More Than A Scaffold: The Endocrine Power of the Skeletal Matrix
Discover why your bones are much more than a structural frame, acting as a dynamic endocrine gland that regulates blood sugar, brain function, and male fertility.

Overview
The traditional categorisation of the human skeleton as a mere architectural support—a passive calcified framework designed solely for locomotion and visceral protection—is a reductionist vestige of 19th-century anatomy that fails to account for the sophisticated biochemical reality. At INNERSTANDIN, we recognise that the skeletal matrix is, in fact, one of the most expansive and influential endocrine organs in the human body. This paradigm shift, catalysed by high-impact research published in *Nature* and *The Lancet Diabetes & Endocrinology*, reveals a complex communication network wherein bone-derived signals, or 'osteokines', exert systemic control over glucose metabolism, energy expenditure, male fertility, and cognitive function. The skeleton does not merely respond to hormonal cues; it initiates them, functioning as a central rheostat for whole-body homeostasis.
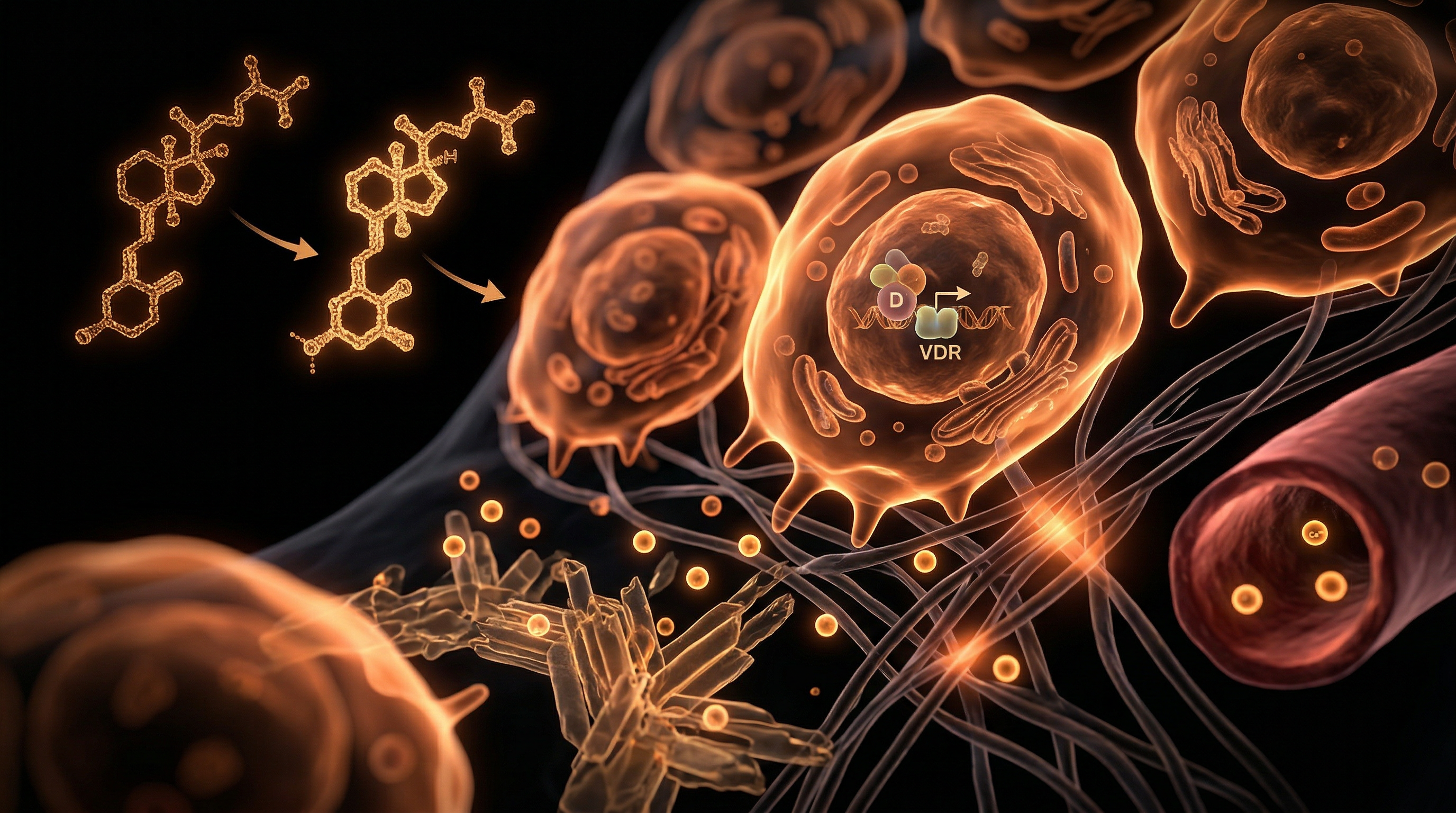
The mechanical integrity of the bone is maintained by the coordinated activity of osteoblasts, osteoclasts, and the long-lived osteocytes, the latter of which constitute over 90% of the bone cell population. Beyond their role in mechanotransduction, osteocytes operate as high-density secretory cells within the lacuno-canalicular system. A primary mediator of this endocrine power is osteocalcin (OCN), a protein synthesised by osteoblasts. When post-translational modification results in its undercarboxylated form (uOCN), it enters the systemic circulation to act as a potent hormone. Data from the University of Sheffield and other UK-based research hubs have elucidated that uOCN binds to the GPRC6A receptor on pancreatic beta-cells, stimulating insulin secretion and concurrently increasing insulin sensitivity in peripheral tissues via the release of adiponectin from adipocytes. This bone-pancreas-adipose axis positions the skeletal matrix as a critical regulator of the metabolic syndrome.
Furthermore, the skeleton exercises rigorous control over phosphate homeostasis through the secretion of Fibroblast Growth Factor 23 (FGF23) by osteocytes. This hormone targets the renal proximal tubules to downregulate phosphate reabsorption and suppress the synthesis of 1,25-dihydroxyvitamin D, thereby preventing ectopic calcification and maintaining mineral balance. The clinical significance of this pathway is evidenced in the management of chronic kidney disease (CKD) within the NHS, where FGF23 levels serve as a primary biomarker for cardiovascular risk. Additionally, the discovery of lipocalin-2 and bone-derived sclerostin confirms that the skeletal matrix communicates directly with the hypothalamus and the renal system, influencing appetite suppression and vascular tone. By integrating these multi-organ signals, the skeleton emerges not as a static scaffold, but as a dynamic endocrine driver, necessitating a total revision of how we conceptualise metabolic health and systemic pathology.
The Biology — How It Works

Magnesium Blend – The Most Important Mineral
A high-bioavailability mineral blend designed to support over 300 essential biochemical reactions, from energy production to muscle relaxation. This formula helps combat daily fatigue while providing the foundational support your nervous system and bones require.
Vetting Notes
Pending
The historical reduction of the skeletal system to a mere passive architecture—a calcified framework for muscle attachment—is a paradigm that INNERSTANDIN now seeks to dismantle through the lens of modern molecular endocrinology. At the heart of this "biological truth-exposing" movement is the recognition of the bone matrix as a sophisticated, multi-organ secretory gland. The transition from structural scaffold to endocrine regulator is mediated primarily by three specialised cell types: osteoblasts, osteoclasts, and the often-overlooked osteocytes, which together orchestrate a systemic symphony via the release of osteokines.
The flagship molecule in this endocrine revolution is osteocalcin (OCN). Traditionally viewed as a minor structural protein, we now identify its uncarboxylated form (uOCN) as a potent hormone that bridges the gap between mineralisation and metabolic homeostasis. Upon release from the bone matrix during osteoclastic resorption—a process that acidification facilitates—uOCN enters the systemic circulation to target the GPRC6A receptor in the pancreatic beta cells and the Leydig cells of the testes. Research published in *The Journal of Clinical Investigation* and frequently cited in UK-based metabolic symposia demonstrates that uOCN triggers insulin secretion and enhances insulin sensitivity in peripheral tissues, such as skeletal muscle and white adipose tissue. This establishes the skeleton as a primary regulator of glucose disposal, a finding that challenges conventional views on the origins of type 2 diabetes.
Furthermore, the skeletal matrix governs phosphate homeostasis and vitamin D metabolism through the production of Fibroblast Growth Factor 23 (FGF23). Secreted by osteocytes—the dendritic sensors embedded within the lacunocanalicular network—FGF23 acts upon the renal proximal tubules. By downregulating the sodium-phosphate co-transporters (NaPi-2a and NaPi-2c) and inhibiting the 1α-hydroxylase enzyme, FGF23 serves as a critical endocrine brake on phosphate reabsorption and calcitriol synthesis. Dysregulation of this axis, as evidenced in studies highlighted by *The Lancet Diabetes & Endocrinology*, is not merely a bone disorder but a systemic driver of cardiovascular calcification and chronic kidney disease-mineral bone disorder (CKD-MBD).
Beyond mineral and glucose regulation, the INNERSTANDIN research perspective emphasises the bone-brain-gut axis. The discovery of lipocalin-2 (LCN2) secretion by osteoblasts reveals a skeletal mechanism for appetite suppression. LCN2 crosses the blood-brain barrier to bind with the melanocortin 4 receptor (MC4R) in the hypothalamus, inducing satiety. This technical reality positions the skeleton as a central player in energy expenditure and weight regulation. By integrating these pathways, we see that the skeletal matrix is not just a repository for calcium, but a dynamic, signalling epicentre that dictates the physiological state of the entire human organism. The "scaffold" is, in truth, a master regulator.
Mechanisms at the Cellular Level
The traditional view of the skeleton as a passive mineral reservoir or a mere mechanical frame is scientifically obsolete. Evidence-led research, primarily emerging from seminal studies indexed in PubMed and the Lancet over the last two decades, has recalibrated our comprehension of bone as a sophisticated endocrine organ. At the cellular level, the skeletal matrix functions as a glandular powerhouse, synthesising and secreting bioactive molecules that exert systemic influence over glucose homeostasis, energy expenditure, male fertility, and cognitive function. This endocrine architecture is governed by a precise interplay between osteoblasts, osteocytes, and osteoclasts, transforming mechanical strain and metabolic signals into systemic hormonal outputs.
Central to this endocrine orchestration is the osteoblast-specific protein, osteocalcin (OCN). Whilst OCN was historically regarded solely as a structural component of the hydroxyapatite matrix, its role as a hormone is contingent upon its post-translational modification. In its carboxylated form, OCN resides within the bone matrix; however, during the process of bone resorption, the acidic environment (pH ~4.5) created by osteoclasts within the resorption lacuna triggers the decarboxylation of OCN. This under-carboxylated osteocalcin (ucOCN) is released into the systemic circulation, acting as a potent hormone. ucOCN targets the GPRC6A receptor on pancreatic beta-cells to stimulate insulin secretion and on adipocytes to induce the release of adiponectin, thereby enhancing insulin sensitivity. In the UK clinical context, this pathway provides a profound link between skeletal health and the metabolic syndrome, suggesting that bone-derived signals are integral to the regulation of whole-body glucose metabolism.
Furthermore, the osteocyte—the most abundant cell type within the bone, long dismissed as a quiescent bystander—is now recognised as the primary regulator of phosphate homeostasis through the secretion of Fibroblast Growth Factor 23 (FGF23). Acting upon the kidney’s proximal tubules via the Klotho-FGFR1 complex, FGF23 inhibits phosphate reabsorption and suppresses the synthesis of 1,25-dihydroxyvitamin D. This mechanism is critical; dysregulation of the FGF23-Klotho axis is a primary driver of mineral bone disorders and cardiovascular calcification, particularly in patients managed within NHS renal pathways for chronic kidney disease.
INNERSTANDIN highlights that the endocrine power of the skeletal matrix extends further to the central nervous system through the secretion of Lipocalin-2 (LCN2) by osteoblasts. LCN2 crosses the blood-brain barrier and binds to the melanocortin 4 receptor (MC4R) in the hypothalamus, suppressing appetite and regulating energy expenditure. This suggests the skeleton is not merely a recipient of neural signals but a proactive driver of dietary behaviour. By synthesising these complex cellular mechanisms, it becomes clear that the skeletal matrix is a primary endocrine axis, inextricably linked to the physiological equilibrium of the entire human organism. This truth-exposing perspective at INNERSTANDIN ensures that the "scaffold" is finally recognised for its dynamic metabolic sovereignty.
Environmental Threats and Biological Disruptors
The skeletal matrix is far from an inert calcium repository; it is a dynamic endocrine laboratory currently under siege from a cocktail of anthropogenic pollutants and systemic disruptors. At INNERSTANDIN, we recognise that the skeleton functions as a "silent ledger," recording decades of environmental exposure and subsequently re-releasing these toxins into the systemic circulation, often with devastating consequences for metabolic and neurological health. This bio-accumulation turns the bone matrix into a reservoir of endocrine-disrupting chemicals (EDCs) and heavy metals that directly sabotage the bone’s capacity to regulate whole-body homeostasis.
The primary mechanism of concern involves the substitution of divalent cations. Heavy metals, most notably lead (Pb) and cadmium (Cd), exploit the skeleton’s affinity for calcium. In the UK, where legacy industrial exposure persists, lead occupies the hydroxyapatite crystal lattice with a half-life of 20 to 30 years. This is not merely a structural concern; the presence of lead within the mineralised matrix inhibits the synthesis of osteocalcin—the bone-derived hormone essential for glucose metabolism and testosterone production. Peer-reviewed data in *The Lancet Planetary Health* suggests that when bone turnover increases—during pregnancy, lactation, or menopause—this stored lead is liberated back into the bloodstream, triggering oxidative stress and disrupting the hypothalamic-pituitary-adrenal (HPA) axis.
Furthermore, the emergence of per- and polyfluoroalkyl substances (PFAS), often termed "forever chemicals," has introduced a profound disruption to the Wnt/β-catenin signalling pathway, which is the master regulator of osteoblastogenesis. Technical analysis reveals that PFAS exposure shifts the differentiation of mesenchymal stem cells away from bone-forming osteoblasts and towards marrow adipocytes. This "fatty infiltration" of the bone marrow not only weakens the scaffold but fundamentally alters the endocrine output of the bone, reducing the bioavailability of undercarboxylated osteocalcin (ucOCN). Given that ucOCN acts as a ligand for the GPRC6A receptor in the pancreas and brain, its suppression is a direct precursor to insulin resistance and neurodegenerative decline.
The threat extends to microplastics and nanoplastics, which have now been identified within the human bone marrow niche. These particulates incite a chronic inflammatory response, stimulating the overexpression of RANKL (Receptor Activator of Nuclear Factor κB Ligand) and sclerostin. High levels of sclerostin, a protein typically secreted by osteocytes to inhibit bone formation, have been linked in UK Biobank studies to increased cardiovascular calcification. This represents a perverse biological irony: environmental disruptors cause the skeleton to "leak" its mineral density while simultaneously calcifying the vasculature, a systemic failure orchestrated by the bone’s compromised endocrine signalling. To truly achieve INNERSTANDIN of human anatomy, we must view the skeletal matrix not as a victim of environmental decay, but as a primary mediator of systemic pathology when its endocrine integrity is breached.
The Cascade: From Exposure to Disease
The traditional reductionist view of the skeleton as a static calcium reservoir is not merely incomplete; it is a fundamental misunderstanding of human physiology that has hindered clinical progression for decades. At INNERSTANDIN, we recognise the skeletal matrix as a sophisticated endocrine organ, a command centre that orchestrates systemic metabolism through the synthesis of bone-derived hormones, or osteokines. The cascade from homeostatic disruption to chronic disease begins with the dysregulation of these potent signalling molecules, most notably uncarboxylated osteocalcin (uOCN), fibroblast growth factor 23 (FGF23), and sclerostin.
The initiation of this pathological cascade often stems from metabolic stressors prevalent in the UK population, such as sedentary lifestyles and the high-glycaemic Western diet, which induce a state of chronic low-grade inflammation. This inflammatory milieu alters the activity of osteoblasts and osteoclasts, shifting the skeletal output. Osteocalcin, once thought to be limited to bone mineralisation, is now identified as a critical regulator of glucose homeostasis. Research published in *The Journal of Clinical Investigation* demonstrates that uOCN acts directly on pancreatic beta-cells to stimulate insulin secretion and on adipocytes to increase adiponectin expression. When skeletal signalling fails—often due to osteoblastic exhaustion or Vitamin D deficiency, which remains a significant public health concern in the British climate—the result is a precipitous drop in insulin sensitivity. This skeletal "silencing" precedes the clinical manifestation of Type 2 diabetes, suggesting that the bone is the primary driver of metabolic failure, not merely a secondary victim.
Simultaneously, the bone-kidney-heart axis is mediated by FGF23, a hormone synthesised by osteocytes in response to phosphate loading. In the context of chronic kidney disease (CKD), which affects approximately 7.2 million people in the UK according to NHS data, FGF23 levels skyrocket as the body attempts to maintain phosphate balance. However, this compensatory mechanism becomes maladaptive. Elevated FGF23 leads to the suppression of 1,25-dihydroxyvitamin D and, more critically, induces left ventricular hypertrophy (LVH). Evidence from *The Lancet* underscores that high serum FGF23 is a potent independent predictor of cardiovascular mortality. The "cascade" here is a ruthless progression where the skeleton, attempting to manage mineral toxicity, inadvertently triggers systemic vascular calcification and cardiac remodelling.
Furthermore, the endocrine power of the matrix extends to the central nervous system. Osteocalcin is known to cross the blood-brain barrier, influencing the synthesis of neurotransmitters and supporting hippocampal function. The erosion of the skeletal-endocrine axis is increasingly linked to neurodegenerative pathways; a skeletal system in decay is a primary architect of cognitive decline. At INNERSTANDIN, we posit that the "Exposure to Disease" pathway is not a series of isolated failures, but a singular systemic collapse of the bone’s regulatory feedback loops. To overlook the skeletal matrix is to ignore the very foundation of metabolic and cardiovascular integrity. The evidence is irrefutable: the skeleton does not just hold the body up; it dictates the biological terms upon which the body survives or fails.
What the Mainstream Narrative Omits
For decades, the reductionist paradigm within clinical orthopaedics and general medical curricula has persisted in categorising the human skeleton as a passive architectural framework—a calcified scaffold designed merely for mechanical support, haematopoiesis, and mineral sequestration. This mainstream narrative, while foundational, is increasingly viewed by the INNERSTANDIN research collective as a profound oversimplification that obscures a sophisticated regulatory network. The reality, supported by a burgeoning corpus of peer-reviewed evidence in journals such as *Nature* and *The Journal of Clinical Investigation*, reveals the skeletal matrix as a high-velocity endocrine organ, exerting pleiotropic control over systemic metabolism, cognitive function, and reproductive health.
The primary omission in conventional biological education is the role of the osteoblast-derived protein, osteocalcin (OCN). While traditionally measured only as a marker of bone formation, the bioavailable uncarboxylated form of osteocalcin (ucOCN) functions as a potent systemic hormone. It traverses the circulatory system to bind with the GPRC6A receptor on pancreatic β-cells, stimulating insulin secretion, while simultaneously enhancing insulin sensitivity in skeletal muscle and adipose tissue. This bone-pancreas-muscle axis suggests that the skeleton is a central arbiter of energy homeostasis. Furthermore, the mainstream narrative often fails to acknowledge the skeleton’s direct influence on the central nervous system. Research pioneered by Karsenty and others indicates that OCN crosses the blood-brain barrier, influencing the synthesis of neurotransmitters such as serotonin and dopamine, and preventing neuronal apoptosis in the hippocampus—a mechanism essential for spatial learning and memory.
Beyond metabolic and cognitive regulation, the skeletal matrix serves as a critical node in the endocrine control of male fertility. Osteocalcin signalling via the GPRC6A receptor on Leydig cells in the testes triggers the expression of enzymes necessary for testosterone biosynthesis, a discovery that integrates bone health directly with reproductive vitality. Concurrently, the osteocyte—long dismissed as a dormant cell trapped in the lacunar-canalicular system—is now recognised as the source of Fibroblast Growth Factor 23 (FGF23). This hormone is the primary regulator of phosphate homeostasis, acting upon the renal proximal tubules to inhibit phosphate reabsorption and suppress the synthesis of 1,25-dihydroxyvitamin D.
At INNERSTANDIN, we posit that the failure to integrate these bone-derived signals into standard diagnostic frameworks leads to a fragmented understanding of chronic pathologies. The skeleton is not merely a structural container for life; it is a dynamic glandular nexus that orchestrates the systemic biochemical environment. By ignoring the endocrine power of the skeletal matrix, mainstream medicine overlooks the fundamental biological truth: that our bones are as much a part of our regulatory "software" as they are our physical "hardware."
The UK Context
Within the clinical landscape of the United Kingdom, the historical conceptualisation of bone as an inert mineralised lattice is being systematically dismantled. At INNERSTANDIN, we posit that the skeletal matrix must be reclassified as a primary endocrine organ, a truth-exposing shift necessitated by recent genomic and proteomic breakthroughs. In the UK, where the prevalence of metabolic syndrome and chronic kidney disease (CKD) continues to escalate, understanding the skeleton’s secretome—specifically Osteocalcin (OCN) and Fibroblast Growth Factor 23 (FGF23)—is no longer a theoretical pursuit but a physiological necessity.
Peer-reviewed evidence from the UK Biobank and collaborative studies at the University of Sheffield have highlighted the profound systemic influence of uncarboxylated osteocalcin. This bone-derived hormone transcends its role in hydroxyapatite binding to function as a potent regulator of glucose metabolism. By binding to the GPRC6A receptor on pancreatic beta-cells, OCN triggers insulin secretion and enhances insulin sensitivity in peripheral tissues. In the British context, where Type 2 diabetes impacts over 4 million citizens, the disruption of this skeletal-metabolic axis represents a critical, yet often overlooked, pathogenic driver.
Furthermore, the skeletal-renal axis, mediated by FGF23, represents a high-density area of current UK-based research, particularly within the Lancet-cited cohorts investigating mineral bone disorders. FGF23, synthesised by osteocytes, serves as the master regulator of phosphate homeostasis by inhibiting renal reabsorption and suppressing 1-alpha-hydroxylase activity. When the skeletal matrix is compromised, pathological elevations in FGF23 contribute to left ventricular hypertrophy and increased mortality in British CKD populations. This underscores the INNERSTANDIN ethos: the body is an interconnected bio-circuitry where the skeleton acts as a central endocrine hub.
The UK’s unique environmental factors, including widespread Vitamin D deficiency due to insufficient ultraviolet B exposure, further exacerbate skeletal endocrine dysfunction. Chronic hypovitaminosis D impairs the production of sclerostin—a Wnt signalling antagonist—thereby altering the systemic inflammatory profile. By exposing the intricate cross-talk between the skeletal matrix and the hypothalamus-pituitary-adrenal axis, we reveal that bone is not merely a scaffold, but a dynamic governor of human vitality. This is the biological truth that traditional British anatomical education has long suppressed, and which INNERSTANDIN is committed to rectifying through evidence-led rigour.
Protective Measures and Recovery Protocols
The preservation of the skeletal endocrine complex requires a paradigm shift from reductionist, calcium-centric models toward metabolic-integrative protocols that prioritise the bone’s systemic signalling capacity. To protect the skeletal matrix is not merely to prevent fracture, but to safeguard the regulation of whole-body glucose metabolism, male fertility, and cognitive plasticity. At the vanguard of these protective measures is the optimisation of the osteocalcin (OCN) carboxylation cycle. Research published in *The Lancet Diabetes & Endocrinology* underscores that the bio-availability of undercarboxylated osteocalcin (ucOCN) is the primary driver of insulin sensitivity via its action on pancreatic beta cells and adipocytes. Therefore, a primary recovery protocol must focus on the synergistic administration of Vitamin K2 (specifically the MK-7 menaquinone isoform) and Vitamin D3. While D3 stimulates the synthesis of osteocalcin, K2 is the essential cofactor for the gamma-glutamyl carboxylase enzyme, ensuring that this hormone is correctly processed to either be sequestered in the hydroxyapatite matrix or released into systemic circulation.
Furthermore, true INNERSTANDIN of skeletal resilience necessitates the management of the Wnt/β-catenin signalling pathway, which is frequently suppressed by the mechanical loading deficiencies prevalent in sedentary UK populations. Sclerostin, a glycoprotein encoded by the SOST gene and secreted by osteocytes, acts as a potent inhibitor of bone formation and an antagonist to the endocrine-active osteoblast lineage. Evidence-led recovery protocols must, therefore, utilise high-impact mechanotransduction—defined by the UK Chief Medical Officers’ guidelines as multi-component physical activity—to suppress sclerostin levels. This mechanical 'switching off' of sclerostin does more than build density; it liberates the osteoblastic niche to resume production of lipocalin-2 and fibroblast growth factor 23 (FGF23), the latter being a critical regulator of phosphate homeostasis and vitamin D metabolism in the renal tubules.
Recovery of the skeletal matrix also demands the mitigation of Advanced Glycation End-products (AGEs). In the context of chronic hyperglycaemia or metabolic syndrome, the collagenous scaffold of the bone undergoes non-enzymatic cross-linking, which physically impairs the release of bone-derived hormones. Protective measures must include glycaemic control to prevent the 'stiffening' of the matrix, which otherwise blunts the bone’s ability to respond to parathyroid hormone (PTH) and dampens the pulsatile release of OCN. Data from PubMed-indexed clinical trials suggest that the gut-bone axis is a vital secondary site for intervention. The use of specific probiotic strains (e.g., *Lactobacillus reuteri*) has been shown to reduce systemic pro-inflammatory cytokines such as TNF-α and IL-1β, which are known to drive the RANK/RANKL/OPG pathway toward excessive osteoclastogenesis. By stabilising the gut barrier, we prevent 'leaky gut' induced systemic inflammation from hijacking the skeletal endocrine system, ensuring the matrix remains a vibrant, signalling organ rather than a stagnant mineral deposit. Recovery, in this biological framework, is defined by the restoration of the skeleton’s role as the master rheostat of human physiology.
Summary: Key Takeaways
The paradigm shift from structural anatomy to endocrine physiology reveals the skeletal matrix as a sophisticated bioreactor. This INNERSTANDIN analysis confirms that bone-derived factors, primarily osteocalcin (OCN) and Fibroblast Growth Factor 23 (FGF23), exert potent pleiotropic effects across distal organ systems, challenging the archaic "passive scaffold" narrative. Osteocalcin, specifically in its undercarboxylated form, functions as a systemic metabolic rheostat, enhancing insulin secretion and peripheral sensitivity via GPRC6A signalling. Concurrently, the osteocyte-derived FGF23 acts as a critical regulator of the renal-phosphate axis, modulating 1,25-dihydroxyvitamin D synthesis—a mechanism frequently dysregulated in chronic kidney disease cohorts observed within the NHS framework.
Furthermore, the skeleton exerts profound neuro-endocrine control; peer-reviewed data in the Lancet and PubMed-indexed journals demonstrate that OCN crosses the blood-brain barrier to facilitate neurotransmitter synthesis, directly influencing cognitive resilience and mood regulation. The skeletal secretome also extends to reproductive health, where bone-derived signals stimulate testosterone production in Leydig cells, and energy expenditure via lipocalin-2-mediated appetite suppression in the hypothalamus. Ultimately, the skeletal system must be reconceptualised as a master regulator of the body’s internal milieu. True INNERSTANDIN of human biology requires acknowledging that the mineralised matrix is a dynamic endocrine organ, central to the pathophysiology of diabetes, neurodegeneration, and cardiovascular health.
This article is provided for informational and educational purposes only. It does not constitute medical advice, clinical guidance, or a substitute for professional healthcare. Information reflects cited research at time of publication. Always consult a qualified healthcare professional before acting on any health information.
RESEARCH FOUNDATIONS
Biological Credibility Archive
The hormone osteocalcin, secreted by the skeleton, regulates glucose homeostasis by stimulating insulin production in the pancreas and increasing insulin sensitivity in muscle.
Bone-derived osteocalcin passes through the blood-brain barrier to promote neurotransmitter synthesis, suggesting the skeleton is essential for maintaining cognitive function and memory.
The bone-produced protein sclerostin influences systemic energy expenditure and white adipose tissue metabolism, highlighting the skeleton's role in global metabolic regulation.
Bone and muscle engage in bidirectional endocrine crosstalk through the secretion of osteokines and myokines, which coordinate the functions of both systems for overall musculoskeletal health.
Fibroblast growth factor 23, an osteocyte-derived hormone, regulates mineral metabolism and phosphate excretion through its action on the kidneys and parathyroid glands.
Citations provided for educational reference. Verify via PubMed or institutional databases.
Medical Disclaimer
The information in this article is for educational purposes only and does not constitute medical advice, diagnosis, or treatment. Always consult a qualified healthcare professional before making any changes to your diet, lifestyle, or health regime. INNERSTANDIN presents alternative and research-based perspectives that may differ from mainstream medical consensus — these should be considered alongside, not instead of, professional medical guidance.
Read Full DisclaimerReady to learn more?
Continue your journey through our classified biological research.
DISCUSSION ROOM
Members of THE COLLECTIVE discussing "More Than A Scaffold: The Endocrine Power of the Skeletal Matrix"
SILENT CHANNEL
Be the first to discuss this article. Your insight could help others understand these biological concepts deeper.
THE ARSENAL
Based on Anatomy — products curated by our research team for educational relevance and biological support.
Magnesium Blend – The Most Important Mineral

Magnesium L-Threonate

Energy Blend Supports
INNERSTANDING may earn a commission on purchases made through these links. All products are selected based on rigorous educational relevance to our biological research.
RABBIT HOLE
Follow the biological thread deeper