The Oxalate Crisis: Kidney Stones and Beyond
High oxalate levels from supposedly healthy diets are causing systemic inflammation misdiagnosed as autoimmune disorders. We examine the biological mechanism of calcium oxalate crystal formation in soft tissues.
Overview
In the current landscape of modern nutrition, a silent epidemic is unfolding—one that is frequently masked by the very labels we associate with "health" and "vitality." At INNERSTANDING, our investigation into the biochemical underpinnings of chronic disease has revealed a staggering oversight in contemporary clinical practice: the systemic toxicity of oxalic acid. While mainstream medicine, including the overstretched corridors of the NHS, predominantly views oxalates through the narrow lens of nephrolithiasis (kidney stones), the reality is far more insidious.
Oxalates are highly reactive molecules found in abundance in many "superfoods" such as spinach, almonds, rhubarb, and beetroot. When the body’s capacity to process these compounds is breached—due to gut dysbiosis, genetic predisposition, or sheer dietary volume—the resulting crystalline structures do not merely exit via the urinary tract. Instead, they migrate into soft tissues, joints, and even the central nervous system.
The consequences are catastrophic. We are witnessing a surge in systemic inflammatory conditions, chronic pain syndromes, and neurological impairments that are being reflexively categorised as "autoimmune" or "idiopathic" (of unknown cause). This article serves as an exhaustive expose on the biological mechanisms of oxalate toxicity, the failure of the current diagnostic paradigm, and the urgent need for a radical shift in how we perceive "healthy" eating in the 21st century.
Fact: It is estimated that approximately 80% of kidney stones are composed of calcium oxalate, yet the systemic deposition of these crystals in other organs remains largely unmonitored by standard diagnostic protocols.
The Biology — How It Works
To understand the oxalate crisis, one must first understand the molecule itself. Oxalic acid ($C_2H_2O_4$) is a simple dicarboxylic acid. In the plant kingdom, it serves two primary roles: as a metabolic byproduct and as a sophisticated defence mechanism. Because plants are sessile organisms, they cannot flee from predators. Instead, they utilise chemical warfare. High-oxalate plants use these compounds to deter insects and herbivores by making the plant tissues either toxic or physically abrasive.
The Soluble vs. Insoluble Distinction
In the human diet, oxalates exist in two primary forms: soluble and insoluble.
- —Insoluble Oxalates: These are typically found as calcium oxalate crystals within the plant matter. When consumed, they generally pass through the digestive tract with minimal absorption, though they can act as physical irritants to the gut lining.
- —Soluble Oxalates: These are salts of sodium or potassium oxalate. These are far more dangerous because they are readily absorbed into the bloodstream. Once in the blood, they seek out calcium ions to bind with, forming needle-like crystals of calcium oxalate.
The Mechanism of Absorption
The human body has no enzyme capable of breaking down the oxalate molecule. We rely entirely on specific gut bacteria—most notably *Oxalobacter formigenes*—to degrade dietary oxalates. However, decades of broad-spectrum antibiotic use in the UK have decimated these microbial populations in a significant portion of the citizenry. Without these "oxalate-eaters," the intestinal permeability (often referred to as "leaky gut") common in modern patients allows high concentrations of oxalic acid to flood the systemic circulation.
The "Raphide" Weaponry
In plants like spinach or kiwi, oxalates often take the form of raphides—needle-shaped crystals. Under a microscope, these look like bundles of microscopic spears. When these are ingested in the quantities promoted by "green smoothie" enthusiasts, they don't just "pass through." They can cause micro-trauma to the epithelial lining of the oesophagus and intestines, facilitating their own entry into the internal environment.
Mechanisms at the Cellular Level
Once oxalic acid enters the blood and extracellular fluid, it initiates a series of biochemical cascades that disrupt fundamental cellular homeostases.
Mitochondrial Dysfunction and Oxidative Stress
The most profound impact of oxalates occurs within the mitochondria—the powerhouses of the cell. Oxalate ions can inhibit the enzymes of the Krebs cycle, specifically succinate dehydrogenase. This leads to a precipitous drop in ATP (cellular energy) production. Furthermore, the presence of oxalate crystals triggers the production of Reactive Oxygen Species (ROS).
Key Term: NLRP3 Inflammasome – Oxalate crystals are recognised by the body as "danger signals," activating the NLRP3 inflammasome. This is a multi-protein complex that initiates the release of highly inflammatory cytokines, leading to chronic, systemic inflammation that mimics autoimmune flares.
The Depletion of Glutathione
To combat the oxidative stress caused by oxalates, the body exhausts its reserves of glutathione, the master antioxidant. As glutathione levels plummet, the cell becomes increasingly vulnerable to other environmental toxins and heavy metals. This creates a synergistic toxicity where oxalates and heavy metals (like aluminium and lead) bind together, forming even more stable and difficult-to-remove deposits within the brain and bone tissue.
Lysosomal Rupture
Cells attempt to defend themselves by "eating" the crystals through a process called phagocytosis. The crystals are taken into lysosomes (the cell’s recycling centres). However, the sharp, needle-like structure of calcium oxalate can physically puncture the lysosomal membrane. This releases digestive enzymes into the cell’s cytoplasm, essentially causing the cell to digest itself from the inside out. This is a primary driver of the tissue necrosis and scarring observed in chronic oxalosis.
Environmental Threats and Biological Disruptors
The oxalate crisis does not exist in a vacuum. It is exacerbated by a range of modern environmental factors that have compromised our biological resilience.
The Glyphosate Connection
The widespread use of glyphosate (the active ingredient in many herbicides) in UK agriculture has had a devastating effect on gut health. Glyphosate is a patented antibiotic; it selectively kills beneficial bacteria while allowing pathogenic strains to thrive. By eliminating *Oxalobacter formigenes* and other oxalate-degrading microbes, glyphosate has effectively lowered the "drawbridge," allowing dietary oxalates to enter the bloodstream unchecked.
Fungal Overgrowth (Candida)
While much of our oxalate burden is exogenous (from food), a significant portion can be endogenous (produced inside the body). Certain fungal species, such as *Candida albicans* and *Aspergillus*, are known to produce oxalic acid as a metabolic byproduct. In patients with chronic yeast overgrowth—often a result of high-sugar diets and antibiotic overuse—the body is subjected to a constant internal drip of oxalates, regardless of dietary intake.
Nutrient Deficiencies: The Vitamin B6 Paradox
Vitamin B6 (Pyridoxine) is a critical cofactor for the enzyme AGT (alanine-glyoxylate aminotransferase), which converts glyoxylate into glycine, preventing it from turning into oxalate. In the presence of B6 deficiency—extremely common due to poor diet and the interference of certain medications—the body's internal production of oxalate skyrockets. This is often the missing link in patients who "eat well" but still suffer from high oxalate levels.
Warning: High-dose Vitamin C supplementation can be a double-edged sword. While essential for health, in an environment of high oxidative stress, excess Vitamin C can metabolise directly into oxalic acid, contributing to the total body burden.
The Cascade: From Exposure to Disease
How does a spinach salad lead to a diagnosis of Fibromyalgia or Rheumatoid Arthritis? The cascade is a journey from the gut to the most sensitive tissues of the body.
Stage 1: The Overflow
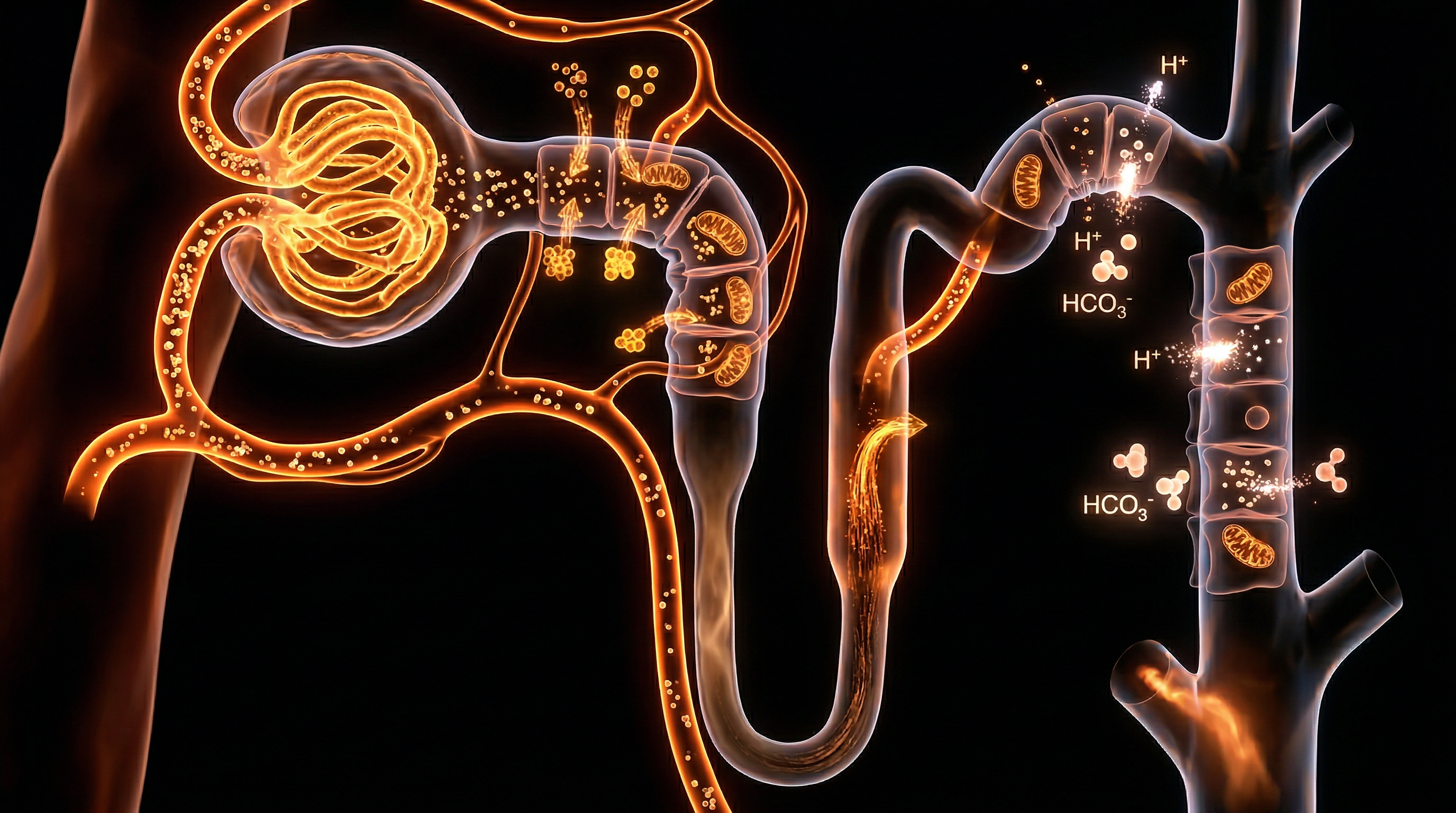
When the kidneys reach their limit for oxalate excretion (approximately 30-50mg per day for a healthy adult), the body must find somewhere else to put the toxin. It cannot allow oxalic acid to remain in the blood, as it would cause fatal electrolyte imbalances.
Stage 2: Sequestration in Soft Tissue
The body begins depositing calcium oxalate crystals in "low-flow" areas or tissues with high mineral turnover. Common sites include:
- —The Thyroid Gland: Leading to nodules and hypothyroidism.
- —The Joints: Causing "pseudo-gout" and what is frequently misdiagnosed as osteoarthritis.
- —The Eyes: Resulting in "gritty" feelings or visual disturbances.
- —The Breasts: Micro-calcifications seen on mammograms are often calcium oxalate.
Stage 3: The Autoimmune Mimicry
As these crystals embed in the fascia and connective tissues, they cause constant mechanical irritation. The immune system, sensing the damage but unable to "dissolve" the mineral shards, remains in a state of permanent activation.
- —Fibromyalgia: Many cases of fibromyalgia are actually the result of microscopic oxalate crystals embedded in the muscle spindles and fascia, causing "all-over" pain that does not respond to traditional painkillers.
- —Interstitial Cystitis: Often called "Painful Bladder Syndrome," this is frequently caused by oxalate crystals being excreted through the bladder wall, essentially "shredding" the delicate lining.
- —Vulvodynia: Unexplained pelvic pain in women has been linked in numerous studies to high urinary oxalate levels.
Stage 4: Neurotoxicity
Perhaps most concerning is the evidence that oxalates can cross the blood-brain barrier, especially when it has been compromised by systemic inflammation. Once in the brain, oxalates can activate the microglia (the brain's immune cells), leading to neuro-inflammation. This has been linked to brain fog, "depersonalisation" disorders, and increasingly, the symptoms associated with the autism spectrum.
What the Mainstream Narrative Omits
The mainstream medical and nutritional establishment is currently promoting a diet that is historically unprecedented in its oxalate density. The "Plant-Forward" movement, while well-intentioned in its goal to reduce processed food consumption, has inadvertently created a toxicity crisis.
The Superfood Trap
The list of "healthy" foods highest in oxalates is a "who's who" of modern wellness:
- —Spinach: One of the highest sources. A single "green smoothie" can contain over 1,000mg of oxalate—twenty times the daily limit.
- —Almonds: Used in milk, flour, and snacks.
- —Beetroot: Promoted for nitric oxide and athletic performance.
- —Sweet Potatoes: A staple of the "Paleo" diet.
- —Turmeric: Ironicaly taken for inflammation, yet high in soluble oxalates.
The Failure of Testing
Standard NHS testing for oxalates is almost exclusively limited to 24-hour urine collections for recurrent kidney stone sufferers. However, this test is fundamentally flawed for diagnosing systemic oxalosis. If a patient's body is efficiently *sequestering* oxalates into their tissues (bones, joints, glands), their urinary output may appear normal or even low. The toxin is in the body, not the bucket.
Furthermore, the "Normal" ranges used by labs are based on a population that is already consuming high-oxalate diets, meaning the baseline for "healthy" is skewed significantly too high.
The Misdiagnosis Pattern
Doctors are trained to look for pathology, not toxicology. When a patient presents with joint pain, fatigue, and brain fog, the GP will run an ANA (Antinuclear Antibody) test or check CRP (C-Reactive Protein). If these are elevated, the patient is referred to a rheumatologist and often put on immunosuppressants or steroids. These drugs may mask the inflammation, but they do nothing to address the physical shards of calcium oxalate causing the damage.
The UK Context
In the United Kingdom, the oxalate crisis is particularly acute due to specific dietary trends and the structural limitations of the NHS.
The "Eatwell Guide" Fallacy
The Public Health England (PHE) "Eatwell Guide" encourages a heavy reliance on starchy carbohydrates and vegetables. While it mentions reducing sugar and salt, it contains zero warnings regarding anti-nutrients like oxalates. The push for "meat-free Mondays" and veganism has led to a massive increase in the consumption of soy, nuts, and spinach—the "Oxalate Trifecta."
The NHS Backlog and Chronic Pain
With the NHS facing record waiting lists, patients with chronic "unexplained" pain are often relegated to long-term pain management programmes. These programmes focus on "living with the pain" rather than identifying the biochemical cause. We are seeing a generation of Britons being "managed" with gabapentin, amitriptyline, and opioids for what is essentially a dietary poisoning.
The Water Factor
Many parts of the UK, particularly the South East, have "hard" water, high in calcium. While calcium can be protective if consumed *with* oxalates (to bind them in the gut), the combination of high-mineral water and high-oxalate food in a population with compromised gut health is a recipe for systemic calcification.
NHS Statistic: Hospital admissions for kidney stones in England have increased by over 60% in the last decade. This is the "canary in the coal mine" for the systemic oxalate crisis.
Protective Measures and Recovery Protocols
Recovery from oxalate toxicity is not a fast process. Because the body stores these crystals in the bones and deep tissues, clearing them requires a strategic and patient approach.
1. The "Low and Slow" Approach
The most dangerous thing a high-oxalate consumer can do is quit oxalates "cold turkey." This triggers a phenomenon known as Oxalate Dumping. When the blood levels of oxalate drop suddenly, the body sees an opportunity to flood the bloodstream with stored crystals from the tissues to be excreted. This can cause severe symptoms, including skin rashes, "sandy" stools, extreme fatigue, and even temporary kidney distress.
- —Protocol: Reduce oxalate intake by no more than 10% per week. Replace high-oxalate staples with low-oxalate alternatives (e.g., replace spinach with arugula/rocket or romaine lettuce; replace almonds with macadamias or walnuts).
2. Calcium Binding
The most effective way to prevent oxalate absorption is to ensure that any oxalate consumed is bound to calcium in the digestive tract, forming an insoluble mass that is excreted in the stool.
- —Strategy: Consume calcium-rich foods (like hard cheeses or yogurt) or take a calcium citrate supplement *with* meals. Calcium citrate is particularly effective because the citrate component also helps to dissolve existing crystals in the blood.
3. Essential Cofactors
Supporting the body's internal machinery is vital for processing endogenous oxalates and mitigating the damage caused by dumping.
- —Vitamin B6 (P5P form): To support the AGT enzyme.
- —Magnesium: Oxalates deplete magnesium. Magnesium citrate or malate can help prevent crystal formation.
- —Potassium Citrate: Helps to alkalinise the urine and prevent the crystallisation of oxalic acid in the kidneys.
4. Hydration and Lemon Juice
Maintaining high urinary flow is essential. Adding fresh lemon juice to water provides a natural source of citrate, which is the body's primary defence against crystal formation in the urinary tract.
5. Gut Restoration
Healing the gut lining and reintroducing beneficial microbes is the long-term solution. While *Oxalobacter formigenes* is not yet available as a commercial probiotic in the UK, increasing fermented foods (if tolerated) and using spore-based probiotics can help rebuild a resilient microbiome.
Summary: Key Takeaways
The "Oxalate Crisis" represents a fundamental failure of modern nutritional science to account for the chemical defences of plants and the fragility of the human microbiome.
- —Oxalates are metabolic toxins that the human body cannot break down. They act as "microscopic shards" that damage tissues and trigger systemic inflammation.
- —The "Autoimmune" epidemic is often a misdiagnosis of systemic oxalosis. When the body cannot excrete oxalates, it stores them in joints, organs, and the brain.
- —Modern "Superfoods" like spinach, almonds, and rhubarb are the primary drivers of this crisis. A single green smoothie can exceed the body's processing capacity by a factor of twenty.
- —NHS diagnostic patterns are currently inadequate, focusing only on kidney stones while ignoring the systemic manifestations of the toxicity.
- —Recovery must be gradual. "Oxalate dumping" can be a severe physiological event. A slow reduction, combined with calcium/citrate supplementation, is the safest path to health.
At INNERSTANDING, we believe that true health begins with the removal of biological disruptors. The oxalate crisis is a call to return to a more ancestral, biologically appropriate way of eating—one that respects the chemical complexity of the natural world and the limitations of our own physiology. The path to recovery is not through more "superfoods," but through the informed, strategic removal of the toxins that have been hiding in plain sight on our dinner plates.
This article is provided for informational and educational purposes only. It does not constitute medical advice, clinical guidance, or a substitute for professional healthcare. Information reflects cited research at time of publication. Always consult a qualified healthcare professional before acting on any health information.
RESEARCH FOUNDATIONS
Biological Credibility Archive
Citations provided for educational reference. Verify via PubMed or institutional databases.
Medical Disclaimer
The information in this article is for educational purposes only and does not constitute medical advice, diagnosis, or treatment. Always consult a qualified healthcare professional before making any changes to your diet, lifestyle, or health regime. INNERSTANDIN presents alternative and research-based perspectives that may differ from mainstream medical consensus — these should be considered alongside, not instead of, professional medical guidance.
Read Full DisclaimerReady to learn more?
Continue your journey through our classified biological research.
DISCUSSION ROOM
Members of THE COLLECTIVE discussing "The Oxalate Crisis: Kidney Stones and Beyond"
SILENT CHANNEL
Be the first to discuss this article. Your insight could help others understand these biological concepts deeper.
THE ARSENAL
Based on NHS Misdiagnosis Patterns — products curated by our research team for educational relevance and biological support.

Panaceum – Prebiotic Oligosaccharide Complex
INNERSTANDING may earn a commission on purchases made through these links. All products are selected based on rigorous educational relevance to our biological research.
RABBIT HOLE
Follow the biological thread deeper