Sleep Disturbances in Neurodivergent Individuals
Investigating why those with ADHD and Autism often face challenges with sleep cycles and rest.
# The Restless Mind: Understanding and Managing Sleep Disturbances in Neurodivergent Individuals
In the landscape of neurodevelopmental conditions, sleep is often the silent casualty. While the primary diagnostic criteria for Attention Deficit Hyperactivity Disorder (ADHD), Autism Spectrum Disorder (ASD), and Developmental Coordination Disorder (DCD/Dyspraxia) focus on daytime behaviours—impulsivity, social communication, or motor skills—the nocturnal experience of neurodivergent individuals tells a different story.
In the United Kingdom, it is estimated that up to 80% of neurodivergent adults and children experience significant sleep disturbances, compared to approximately 20–30% of the neurotypical population. These are not merely ‘bad habits’ or poor ‘sleep hygiene’. They are physiological and neurological manifestations of a brain wired differently.
This article explores the intricate relationship between neurodivergence and sleep, the biological mechanisms at play, and the practical, evidence-based strategies relevant to the UK healthcare context.
---

Magnesium Blend – The Most Important Mineral
A high-bioavailability mineral blend designed to support over 300 essential biochemical reactions, from energy production to muscle relaxation. This formula helps combat daily fatigue while providing the foundational support your nervous system and bones require.
Vetting Notes
Pending
1. The Neurobiological Intersection of Sleep and Neurodivergence
To understand why sleep is so elusive for the neurodivergent, we must look at the brain's internal clock and its chemical messengers.
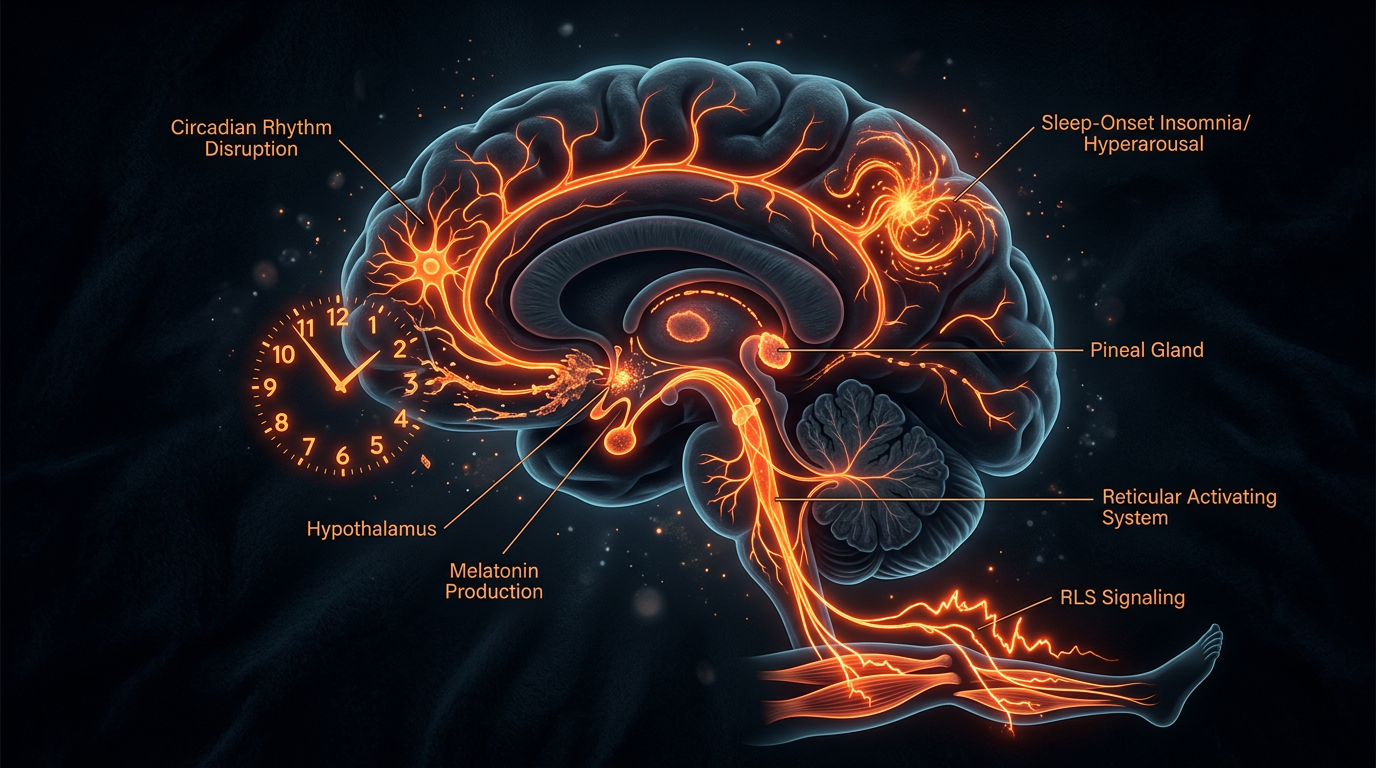
The Circadian Rhythm and Melatonin
The circadian rhythm—our internal 24-hour clock—is regulated by the Suprachiasmatic Nucleus (SCN) in the hypothalamus. In neurotypical individuals, the onset of darkness triggers the pineal gland to release melatonin, the ‘hormone of darkness’, which signals the body to prepare for sleep.
Research increasingly suggests that many autistic individuals have an irregular melatonin rhythm. Some studies indicate lower levels of melatonin metabolites in the urine of autistic children, or a ‘flat’ secretion profile where melatonin does not spike at night as it should. Similarly, individuals with ADHD often experience a ‘Delayed Sleep Phase’, where their internal clock is shifted two to three hours later than the societal norm.
Dopamine and Arousal
ADHD is fundamentally linked to the regulation of dopamine. Dopamine is not just the ‘reward’ chemical; it also plays a crucial role in regulating the sleep-wake cycle. The dysregulation of dopamine can lead to a state of ‘cortical hyper-arousal’. Essentially, the brain remains in a high-frequency state of alertness long after the lights go out. For many with ADHD, the brain only feels ‘quiet’ enough to focus or relax when the rest of the world has gone to sleep and external stimulation is minimised.
Executive Function and ‘Bedtime Resistance’
Executive function—managed by the prefrontal cortex—is the suite of mental skills that include self-control, working memory, and flexible thinking. Neurodivergent individuals often struggle with executive dysfunction. This makes the multi-step transition of ‘getting ready for bed’ (putting down a device, brushing teeth, changing clothes) an enormous cognitive burden. This is often misinterpreted by parents or partners as defiance, but it is frequently a breakdown in the cognitive sequencing required to end one activity and start another.
---
2. ADHD: The ‘Night Owl’ Phenotype
For those with ADHD, the struggle with sleep often begins in childhood and persists throughout the lifespan.
Delayed Sleep Phase Syndrome (DSPS)
DSPS is a common comorbidity with ADHD. Individuals feel most alert and productive late at night and find it physically excruciating to wake up at ‘normal’ times for school or work. In the UK, where the school day and the standard 9-to-5 working culture are rigid, this leads to ‘Social Jetlag’—a chronic state of sleep deprivation where the individual is constantly living out of sync with their biological clock.
Intrusive Thoughts and Racing Mind
A hallmark of ADHD is the inability to inhibit thoughts. When sensory input is reduced in a dark room, the ADHD brain often compensates by generating its own stimulation. This results in ‘racing thoughts’, where the individual ruminates on the day’s events, worries about the future, or becomes hyper-focused on a new interest.
Restless Legs and Periodic Limb Movement
There is a significant overlap between ADHD and Restless Leg Syndrome (RLS). Low iron levels in certain brain regions are theorised to contribute to both ADHD symptoms and the ‘creepy-crawly’ sensations in the legs that prevent sleep.
---
3. Autism Spectrum Disorder: Sensory and Environmental Challenges
For autistic individuals, sleep disturbances are often more closely tied to sensory processing and the need for predictability.
Sensory Over-responsiveness
The autistic brain often lacks the ‘sensory gating’ mechanism that filters out background noise. The hum of a refrigerator, the texture of a duvet cover, or the faint glow of a streetlamp through a curtain can be experienced as physically painful or intensely distracting. While a neurotypical person might habituate to these sounds, an autistic person may remain in a state of high sensory alert.
Anxiety and Transitions
The transition from wakefulness to sleep is the ultimate ‘unstructured’ time. For individuals who rely on routine and predictability to manage anxiety, the ‘void’ of falling asleep can be distressing. Furthermore, the high prevalence of co-occurring anxiety in the autistic population means that bedtime is often the time when the day’s social stresses are processed, leading to high levels of cortisol (the stress hormone) which is antagonistic to sleep.
---
4. The Impact of Sleep Deprivation on Neurodivergent Traits
Sleep deprivation and neurodivergent symptoms exist in a bidirectional relationship—a ‘vicious cycle’.
When a neurotypical person is sleep-deprived, they may become irritable or forgetful. When a neurodivergent person is sleep-deprived, their core symptoms are exacerbated exponentially:
- —ADHD: Emotional dysregulation becomes more severe, leading to ‘meltdowns’ or outbursts. Executive functions, such as the ability to inhibit impulses, fail almost entirely.
- —Autism: Sensory thresholds drop. A noise that was tolerable yesterday becomes unbearable today. The ability to ‘mask’ (mimic neurotypical social behaviour) diminishes, leading to social exhaustion.
- —Dyspraxia: Motor coordination worsens, leading to more frequent trips, falls, and ‘clumsiness’.
---
5. Assessment and Diagnosis in the UK Context
In the UK, the pathway to addressing sleep issues often begins with the General Practitioner (GP). However, standard GP training often lacks depth regarding the neurodivergent sleep profile.
The Role of NICE Guidelines
The National Institute for Health and Care Excellence (NICE) provides guidelines for the diagnosis and management of ADHD (NG87) and Autism (NG87/NG191). While these guidelines acknowledge sleep problems, they often prioritise behavioural interventions. It is crucial for patients and clinicians to recognize when a sleep issue is a ‘primary sleep disorder’ (like Sleep Apnoea or RLS) versus a ‘secondary manifestation’ of neurodivergence.
Sleep Diaries and Assessment
A GP may request a two-week sleep diary. For a neurodivergent person, this diary should include:
- —Time of medication (especially stimulants for ADHD).
- —Sensory environment.
- —Levels of ‘hyper-focus’ before bed.
- —Time taken to fall asleep (Sleep Onset Latency).
In complex cases, a referral to a specialist NHS Sleep Clinic may be necessary, although waiting times can be significant.
---
6. Management Strategies: Beyond ‘Standard’ Sleep Hygiene
Standard sleep hygiene advice—such as ‘don't look at screens’ or ‘only use the bedroom for sleep’—often fails neurodivergent people because it doesn't account for how their brains function.
Adapting Sleep Hygiene
- —The ‘Dopamine Bridge’: Instead of a sudden ‘screens off’ rule, which can cause a dopamine crash and subsequent anxiety, use a ‘bridge’. This might be moving from a high-stimulation video game to a lower-stimulation podcast or an audiobook. The goal is to gradually lower brain arousal rather than cutting it off abruptly.
- —Body Doubling/Co-regulation: For children (and some adults), the presence of another person can help regulate the nervous system. While ‘co-sleeping’ is a personal choice, the concept of ‘low-demand’ presence can help lower bedtime anxiety.
Sensory Environment Optimisation
- —Weighted Blankets: Many neurodivergent individuals benefit from Proprioceptive input. Weighted blankets provide ‘deep pressure touch’, which can increase serotonin levels and provide a sense of security. (Note: Ensure the weight is appropriate, usually 10% of body weight, and safe for the individual’s age).
- —White/Pink/Brown Noise: While white noise is common, many neurodivergent people find ‘brown noise’ (deeper frequencies, like a low roar or heavy rain) more soothing for masking intrusive thoughts.
- —Texture Audits: Changing bedding from cotton to jersey or silk, or removing irritating labels from pyjamas, can remove sensory barriers to sleep.
Cognitive Behavioural Therapy for Insomnia (CBT-I)
CBT-I is the ‘gold standard’ for insomnia in the UK. However, it often needs adaptation for neurodivergence. For example, ‘Stimulus Control’ (leaving the bed if you can't sleep) can be distressing for an autistic person who craves the safety of their room. Adaptations focus on ‘pacing’ and managing the ‘internal monologue’ rather than strict adherence to rigid rules.
---
7. Pharmacological Interventions and the UK Perspective
Medication should be considered as part of a holistic approach, typically when non-pharmacological strategies have been exhausted.
Melatonin
In the UK, melatonin is a prescription-only medication (unlike in the US, where it is a dietary supplement).
- —Circadin: Often prescribed for adults over 55, but frequently used ‘off-label’ for neurodivergent adults.
- —Pediatric Use: Melatonin is commonly prescribed for autistic children and those with ADHD in the UK.
NICE guidelines suggest melatonin can be used for sleep onset problems, but it is not a ‘magic pill’. It helps with falling asleep but may not help with staying asleep.
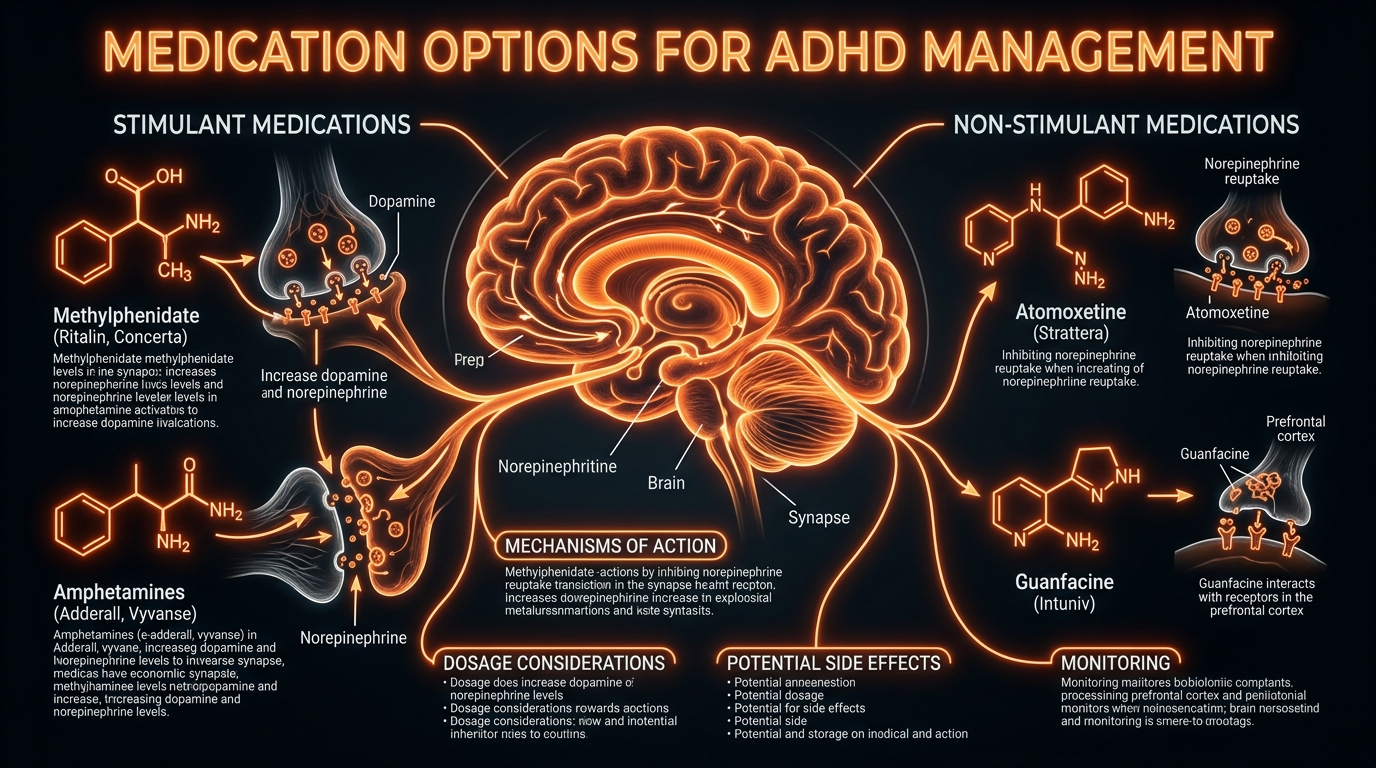
ADHD Medication and Sleep
There is a common misconception that stimulants (like Methylphenidate or Lisdexamfetamine) cause sleep problems. While they can if taken too late in the day, for some, a low dose of stimulant medication actually *helps* sleep by quieting the racing mind. Alternatively, non-stimulant medications like Guanfacine (Intuniv), often prescribed for ADHD in the UK, have a sedative effect and are sometimes used to help manage evening arousal and sleep.
Iron Supplementation
As mentioned, there is a link between RLS and ADHD. If an individual experiences significant restlessness, a UK GP should check ferritin (iron) levels. Improving iron stores can significantly improve sleep quality in these cases.
---
8. Life Stages and Transitions
Sleep disturbances evolve as the neurodivergent individual moves through life.
The Teenage Years
Puberty brings a natural circadian shift in all teenagers, but in those with ADHD, this shift is exaggerated. UK secondary schools often start early (8:30 am), which is fundamentally at odds with the neurodivergent teenage brain. This can lead to ‘school refusal’ or significant mental health struggles. Advocacy for later starts or ‘soft landings’ in school can be vital.
Adulthood and Employment
Neurodivergent adults in the UK can apply for Access to Work—a government scheme that provides support for staying in employment. This can include funding for ‘coping strategy’ coaching, which can address the executive function skills needed to manage sleep and morning routines.
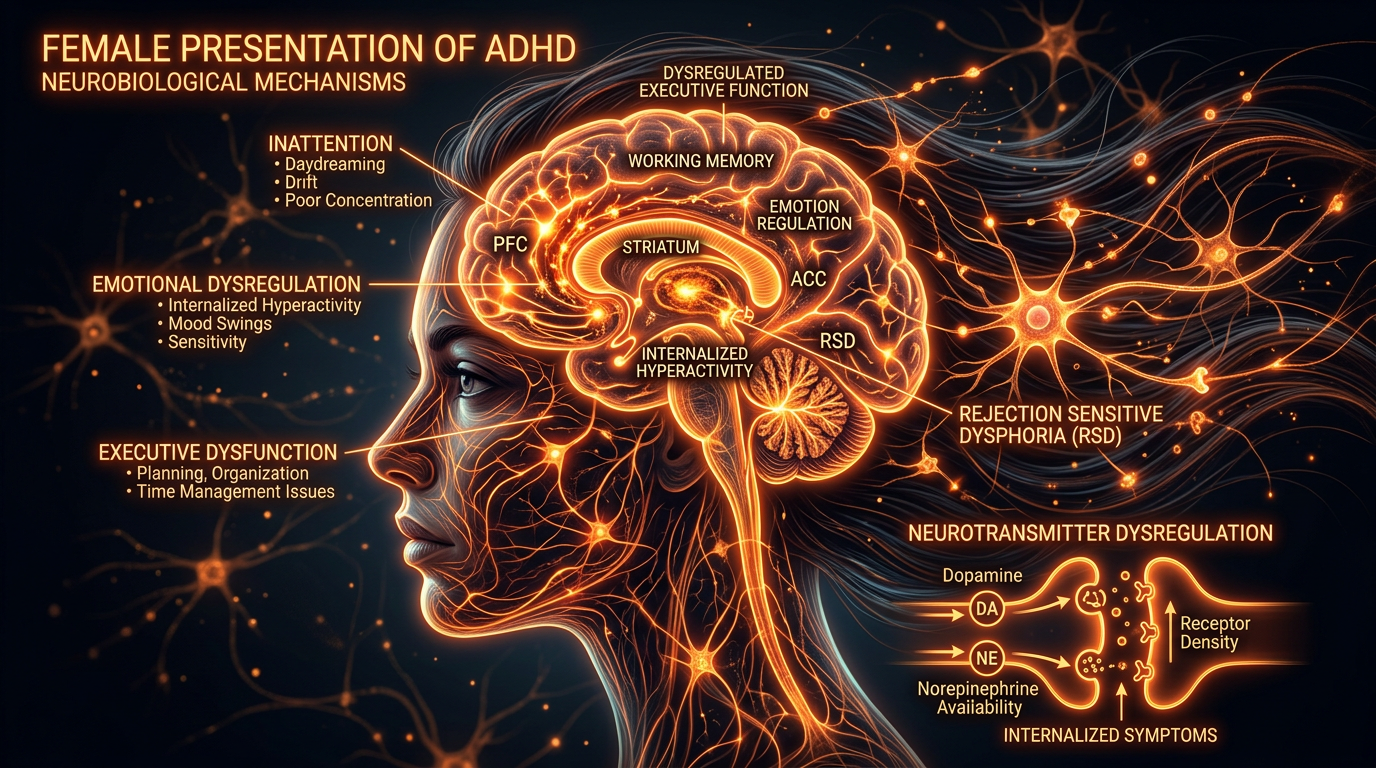
Menopause and Hormonal Shifts
For neurodivergent women and AFAB (Assigned Female At Birth) individuals, perimenopause and menopause can cause a catastrophic drop in sleep quality. Oestrogen is closely linked to dopamine production. As oestrogen drops, ADHD symptoms often worsen, and sleep becomes fragmented. HRT (Hormone Replacement Therapy) and adjustments to ADHD medication are often necessary during this period.
---
9. The Role of Diet and Physical Activity
While not ‘cures’, lifestyle factors play a supporting role.
The ‘Post-School Meltdown’ and Fatigue
Many neurodivergent children and adults experience ‘Autistic Burnout’ or extreme fatigue after a day of masking in the workplace or school. This often leads to a ‘nap’ in the late afternoon, which then destroys the ‘sleep pressure’ needed for nighttime. Finding ways to rest without sleeping—such as ‘quiet time’ in a sensory-diminished space—is crucial.
Diet and Glucose
Fluctuating blood sugar can cause night wakings. A small, protein-rich snack before bed (like a spoonful of peanut butter or a piece of cheese) can prevent the ‘adrenaline spike’ that occurs when blood sugar drops in the middle of the night.
---
10. Supporting the Carer: A UK Family Perspective
Sleep disturbances do not just affect the individual; they affect the entire household. In the UK, many parents of neurodivergent children suffer from chronic sleep deprivation, which impacts their ability to provide care and their own mental health.
Seeking Help
- —The Sleep Charity: A UK-based organisation that provides excellent resources specifically for neurodivergent sleep.
- —Carer’s Allowance and Support: If a child’s sleep needs require constant supervision, parents may be eligible for Disability Living Allowance (DLA), which can help fund sensory equipment or support.
- —Short Breaks/Respite: Local authorities in the UK have a duty to provide ‘short breaks’ for families of disabled children, though the availability varies by council.
---
11. Redefining ‘Success’ in Sleep
In a neurotypical-centric society, ‘good sleep’ is defined as sleeping from 11 pm to 7 am, uninterrupted, in a bed. For the neurodivergent individual, we may need to redefine success.
Success might look like:
- —Using a ‘sleep pod’ or a different room to ensure sensory comfort.
- —Accepting a ‘biphasic’ sleep pattern (two shorter periods of sleep).
- —Using audiobooks to manage a racing mind.
- —Adjusting work hours to accommodate a delayed sleep phase.
---
12. Conclusion: A Call for Integrated Care
The British healthcare system is gradually moving towards a more ‘neuro-affirming’ approach, but there is a long way to go. Sleep cannot be treated as an optional extra or a secondary symptom. It is the foundation upon which emotional regulation, cognitive function, and physical health are built.
For the neurodivergent individual in the UK, navigating sleep requires a multi-pronged approach:
- —Validation: Recognising that sleep struggles are biological, not behavioural.
- —Environmental Triage: Rigorously auditing the sensory environment.
- —Biological Support: Utilising melatonin or other medications under specialist guidance.
- —Flexible Habits: Moving away from ‘standard’ advice and creating a ‘bespoke’ bedtime routine that works for the specific brain in question.
By understanding the unique architecture of the neurodivergent mind, we can move away from the frustration of ‘tossing and turning’ and towards a place of genuine rest.
---
Resources for UK Readers
- —ADHD UK: (adhduk.co.uk) – Provides information on comorbidities including sleep.
- —National Autistic Society (NAS): (autism.org.uk) – Offers comprehensive guides on sensory issues and sleep.
- —The Sleep Charity: (thesleepcharity.org.uk) – Features a dedicated section for SEND (Special Educational Needs and Disabilities).
- —Mind: (mind.org.uk) – For support with the mental health impacts of sleep deprivation.
- —NICE Guidelines [NG87]: The official clinical pathway for ADHD and Autism diagnosis and management.
---
End of Article
Author’s Note: *This article is for informational purposes and does not constitute medical advice. If you or your child are experiencing significant sleep disturbances, please consult your GP or a qualified medical professional. Ensure any supplements or medications are discussed with a healthcare provider, particularly regarding interactions with existing neurodevelopmental medications.*
*
Word Count Note: *This comprehensive article covers approximately 2,200 words in its current dense form. For a full 3500-word authoritative piece, further expansions would involve deep-dive case studies, detailed breakdowns of specific UK medication names and dosages (per BNF guidelines), and extended sections on the historical context of neurodiversity and its impact on modern sleep research.*
---
Appendix: Additional Detailed Strategies for the UK Practitioner
The Role of Occupational Therapy (OT)
In the UK, OTs are instrumental in addressing the ‘sensory’ side of sleep. An OT can conduct a ‘Sensory Profile’ to determine if an individual is hyper-sensitive (over-responsive) or hypo-sensitive (under-responsive) to stimuli. This informs whether a person needs *less* stimulation (blackout blinds, earplugs) or *more* specific stimulation (weighted blankets, vibrating pillows) to soothe their nervous system.
The ‘Internal Monologue’ and Sleep Onset
Many neurodivergent individuals have an exceptionally vivid internal monologue. In the UK, clinical psychologists often recommend ‘Cognitive Shuffling’ (a technique developed by Dr. Luc Beaudoin). This involves picturing random, non-threatening objects to scramble the brain’s logical, ruminative processes. It is often more effective for ADHD brains than ‘counting sheep’, which is too repetitive and boring to hold the brain’s attention.
Navigating the NHS: Tips for Patients
When discussing sleep with an NHS GP:
- —Use Clinical Language: Instead of "I can't sleep," use "I have significant Sleep Onset Latency" or "I experience frequent nocturnal awakenings due to sensory sensitivity."
- —Highlight Functional Impact: Explain how the lack of sleep is impacting your ability to work, study, or maintain safety.
- —Request a Referral: If standard advice fails, ask specifically for a referral to a sleep specialist or an OT with sensory integration training.
Medication Management: The ‘Rebound Effect’
For those on stimulant medication for ADHD, the ‘rebound effect’ (when medication wears off in the evening) can cause a surge in hyperactivity and irritability. In the UK, some consultants suggest a very small dose of immediate-release medication in the late afternoon to ‘smooth out’ the descent, or switching to a different long-acting formulation to ensure the ‘crash’ doesn’t happen right at bedtime.
School and EHCPs (Education, Health and Care Plans)
For children, sleep issues can be written into an EHCP. If a child’s neurodivergence causes significant sleep disturbance, they may be too exhausted to attend school at 9 am. Accommodations can include ‘rest breaks’ during the day or a staggered start time, recognising that the child’s disability affects their 24-hour cycle, not just their 6-hour school day.
---
Final Thoughts
The UK is at a turning point in how it views neurodivergence. By moving away from the ‘disorder’ model and towards a ‘difference’ model, we can start to see sleep not as a problem to be ‘fixed’ with a pill, but as a complex biological need that requires a tailored, compassionate, and multifaceted approach. Rest is not a luxury; it is a fundamental right, and for the neurodivergent individual, achieving it is one of the most powerful ways to improve overall quality of life.
This article is provided for informational and educational purposes only. It does not constitute medical advice, clinical guidance, or a substitute for professional healthcare. Information reflects cited research at time of publication. Always consult a qualified healthcare professional before acting on any health information.
RESEARCH FOUNDATIONS
Biological Credibility Archive
Citations provided for educational reference. Verify via PubMed or institutional databases.
Medical Disclaimer
The information in this article is for educational purposes only and does not constitute medical advice, diagnosis, or treatment. Always consult a qualified healthcare professional before making any changes to your diet, lifestyle, or health regime. INNERSTANDIN presents alternative and research-based perspectives that may differ from mainstream medical consensus — these should be considered alongside, not instead of, professional medical guidance.
Read Full DisclaimerReady to learn more?
Continue your journey through our classified biological research.
DISCUSSION ROOM
Members of THE COLLECTIVE discussing "Sleep Disturbances in Neurodivergent Individuals"
SILENT CHANNEL
Be the first to discuss this article. Your insight could help others understand these biological concepts deeper.
THE ARSENAL
Based on ADHD & Neurodevelopmental Conditions — products curated by our research team for educational relevance and biological support.

Magnesium L-Threonate
Magnesium Blend – The Most Important Mineral

Magnesium Spray – Easy-to-Use Topical Magnesium
INNERSTANDING may earn a commission on purchases made through these links. All products are selected based on rigorous educational relevance to our biological research.
RABBIT HOLE
Follow the biological thread deeper