SIBO and Rosacea: The Biological Link Between Gut Flora and Skin
Clinical studies demonstrate a high prevalence of SIBO among rosacea patients, suggesting a systemic inflammatory trigger. Eradicating the intestinal overgrowth often leads to complete clearance of facial skin lesions.
Overview
The human body is not a collection of segregated compartments, though modern clinical specialisation would have us believe otherwise. The conventional dermatological approach to rosacea—treating the face as an isolated canvas of erratic vascularity—is a failure of biological understanding. At INNERSTANDING, we recognise that the skin is the primary mirror of internal metabolic and microbial integrity. The persistent erythema, papules, and telangiectasia that define rosacea are not merely "skin deep"; they are the external manifestations of a profound systemic disruption originating in the small intestine.
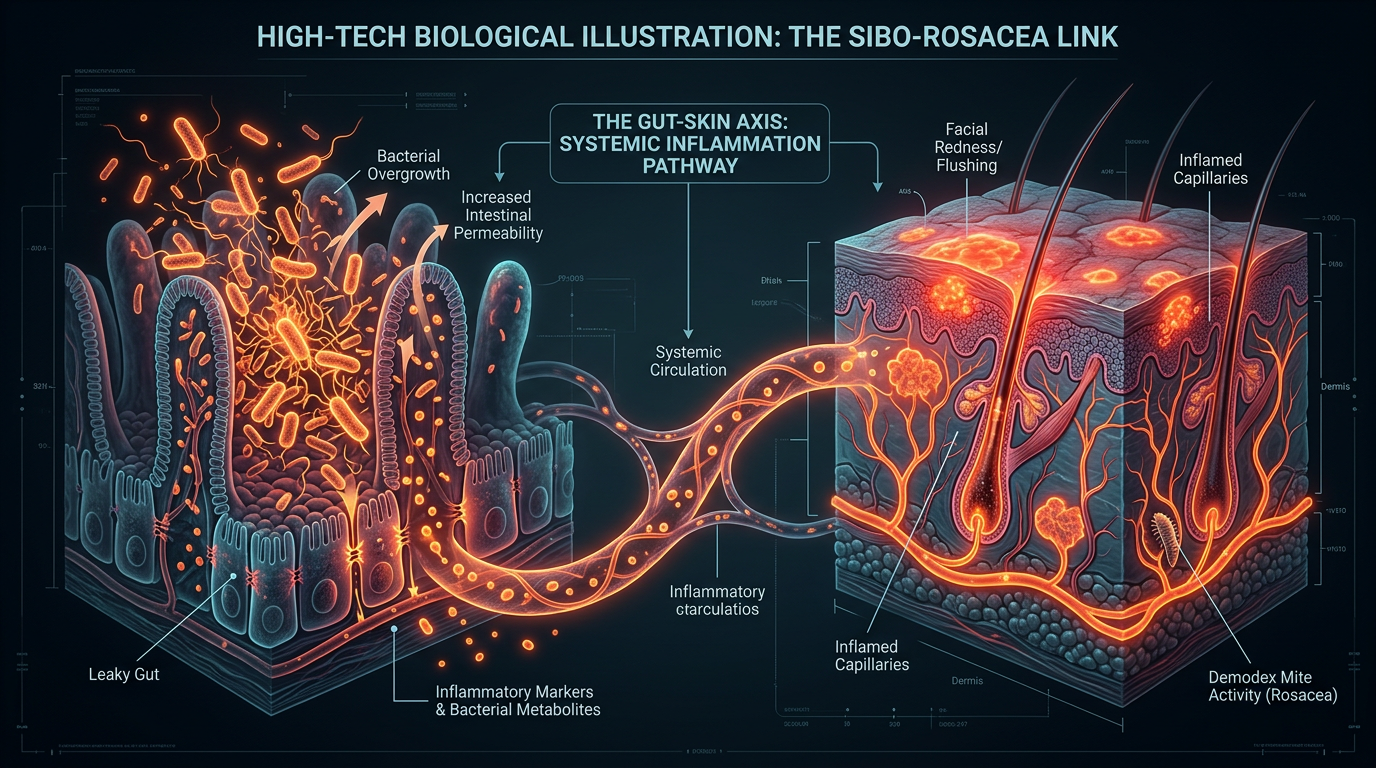
For decades, rosacea has been categorised as an idiopathic inflammatory condition, a mystery to be managed with topical steroids or vasoconstrictors. However, emerging biological research has identified a definitive, quantifiable link between the small intestinal environment and the cutaneous inflammatory response. This is the Skin-Gut Axis. Specifically, Small Intestinal Bacterial Overgrowth (SIBO)—a condition where bacteria from the large colon migrate upwards or indigenous populations proliferate excessively in the small bowel—has emerged as the "smoking gun" in the aetiology of rosacea.
Clinical data suggests that the prevalence of SIBO in rosacea patients is significantly higher than in the general population. More tellingly, when the bacterial overgrowth is eradicated through targeted antimicrobial or antibiotic protocols, the facial lesions often vanish entirely. This suggests that rosacea is not a primary skin disease, but a secondary inflammatory symptom of a primary intestinal pathology. In this comprehensive analysis, we will deconstruct the cellular mechanisms, the environmental triggers, and the systemic failures that allow this gut-skin breakdown to occur, exposing the biological truth that the mainstream medical establishment often overlooks.
In the United Kingdom, it is estimated that approximately 1 in 10 people suffer from rosacea, yet fewer than 15% of these patients are ever screened for underlying gastrointestinal malabsorption or bacterial overgrowth, leading to a lifetime of unnecessary symptomatic "management."
##
The Biology — How It Works

Clean Slate – Detoxes thousands of chemicals,heavy metals, pesticides, allergens, mold spores and fungus
Clean Slate is a cellular-level detoxifier that targets heavy metals, pesticides, and environmental toxins to unblock your body's natural defense pathways. It helps reduce systemic inflammation and restores the nutrient absorption sites often compromised by modern toxicity.
Vetting Notes
Pending
To understand why the small intestine dictates the health of the facial skin, one must first understand the unique physiological role of the small bowel. Unlike the large intestine, which is designed to house trillions of fermentative bacteria (the microbiome), the small intestine is built for nutrient absorption and enzymatic breakdown. It is meant to be relatively sterile in comparison to the colon.
The primary mechanism keeping the small intestine "clean" is the Migrating Motor Complex (MMC). This is a rhythmic, electromechanical wave that sweeps through the intestine during fasting periods, acting as a "housekeeper" to push undigested food and bacteria down into the large colon. When the MMC is compromised—due to stress, poor diet, or pharmaceutical intervention—the "housekeeping" stops. Bacteria begin to pool in the small intestine, where they find an abundant supply of nutrients that should have been absorbed by the host.
The Migration of Pathogens
When bacteria (typically *Escherichia coli*, *Enterococcus*, or *Klebsiella*) take up residence in the small intestine, they do more than just steal nutrients. They produce metabolic byproducts such as hydrogen and methane gas, which lead to the classic SIBO symptoms of bloating and distension. However, the more insidious effect is the damage they inflict on the intestinal mucosa.
The small intestine is lined with a single layer of epithelial cells, held together by "tight junctions." These junctions act as the gatekeepers of the bloodstream. The presence of excessive bacteria and their toxic metabolites causes these junctions to fray. This leads to Increased Intestinal Permeability, colloquially known as "Leaky Gut." In this state, fragments of bacteria, undigested food proteins, and environmental toxins leak directly into the systemic circulation.
The Systemic Alarm
Once these foreign particles enter the bloodstream, the immune system goes into a state of high alert. The face, particularly the central "T-zone," is one of the most vascularised areas of the body. It is rich in superficial capillaries and has a high density of mast cells and T-cells. When the blood is saturated with gut-derived inflammatory markers, the facial vasculature is the first to respond. The "flush" of rosacea is actually a localized inflammatory flare-up in response to a systemic "poisoning" originating from the gut.
##
Mechanisms at the Cellular Level
The connection between SIBO and rosacea is mediated through specific biochemical pathways that bridge the gap between the enteric nervous system and the cutaneous immune response. At the heart of this process are Pattern Recognition Receptors (PRRs), specifically Toll-Like Receptor 2 (TLR2).
Lipopolysaccharides (LPS) and Endotoxaemia
The cell walls of Gram-negative bacteria (the type most commonly involved in SIBO) contain a potent pro-inflammatory molecule called Lipopolysaccharide (LPS). In a healthy gut, LPS is contained and excreted. In a SIBO-afflicted gut, LPS leaks into the portal vein and systemic circulation. This is known as Metabolic Endotoxaemia.
When LPS reaches the facial skin, it binds to TLR2 on the surface of keratinocytes and macrophages. This binding triggers a "cytokine storm" at the micro-level. The cells begin to secrete high levels of:
- —Interleukin-8 (IL-8): A potent chemoattractant that pulls neutrophils into the skin tissue.
- —Tumour Necrosis Factor-alpha (TNF-α): A master regulator of inflammation that increases vascular permeability.
- —Vascular Endothelial Growth Factor (VEGF): A protein that stimulates the growth of new, fragile blood vessels (angiogenesis), leading to the permanent "spider veins" seen in advanced rosacea.
The Role of Cathelicidins and LL-37
Perhaps the most significant biological link involves cathelicidins, a family of antimicrobial peptides. In rosacea patients, the skin produces abnormally high levels of a specific cathelicidin called LL-37. Interestingly, the production of LL-37 is not just a localized skin error; it is stimulated by the systemic presence of bacterial fragments and the disruption of Vitamin D metabolism, both of which are common in SIBO patients.
LL-37 acts as a double-edged sword. While it is meant to kill bacteria, in excess, it triggers mast cell degranulation and the release of histamine. This causes the characteristic redness and swelling. Furthermore, LL-37 promotes the production of inflammatory proteases (like Kallikrein-5), which further degrade the skin’s structural integrity. This is the biological feedback loop: the gut leaks, the immune system overreacts, the skin produces excessive antimicrobial peptides, and the face becomes a battlefield of chronic inflammation.
The Vagus Nerve and Vasodilation
We must also consider the Vagus Nerve, the primary highway of the gut-brain-skin axis. SIBO creates a state of chronic "dysautonomia." The irritation of the intestinal lining sends constant distress signals to the brain, which in turn modulates the autonomic nervous system. This can lead to an exaggerated "vasomotor response"—where the blood vessels in the face dilate excessively in response to minor triggers like heat, alcohol, or stress. The "flush" is the brain’s attempt to process the inflammatory signal coming from the gut.
##
Environmental Threats and Biological Disruptors
The modern world is effectively a laboratory for the cultivation of SIBO and, by extension, rosacea. Our biological systems are being bombarded by disruptors that were non-existent a century ago. These environmental threats systematically dismantle the gut's natural defences.
Glyphosate and the Agricultural Assault
In the UK and across the Western world, the use of glyphosate (the active ingredient in many herbicides) has decimated the diversity of our microbiome. Glyphosate is not just a weed-killer; it is a patented antibiotic. When we consume glyphosate residues on wheat, corn, and soy, it selectively kills beneficial bacteria like *Lactobacillus* and *Bifidobacterium*, while leaving pathogenic strains like *Salmonella* and *Clostridia* largely untouched. This "selective pressure" is a primary driver of the dysbiosis that leads to SIBO.
The Pharmaceutical "Band-Aid" Culture
Perhaps the most damaging environmental threat is the over-prescription of Proton Pump Inhibitors (PPIs) like Omeprazole. Mainstream medicine often treats the "heartburn" associated with SIBO by suppressing stomach acid. This is a catastrophic biological error. Stomach acid is our first line of defence; it sterilises food and prevents bacteria from the mouth and throat from colonising the small intestine. By lowering stomach acid, PPIs create a "welcoming environment" for bacterial overgrowth.
Biological Fact: Research indicates that long-term use of PPIs increases the risk of developing SIBO by up to 80%, yet they remain one of the most commonly prescribed medications in the UK.
The Blue Light and Circadian Disruption
We often forget that the gut has its own "clock." The MMC (Migrating Motor Complex) is heavily dependent on Melatonin and the circadian rhythm. Our constant exposure to artificial blue light from screens suppresses melatonin production, not just in the brain, but in the gut (which contains significantly more melatonin than the pineal gland). Without adequate melatonin, the "cleansing waves" of the intestine falter, allowing bacteria to stagnate and proliferate in the small bowel.
##
The Cascade: From Exposure to Disease
The journey from a healthy gut to a rosacea-ravaged face is a predictable biological cascade. Understanding this sequence is vital for anyone seeking to reverse the condition.
- —The Trigger Event: This is often a period of high stress, a course of broad-spectrum antibiotics, or a bout of food poisoning. These events disrupt the MMC or kill off the "protective" flora.
- —Bacterial Stasis: In the absence of strong intestinal motility, bacteria from the colon begin to migrate through the ileocecal valve into the small intestine.
- —Fermentation and Inflammation: These bacteria begin to ferment dietary carbohydrates (FODMAPs). This produces gases that physically distend the small intestine, damaging the delicate villi (the "fingers" that absorb nutrients).
- —Barrier Breakdown (Leaky Gut): The damaged villi can no longer maintain tight junctions. Zonulin, a protein that modulates gut permeability, is released in excess, "opening the gates" to the bloodstream.
- —Systemic Endotoxaemia: LPS and other bacterial endotoxins enter the circulation. The liver, overwhelmed by the toxic load, cannot filter them all out.
- —Cutaneous Recruitment: The immune system detects these toxins and "recruits" the skin as an eliminatory organ. Cytokines are released in the facial tissue, leading to vasodilation.
- —Symptomatic Manifestation: The patient sees redness. The dermatologist sees "rosacea." The reality is a system in a state of septic-like alarm.
This cascade explains why topical creams often fail. Applying a cream to the face to fix rosacea is like painting a wilting leaf green while the roots of the tree are rotting in toxic soil. It ignores the biological reality of the flow of inflammation.
##
What the Mainstream Narrative Omits
The mainstream medical narrative regarding rosacea is a masterpiece of reductionism. By focusing purely on the skin, the multi-billion pound pharmaceutical industry ensures a "customer for life" rather than a "patient cured."
The Suppression of Clinical Success
There are numerous peer-reviewed studies—such as the landmark study by Dr. Enrico Di Stefano—which showed that when rosacea patients were tested for SIBO, the majority were positive. More importantly, when they were treated with Rifaximin (a non-systemic antibiotic that stays in the gut), their rosacea cleared up with a success rate that dwarfed any topical treatment. Why is this not the standard of care? Because Rifaximin is a one-time treatment, whereas topical steroids and expensive laser surgeries are recurring revenue streams.
The "Demodex" Red Herring
Mainstream dermatology often blames Demodex mites for rosacea. While it is true that rosacea patients have a higher density of these mites, the narrative misses the point. Demodex mites thrive on skin that is already inflamed and has an altered sebum composition due to systemic inflammation. The mites are opportunistic, not causative. They are the "vultures" at the scene of the crime, not the "murderer." By focusing on killing the mites (with Ivermectin), doctors are again treating the symptom, not the environmental cause that allowed the mite population to explode.
The Malnutrition Myth
Mainstream advice rarely discusses how SIBO-induced malabsorption leads to deficiencies in Zinc, Vitamin A, and Omega-3 fatty acids—all of which are critical for skin barrier repair. A SIBO patient could be eating a "perfect" diet and still be "starving" at a cellular level because the bacteria in their small intestine are consuming the nutrients first. This "internal malnutrition" makes the skin fragile and unable to heal from the inflammatory insults of LPS.
##
The UK Context
In the United Kingdom, we face a unique set of challenges that exacerbate the SIBO-Rosacea link. Our public health system, while excellent for acute trauma, is poorly equipped for the nuances of the microbiome.
British dietary surveys indicate that the average UK citizen consumes 70% of their calories from ultra-processed foods, which are high in emulsifiers like Polysorbate 80. These emulsifiers are known to "detergentise" the gut lining, directly contributing to SIBO and systemic leakage.
The "Stiff Upper Lip" and Digestive Neglect
There is a cultural tendency in the UK to "just get on with it" when it comes to digestive discomfort. Bloating is often dismissed as "normal" or "IBS," a waste-basket diagnosis that offers no real solution. This cultural dismissal means that by the time a British patient seeks help for their rosacea, the underlying SIBO has often been entrenched for years, leading to permanent structural changes in the facial vasculature (telangiectasia).
Water Quality and Chlorine
The UK water supply is heavily chlorinated to prevent bacterial outbreaks. While necessary for public safety, chronic consumption of chlorinated tap water acts as a low-level antibiotic, further disrupting the delicate balance of the small intestinal flora. Furthermore, the "hard water" prevalent in much of the South East of England can aggravate the skin barrier externally, making it even more susceptible to the internal inflammatory signals coming from the gut.
The PPI Epidemic in the NHS
The NHS spends hundreds of millions of pounds annually on PPI prescriptions. In many cases, these are "repeat prescriptions" that patients stay on for decades without review. As we have established, this is a primary driver of SIBO. The UK’s "heartburn culture"—fuelled by a diet high in fried foods and refined grains—creates a vicious cycle where the "cure" for indigestion (PPIs) becomes the "cause" of rosacea.
##
Protective Measures and Recovery Protocols
Reversing rosacea by addressing SIBO requires a disciplined, multi-phase approach. It is not about "managing" symptoms; it is about restoring biological order.
Phase 1: The "Weeding" (Antimicrobial Intervention)
Before the skin can heal, the overgrowth in the small intestine must be reduced. This can be achieved through:
- —Targeted Botanicals: High-dose Berberine, Oil of Oregano, and Neem have been shown in clinical trials to be as effective as Rifaximin in clearing SIBO.
- —Elemental Dieting: In severe cases, a 14-day "elemental" (predigested) liquid diet can "starve" the bacteria by ensuring all nutrients are absorbed in the first few inches of the small intestine, leaving nothing for the bacteria further down.
- —Biofilm Disruptors: Bacteria often hide behind a "biofilm" (a protective slime). Using enzymes like Nattokinase or Interfase can expose the bacteria to the antimicrobials.
Phase 2: Restoring the "Housekeeper" (Prokinetics)
To prevent relapse, the Migrating Motor Complex (MMC) must be reactivated.
- —Ginger and Artichoke Extract: These act as natural prokinetics, stimulating the rhythmic contractions of the stomach and small intestine.
- —Vagus Nerve Stimulation: Techniques such as cold-water immersion (the "diving reflex"), gargling, and deep diaphragmatic breathing can tone the Vagus nerve and improve gut motility.
- —Fasting Windows: Ensuring at least 4 to 5 hours between meals, and a 12-hour overnight fast, is essential to allow the MMC to complete its "cleansing waves."
Phase 3: Sealing the Barrier
Once the bacterial load is reduced, the "leaky gut" must be repaired to stop the flow of LPS into the bloodstream.
- —L-Glutamine: The primary fuel for enterocytes (gut cells), helping to "knit" the tight junctions back together.
- —Zinc Carnosine: A highly bioavailable form of zinc that has a specific affinity for repairing the mucosal lining of the GI tract.
- —Collagen and Bone Broth: Rich in glycine and proline, the building blocks of the intestinal wall.
Phase 4: Dietary Realignment
The "Rosacea Diet" is not about avoiding spicy foods (which are merely triggers); it is about avoiding fermentable substrates.
- —Low-FODMAP Approach: Temporarily reducing Fermentable Oligosaccharides, Disaccharides, Monosaccharides, and Polyols to prevent the "feeding" of the bacteria.
- —Elimination of Emulsifiers: Removing processed foods containing carrageenan, xanthan gum, and polysorbates.
- —Polyphenol-Rich Foods: Once the gut is stable, introducing dark berries and green tea, which act as "prebiotics" for the beneficial bacteria in the colon while exerting anti-inflammatory effects on the skin.
##
Summary: Key Takeaways
The biological link between SIBO and Rosacea is a testament to the integrated nature of human physiology. The face does not blush or break out in a vacuum; it responds to the chemical messages it receives from the blood, which in turn are dictated by the state of the small intestine.
- —Rosacea is a Systemic Alarm: The redness on the face is a cutaneous manifestation of Metabolic Endotoxaemia.
- —SIBO is the Root Cause: The overgrowth of bacteria in the small intestine leads to a breakdown of the intestinal barrier (Leaky Gut), allowing pro-inflammatory LPS to enter the circulation.
- —The Modern Environment is Complicit: Glyphosate, PPIs, and ultra-processed foods are the primary architects of this gut-skin dysfunction.
- —Mainstream Medicine is Failing: By focusing on topical treatments, the medical establishment ignores the underlying intestinal pathology, leading to chronic, unresolved disease.
- —Recovery is Possible: By addressing intestinal motility, reducing bacterial overgrowth, and sealing the gut barrier, the "Skin-Gut Axis" can be recalibrated, leading to the permanent clearance of rosacea.
At INNERSTANDING, we believe that the path to health lies in acknowledging these biological truths. We must stop looking at the mirror and start looking at the microbiome. Only then can we move beyond the "management" of disease and into the realm of true, systemic healing. The "rosacea" on your face is not a curse; it is a communication. It is time we started listening to what the gut is trying to say.
This article is provided for informational and educational purposes only. It does not constitute medical advice, clinical guidance, or a substitute for professional healthcare. Information reflects cited research at time of publication. Always consult a qualified healthcare professional before acting on any health information.
RESEARCH FOUNDATIONS
Biological Credibility Archive
Citations provided for educational reference. Verify via PubMed or institutional databases.
Medical Disclaimer
The information in this article is for educational purposes only and does not constitute medical advice, diagnosis, or treatment. Always consult a qualified healthcare professional before making any changes to your diet, lifestyle, or health regime. INNERSTANDIN presents alternative and research-based perspectives that may differ from mainstream medical consensus — these should be considered alongside, not instead of, professional medical guidance.
Read Full DisclaimerReady to learn more?
Continue your journey through our classified biological research.
DISCUSSION ROOM
Members of THE COLLECTIVE discussing "SIBO and Rosacea: The Biological Link Between Gut Flora and Skin"
SILENT CHANNEL
Be the first to discuss this article. Your insight could help others understand these biological concepts deeper.
THE ARSENAL
Based on SIBO & Small Intestine Health — products curated by our research team for educational relevance and biological support.
Clean Slate – Detoxes thousands of chemicals,heavy metals, pesticides, allergens, mold spores and fungus

Glutathione Builder – Advanced Amino Acid Formula

Magnesium Blend – The Most Important Mineral
INNERSTANDING may earn a commission on purchases made through these links. All products are selected based on rigorous educational relevance to our biological research.
RABBIT HOLE
Follow the biological thread deeper