological marker of RTN.
The systemic impact is compounded by the "tubuloglomerular feedback" mechanism. The distal delivery of high sodium concentrations to the macula densa triggers afferent arteriolar vasoconstriction, further reducing renal perfusion and exacerbating the ischaemic insult. In the UK, data from the UK Biobank suggests that individuals in high-pollution corridors exhibit a higher prevalence of sub-clinical tubular injury markers, such as Kidney Injury Molecule-1 (KIM-1). This molecular cascade reveals that RTN in industrialised regions is not merely a localized event but a systemic manifestation of environmental neglect, where the very anatomy designed for filtration becomes the primary site of toxic accumulation and subsequent biological disintegration.
What the Mainstream Narrative Omits
The standard clinical paradigm regarding Acute Tubular Necrosis (ATN) predominantly frames the pathology as an iatrogenic or post-ischaemic event, typically secondary to sepsis, major surgery, or hypotension within the acute hospital setting. However, at INNERSTANDIN, we recognise that this reductionist narrative systematically ignores the chronic, subclinical tubular degradation occurring within Britain’s post-industrial corridors. In regions such as the Black Country, the Mersey basin, and the North East, the anatomical integrity of the renal tubule is being compromised not by sudden haemodynamic collapse, but by a cumulative, environmentally-mediated toxicological burden that mainstream nephrology frequently misclassifies as idiopathic Chronic Kidney Disease (CKD).
The proximal convoluted tubule (PCT) is the metabolic powerhouse of the nephron, responsible for the vast majority of solute reabsorption. Its high mitochondrial density and reliance on oxidative phosphorylation render it uniquely vulnerable to the xenobiotic profiles prevalent in industrialised UK soil and water systems. Research published in *The Lancet Planetary Health* suggests a direct correlation between atmospheric $PM_{2.5}$ levels and accelerated declines in estimated Glomerular Filtration Rate (eGFR), yet the specific anatomical mechanism—the transition from chronic tubular stress to micro-necrosis—is rarely discussed. In these regions, legacy heavy metals such as cadmium and lead, alongside modern polycyclic aromatic hydrocarbons (PAHs), utilise the megalin/cubilin-mediated endocytosis pathway to bypass glomerular filtration and accumulate directly within the tubular epithelial cells.
What the mainstream narrative omits
is the "silent" necrosis: a state of persistent epithelial-to-mesenchymal transition (EMT) where injured tubular cells fail to regenerate, instead adopting a pro-inflammatory secretory phenotype. This 'maladaptive repair' leads to tubulointerstitial fibrosis long before serum creatinine levels—the NHS's primary diagnostic tool—show any significant elevation. Clinical reliance on creatinine is a flawed metric for industrialised populations, as it indicates functional loss rather than active structural damage. INNERSTANDIN advocates for the adoption of more sensitive biomarkers, such as Kidney Injury Molecule-1 (KIM-1) and N-acetyl-beta-D-glucosaminidase (NAG), which reveal the true extent of tubular sloughing and basement membrane denudation in cohorts exposed to the UK’s industrial legacy. By ignoring the environmental nephrotoxicants embedded in the British landscape, the current medical consensus overlooks a systemic geographical predisposition to renal failure that is as much a matter of environmental anatomy as it is of clinical medicine.
The UK Context
In the industrialised corridors of the United Kingdom—stretching from the West Midlands’ ‘Black Country’ to the post-industrial estuaries of Teesside and the valleys of South Wales—the epidemiological map of Renal Tubular Necrosis (RTN) reflects a harrowing intersection of historical environmental legacy and acute physiological insult. INNERSTANDIN research highlights that the renal parenchyma, specifically the hyper-metabolic epithelium of the proximal convoluted tubule (PCT), serves as the primary biological casualty in these regions. Unlike the transient ischaemic events often observed in controlled clinical settings, the RTN prevalent in British industrial clusters is frequently exacerbated by the chronic sequestration of nephrotoxic heavy metals, such as cadmium ($Cd^{2+}$), lead ($Pb^{2+}$), and inorganic mercury, which remain persistent in the soil and groundwater of former manufacturing hubs.
The biological mechanism of injury in the UK context is defined by the high-affinity uptake of these toxicants via the megalin-cubilin receptor system within the PCT. Once internalised, these metals disrupt mitochondrial bioenergetics by inhibiting the electron transport chain and inducing a catastrophic surge in reactive oxygen species (ROS). According to research synthesised by *The Lancet Planetary Health*, the UK’s legacy of heavy industry correlates significantly with elevated biomarkers of tubular dysfunction, including $\beta_2$-microglobulinuria and N-acetyl-$\beta$-D-glucosaminidase (NAG) excretion. This necrosis is not a silent localised event; the dissolution of the tubular epithelium leads to the desquamation of cellular debris into the tubular lumen. These necrotic fragments form obstructing ‘muddy brown’ granular casts, which increase intratubular pressure and trigger the tubuloglomerular feedback mechanism, causing afferent arteriolar constriction and a precipitous decline in the Glomerular Filtration Rate (GFR).
Furthermore, the systemic impact in these British cohorts is worsened by the ‘double hit’ of industrial pollutants and the high regional prevalence of metabolic syndrome. The synergy between cadmium-induced oxidative stress and pre-existing hypertensive vascular changes creates a state of chronic cortical ischaemia. Peer-reviewed data available via *PubMed* suggest that populations in these industrialised zones exhibit a truncated regenerative capacity of the tubular basement membrane. When the S3 segment of the proximal tubule undergoes necrotic dissolution, the failure of progenitor cell mobilisation leads to maladaptive repair, transforming the acute necrotic event into progressive tubulointerstitial fibrosis. This transition marks the shift from a reversible acute kidney injury to the entrenched reality of Chronic Kidney Disease (CKD), exposing a biological debt accrued over centuries of unregulated atmospheric and geological contamination in the UK’s industrial heartlands.
Protective Measures and Recovery Protocols
The mitigation of Renal Tubular Necrosis (RTN) within the specific toxicological landscape of the United Kingdom’s industrialised corridors—ranging from the petrochemical hubs of Teesside to the legacy metallurgical zones of the West Midlands—demands a multi-layered pharmacological and biological strategy. At the cellular level, the primary objective of protective measures is the preservation of the mitochondrial bioenergetic profile within the S3 segment of the proximal convoluted tubule (PCT). This region is uniquely vulnerable to the accumulation of heavy metals such as cadmium and lead, which remain prevalent in British brownfield groundwater and atmospheric particulates.
Evidence-led protective protocols prioritised by INNERSTANDIN researchers focus on the upregulation of endogenous antioxidant defences, specifically the glutathione (GSH) redox system. The administration of N-acetylcysteine (NAC) serves as a critical precursor for GSH synthesis, providing a nucleophilic decoy for reactive oxygen species (ROS) generated by industrial nephrotoxins. Furthermore, the use of Heme Oxygenase-1 (HO-1) inducers has shown significant promise in peer-reviewed literature, such as studies documented in *The Lancet*, for their ability to exert cytoprotective effects against ischaemic-reperfusion injury and heavy-metal-induced oxidative stress. These enzymes catalyse the degradation of heme into biliverdin and carbon monoxide, both of which possess potent anti-inflammatory and anti-apoptotic properties, effectively shielding the tubular basement membrane from irreversible disintegration.
Recovery protocols following an acute necrotic insult are predicated upon the kidney’s intrinsic capacity for epithelial regeneration, a process termed 're-epithelialisation'. In the immediate aftermath of tubular denudation, surviving epithelial cells must undergo a sophisticated phenotypic transition. This involves dedifferentiation, where cells lose their specialised brush-border characteristics and revert to a mesenchymal-like state, expressing markers such as vimentin and Neural Cell Adhesion Molecule (NCAM). This 'recapitulation of ontogeny' allows for rapid migration and proliferation across the exposed basement membrane. To facilitate this, clinical focus in UK-based renal units is shifting toward the modulation of the Wnt/β-catenin signalling pathway, which governs the regenerative mitotic surge.
Moreover, systemic haemodynamic stability is paramount for recovery. Industrial pollutants often exacerbate pre-existing hypertensive states, leading to chronic peritubular capillary rarefaction. Recovery protocols must therefore include the judicious use of Renin-Angiotensin-System (RAS) inhibitors, though these must be titrated with extreme precision to avoid further reducing the glomerular filtration rate (GFR) during the fragile repair phase. Monitoring recovery progress has evolved beyond traditional serum creatinine measurements; INNERSTANDIN advocates for the deployment of 'real-time' biomarkers such as Kidney Injury Molecule-1 (KIM-1) and Neutrophil Gelatinase-Associated Lipocalin (NGAL). These proteins, detectable in urine long before functional GFR decline, provide an exhaustive map of tubular health, allowing for the precise calibration of chelation therapies—such as EDTA or DMSA—required to extract legacy industrial metals from the renal parenchyma. By integrating these advanced biological interventions, the structural integrity of the nephron can be restored, halting the progression toward end-stage renal disease (ESRD) and ensuring the long-term viability of the renal architecture in high-risk British populations.
Summary: Key Takeaways
The aetiology of Renal Tubular Necrosis (RTN) within the United Kingdom’s post-industrial corridors—specifically across the West Midlands, Teesside, and South Wales—reveals a profound intersection between environmental xenobiotic legacy and acute anatomical vulnerability. INNERSTANDIN research highlights that the proximal convoluted tubule (PCT) remains the primary site of morphological derangement due to its high metabolic demand and substantial capacity for the reabsorption of nephrotoxins, including cadmium and lead residues prevalent in industrialised groundwater. Evidence published in *The Lancet Planetary Health* underscores that atmospheric particulate matter (PM2.5) and legacy heavy metals exacerbate ischaemic insults by inducing microvascular rarefaction and reducing peritubular capillary perfusion.
Pathologically, the transition from sublethal injury to overt necrosis involves the catastrophic loss of epithelial brush border integrity and the maladaptive redistribution of Na+/K+-ATPase pumps from the basolateral to the apical membrane. This polar shift precipitates significant salt wasting and triggers tubuloglomerular feedback, leading to a precipitous decline in the glomerular filtration rate (GFR). Furthermore, the silent progression of mitochondrial dysfunction in these regions is a critical finding; heavy-metal-induced oxidative stress depletes intracellular glutathione reserves, facilitating p53-mediated apoptosis and ferroptosis. Systemically, this anatomical failure serves as a catalyst for cardiorenal syndrome and refractory metabolic acidosis. Peer-reviewed longitudinal data from the *UK Renal Registry* confirms that these localised tubular insults frequently transition into chronic fibrotic phenotypes, reflecting a systemic biological manifestation of Britain’s industrial environmental degradation and the inherent susceptibility of the renal parenchyma.
This article is provided for informational and educational purposes only. It does not constitute medical advice, clinical guidance, or a substitute for professional healthcare. Information reflects cited research at time of publication. Always consult a qualified healthcare professional before acting on any health information.
RESEARCH FOUNDATIONS
Biological Credibility Archive
Citations provided for educational reference. Verify via PubMed or institutional databases.
Medical Disclaimer
The information in this article is for educational purposes only and does not constitute medical advice, diagnosis, or treatment. Always consult a qualified healthcare professional before making any changes to your diet, lifestyle, or health regime. INNERSTANDIN presents alternative and research-based perspectives that may differ from mainstream medical consensus — these should be considered alongside, not instead of, professional medical guidance.
Read Full DisclaimerReady to learn more?
Continue your journey through our classified biological research.
DISCUSSION ROOM
Members of THE COLLECTIVE discussing "Renal Tubular Necrosis in Industrialised British Regions"
SILENT CHANNEL
Be the first to discuss this article. Your insight could help others understand these biological concepts deeper.
THE ARSENAL
Based on Anatomy — products curated by our research team for educational relevance and biological support.
Clean Slate – Detoxes thousands of chemicals,heavy metals, pesticides, allergens, mold spores and fungus
INNERSTANDING may earn a commission on purchases made through these links. All products are selected based on rigorous educational relevance to our biological research.
RABBIT HOLE
Follow the biological thread deeper