The Role of Bile Acids in Lipid Homeostasis
Bile acids are not just digestive aids but powerful signaling molecules that regulate cholesterol levels. This article explores the liver-gut axis and its role in maintaining a healthy lipid profile.

# The Role of Bile Acids in Lipid Homeostasis: The Endocrine Master Switch
Overview
For decades, the mainstream medical narrative has relegated bile acids (BAs) to the status of mere digestive detergents. In the standard textbook view, bile is a greenish-yellow fluid produced by the liver, stored in the gallbladder, and secreted into the small intestine to emulsify dietary fats. While this is mechanically true, it represents a profound oversimplification that has hindered our understanding of metabolic health.
Recent breakthroughs in molecular biology and endocrinology have revealed that bile acids are, in fact, powerful hormone-like signaling molecules. They act as the primary rheostat for lipid homeostasis, governing not only the absorption of fats but the synthesis, transport, and excretion of cholesterol. Through the activation of specific nuclear and G protein-coupled receptors, bile acids communicate between the gut, the liver, and the systemic circulation, forming what we now recognise as the liver-gut-microbiome axis.
This article serves as a deep dive into the clandestine world of bile acid signaling. We will explore how these molecules dictate the fate of cholesterol, how environmental toxins are sabotaging this ancient biological system, and why the current pharmacological obsession with lowering LDL-cholesterol via statins may be ignoring the more fundamental issue of biliary stasis and receptor dysregulation. To understand lipid homeostasis, one must first understand the fluid that carries the lifeblood of our metabolism: bile.
---
The Biology — How It Works

Glytamins Suppositories – Specialist Suppository Formula
A practitioner-strength suppository designed to support liver and gallbladder health by bypassing the digestive system for maximum absorption. This formula uses targeted amino acids and botanicals to assist the body's natural bile production and detoxification pathways.
Vetting Notes
Pending
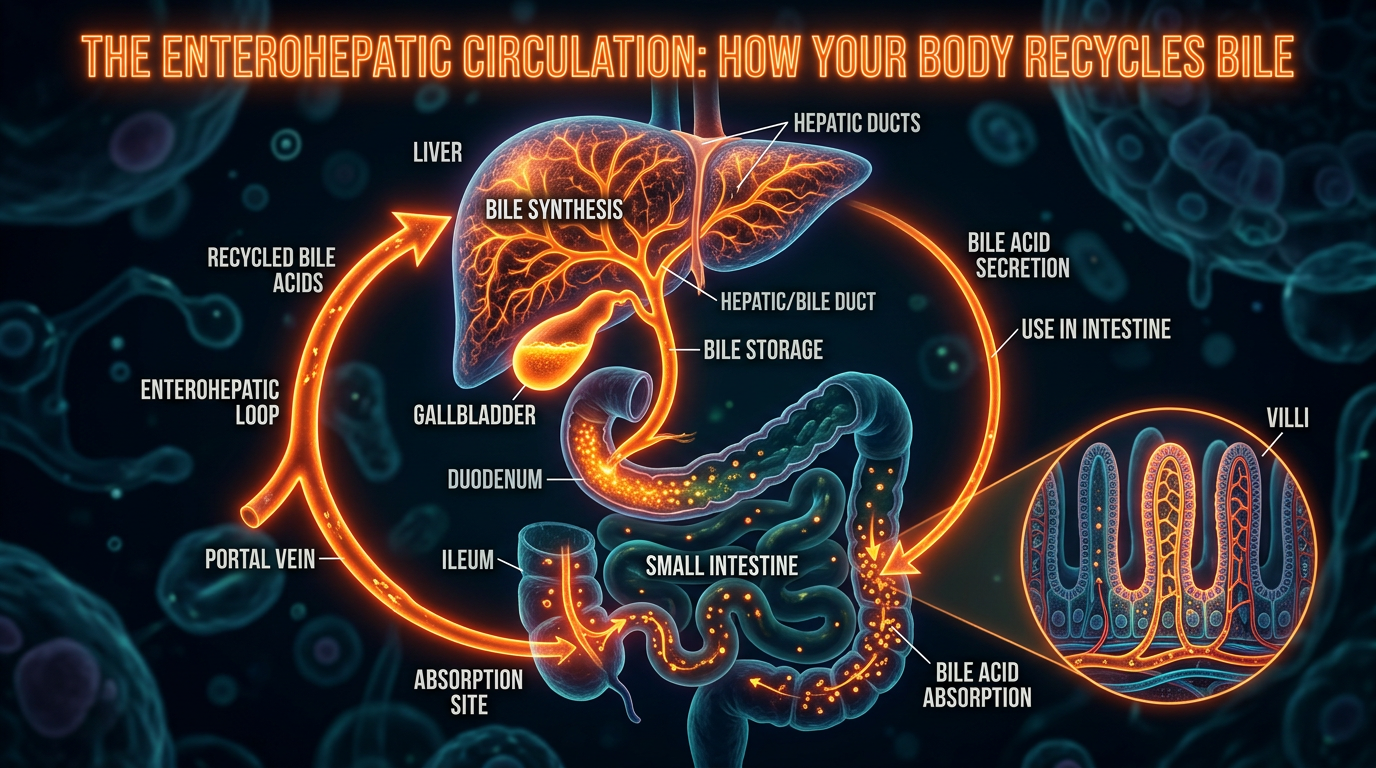
The lifecycle of a bile acid is a masterpiece of biological recycling, known as enterohepatic circulation. This process ensures that the body maintains a constant pool of BAs while minimising the energy-intensive process of *de novo* synthesis.
Primary vs. Secondary Bile Acids
Bile acid synthesis occurs exclusively in the hepatocytes (liver cells). The precursor for all bile acids is cholesterol. This is a vital point: the primary pathway for the elimination of excess cholesterol from the human body is its conversion into bile acids.
- —Primary Bile Acids: These are synthesized directly from cholesterol. The two main types in humans are Cholic Acid (CA) and Chenodeoxycholic Acid (CDCA).
- —Conjugation: Before secretion, these acids are "conjugated" with amino acids, usually glycine or taurine. This step is crucial because it renders them water-soluble and less toxic to the biliary membranes, forming what we call "bile salts."
- —Secondary Bile Acids: Once bile enters the intestines, the resident microbiota take over. Bacterial enzymes (specifically bile acid hydrolases) deconjugate and dehydroxylate the primary acids. This transforms CDCA into Lithocholic Acid (LCA) and CA into Deoxycholic Acid (DCA).
The Enterohepatic Loop
The efficiency of the body is staggering. Approximately 95% of the bile acids secreted into the duodenum are reabsorbed in the terminal ileum (the final section of the small intestine). They are then transported back to the liver via the portal vein.
Fact: The human bile acid pool (approx. 3–5 grams) cycles between 4 to 12 times per day. Only about 0.5 grams are lost in the faeces daily, which is the exact amount the liver must synthesise to maintain balance.
Solubilisation and Micelle Formation
The primary mechanical role of bile is the formation of mixed micelles. Because fats are hydrophobic (water-fearing), they cannot be absorbed in the aqueous environment of the gut. Bile acids act as amphipathic molecules—possessing both a water-loving and a fat-loving side. They surround lipid droplets, breaking them down into tiny micelles that allow pancreatic lipases to digest triglycerides and enable the absorption of fat-soluble vitamins (A, D, E, and K).
---
Mechanisms at the Cellular Level
To appreciate the role of BAs in lipid homeostasis, we must look at the specific receptors they activate. This is where bile acids transition from detergents to master regulators.
The Farnesoid X Receptor (FXR)
The Farnesoid X Receptor (FXR) is a nuclear receptor found in high concentrations in the liver and intestines. It is the "sensor" for bile acid levels. When BA levels are high, they bind to FXR, triggering a cascade that protects the liver from toxicity and regulates lipid levels.
- —Inhibition of Synthesis: Activated FXR induces the expression of SHP (Small Heterodimer Partner). SHP, in turn, inhibits CYP7A1 (cholesterol 7α-hydroxylase), the rate-limiting enzyme that converts cholesterol into bile acids. This is a classic negative feedback loop.
- —Lipid Metabolism: FXR activation reduces the synthesis of triglycerides by inhibiting SREBP-1c, a master transcription factor for lipogenesis.
- —Transport: FXR promotes the expression of export pumps (like BSEP) that push bile out of the liver, preventing "intrahepatic cholestasis" (bile backup).
TGR5: The Metabolic Trigger
While FXR lives in the nucleus, TGR5 is a G protein-coupled receptor located on the cell membrane. It is particularly sensitive to secondary bile acids like LCA and DCA.
- —Energy Expenditure: TGR5 activation in brown adipose tissue increases the conversion of inactive thyroid hormone (T4) to active T3, boosting the metabolic rate.
- —Glucose Control: In the gut, TGR5 triggers the release of GLP-1 (Glucagon-like peptide-1). This enhances insulin secretion and improves glucose tolerance, linking bile acid flow directly to the prevention of Type 2 Diabetes.
FGF15/19: The Inter-Organ Messenger
When BAs activate FXR in the intestine, the enterocytes produce a hormone called FGF19 (FGF15 in rodents). This hormone travels through the blood back to the liver, where it acts as a potent signal to stop bile acid production and facilitate gallbladder filling. This gut-liver axis communication is essential for maintaining the "rhythm" of lipid processing.
---
Environmental Threats and Biological Disruptors
The modern world is an obstacle course for bile acid metabolism. We are currently witnessing a silent epidemic of biliary dysregulation caused by exogenous factors that the mainstream medical establishment largely ignores.
The Glyphosate Impact
The herbicide glyphosate is perhaps the most significant disruptor of the liver-gut axis. While marketed as safe for humans because we lack the "shikimate pathway," this pathway exists in our gut bacteria. Glyphosate decimates the beneficial bacteria responsible for converting primary bile acids into secondary ones.
Statistic: Research indicates that glyphosate exposure can lead to a significant decrease in the diversity of the *Firmicutes* phylum, which are key players in bile acid deconjugation.
Without the correct bacterial balance, the signaling through TGR5 and FXR is muted, leading to a "sluggish" metabolism and the accumulation of primary bile acids that can become inflammatory in high concentrations.
Ultra-Processed Foods (UPFs) and Emulsifiers
The modern diet is loaded with synthetic emulsifiers (like carboxymethylcellulose and polysorbate 80). These compounds interfere with the natural micellar structure formed by bile acids. Furthermore, high-fructose corn syrup—a staple of UPFs—is a direct driver of De Novo Lipogenesis (DNL) in the liver. This floods the system with triglycerides that the bile acid pool struggles to manage, leading to "fatty liver" or MASLD (Metabolic Dysfunction-Associated Steatotic Liver Disease).
Microplastics and Endocrine Disruptors
BPA and phthalates, found in plastic packaging and water supplies, act as xenoestrogens. High oestrogen levels are known to inhibit bile flow (cholestasis). This is why gallbladder issues are statistically more common in women and during pregnancy. Microplastics also provide a surface for pathogenic bacteria to colonise in the gut, further disrupting the secondary bile acid profile.
---
The Cascade: From Exposure to Disease
When bile acid signaling fails, the result is not just a "stomach ache"—it is a systemic metabolic collapse. The cascade usually follows a predictable, yet devastating, path.
Stage 1: Subclinical Cholestasis
The process begins with "thick" or "sluggish" bile. This is often caused by a lack of taurine or phosphatidylcholine, the two substances required to keep bile fluid. When bile becomes viscous, it cannot flow freely. Cholesterol, which is supposed to be kept in solution by bile salts, begins to crystallize, eventually forming gallstones.
Stage 2: Impaired Cholesterol Clearance
If bile flow is restricted, the liver’s primary "exhaust pipe" for cholesterol is blocked. The liver, sensing a backup, downregulates LDL receptors. This causes LDL-cholesterol to circulate longer in the bloodstream, where it becomes susceptible to oxidation. It is not the presence of LDL that is the problem; it is the stagnation of LDL due to poor biliary clearance.
Stage 3: Dysbiosis and Endotoxaemia
Bile is a potent antimicrobial. One of its "hidden" jobs is to keep the small intestine relatively sterile. When bile flow is low, bacteria from the colon can migrate upward, leading to SIBO (Small Intestinal Bacterial Overgrowth).
Important Fact: Bile acids neutralise Lipopolysaccharides (LPS)—highly inflammatory endotoxins produced by Gram-negative bacteria. Low bile flow allows LPS to enter the bloodstream (leaky gut), triggering systemic inflammation and insulin resistance.
Stage 4: Atherosclerosis and Metabolic Syndrome
The final stage of the cascade is the deposition of oxidised lipids into the arterial walls. Because BA signaling through FXR and TGR5 is compromised, the body remains in a state of chronic low-level inflammation. The "lipid profile" becomes deranged (high triglycerides, low HDL, small dense LDL), but these are merely the symptoms of a failed liver-gut axis.
---
What the Mainstream Narrative Omits
The current healthcare paradigm treats lipid issues with a "reductionist" approach. If cholesterol is high, the answer is a statin. While statins inhibit the HMG-CoA reductase enzyme to reduce cholesterol synthesis, they do nothing to address the clearance or signaling of bile.
The Gallbladder "Uselessness" Myth
Surgery to remove the gallbladder (cholecystectomy) is one of the most common procedures in the UK and US. Patients are often told they "don't need" their gallbladder. This is scientifically inaccurate. Without a gallbladder, bile constantly trickles into the intestine rather than being delivered in a concentrated bolus during a meal. This leads to:
- —Malabsorption of fat-soluble vitamins.
- —Constant irritation of the intestinal lining.
- —Altered gut microbiome profiles.
- —Increased risk of colon cancer due to the constant presence of secondary bile acids.
The Cholesterol Phobia
Mainstream medicine views cholesterol as a "poison." In reality, cholesterol is the precursor to Vitamin D, oestrogen, testosterone, and cortisol. By focusing solely on suppressing cholesterol production, we ignore the vital role of bile acid flux. A healthy body doesn't need *low* cholesterol; it needs *flowing* cholesterol.
The Suppression of Bile Acid Sequestrants
In the 1970s and 80s, bile acid sequestrants (like Cholestyramine) were the primary treatment for high cholesterol. They work by binding to bile acids in the gut and forcing their excretion, which in turn forces the liver to use up more cholesterol to make new bile. While effective, they were largely pushed aside for statins, which are more profitable and easier for patients to take. However, sequestrants addressed the "exhaust" end of the system, whereas statins address the "factory" end.
---
The UK Context
In the United Kingdom, the burden of metabolic disease is reaching a breaking point. The NHS spends billions annually treating the complications of cardiovascular disease and Type 2 Diabetes.
The "British Diet" and Biliary Health
The UK population has one of the highest consumptions of ultra-processed foods in Europe. The lack of "bitter" foods in the modern British palate is particularly concerning. Historically, the British diet included bitter herbs and foraged greens, which are natural choleretics (substances that stimulate bile production). Today, the dominance of sweet and salty "beige" foods has led to a population with chronically under-stimulated biliary systems.
NHS Guidelines and Missing Diagnostics
Standard NHS blood panels measure ALT, AST (liver enzymes), and a basic lipid profile. However, Bile Acid Tests are rarely performed unless a woman is pregnant (screening for obstetric cholestasis) or a patient has severe liver failure.
Note: Many UK patients suffering from "IBS" are actually suffering from Bile Acid Malabsorption (BAM), a condition where the ileum fails to reabsorb BAs, leading to chronic diarrhoea. It is estimated that 1 in 3 people diagnosed with IBS-D actually have BAM.
The Pesticide Regulatory Landscape
Post-Brexit, the UK's regulation of pesticides like glyphosate remains a point of contention. While some EU nations have moved toward bans, the UK has largely maintained current usage levels. This ensures that the environmental disruption of the British gut-liver axis will continue for the foreseeable future unless individual action is taken.
---
Protective Measures and Recovery Protocols
Restoring lipid homeostasis requires a multifaceted approach that goes beyond "low-fat" dieting. In fact, low-fat diets can worsen biliary stasis because bile is only secreted in response to dietary fat.
1. Re-establishing Bile Flow
To fix the lipid profile, we must get the bile moving. This is known as cholagogue therapy.
- —Bitter Herbs: Dandelion root, artichoke leaf, and milk thistle stimulate the gallbladder and liver. Consuming these 15–20 minutes before a meal "primes" the system.
- —Taurine and Glycine: These amino acids are essential for bile acid conjugation. Taurine, in particular, has been shown to improve the solubility of bile and prevent stone formation.
- —Phosphatidylcholine (PC): Bile is composed of bile salts, cholesterol, and phospholipids. PC is the primary phospholipid in bile. Supplementing with PC helps thin the bile and prevent "sludge."
2. Microbiome Restoration
Since the microbiome controls the production of secondary bile acids (the ones that activate TGR5), gut health is paramount.
- —Fibre (The Sequestrant): Soluble fibre (like psyllium husk or glucomannan) acts as a natural bile acid sequestrant. It binds to old, toxic bile acids and carries them out of the body, forcing the liver to manufacture fresh bile from circulating cholesterol.
- —Polyphenols: Foods high in polyphenols (blueberries, dark chocolate, green tea) promote the growth of *Akkermansia muciniphila*, a bacterium that plays a role in metabolic signaling.
3. Molecular Support: TUDCA
Tauroursodeoxycholic Acid (TUDCA) is a hydrophilic bile acid that has been used in Chinese medicine for centuries. Modern research shows it is incredibly neuroprotective and hepatoprotective. It helps to resolve "ER stress" (Endoplasmic Reticulum stress) in the liver, which is a core driver of insulin resistance and poor lipid handling.
4. Environmental Mitigation
- —Water Filtration: Use high-quality filters (reverse osmosis or distillation with remineralisation) to remove fluoride, microplastics, and pesticide residues.
- —Avoid "The Big Three": Fructose, seed oils (high in linoleic acid), and glyphosate-treated grains. Seed oils are particularly problematic as they incorporate into the cell membranes of the biliary tree, making them more susceptible to oxidative damage.
5. Intermittent Fasting and Circadian Alignment
Bile acid synthesis follows a circadian rhythm. Eating late at night disrupts the FXR signaling pathways. Intermittent fasting allows the gallbladder to rest and concentrate bile, ensuring a potent "flush" when the first meal is consumed the following day.
---
Summary: Key Takeaways
The path to true lipid homeostasis is not found in a statin bottle, but in the fluid dynamics of the liver and the signaling of the gut.
- —Bile acids are hormones: They regulate more than just digestion; they control energy expenditure, glucose levels, and cholesterol clearance via receptors like FXR and TGR5.
- —Cholesterol is not the enemy: High cholesterol is often a symptom of biliary stasis—the body's inability to "flush" lipids through the gut-liver axis.
- —Environmental toxins are key disruptors: Pesticides like glyphosate and synthetic emulsifiers break the delicate feedback loops that maintain metabolic health.
- —Bitters and Fibre are essential: To maintain a healthy lipid profile, one must consume bitter compounds to stimulate flow and fibre to ensure the excretion of toxic bile.
- —The UK faces a unique crisis: The combination of a highly processed diet and a medical system that ignores biliary signaling has created a "perfect storm" of metabolic disease.
By shifting our perspective from "lowering cholesterol" to "optimising bile acid signaling," we can unlock a new level of biological resilience. The liver is the laboratory of the body, and bile is its most important chemical product. It is time we treated it with the scientific respect it deserves.
This article is provided for informational and educational purposes only. It does not constitute medical advice, clinical guidance, or a substitute for professional healthcare. Information reflects cited research at time of publication. Always consult a qualified healthcare professional before acting on any health information.
RESEARCH FOUNDATIONS
Biological Credibility Archive
Bile acids act as signaling molecules via the farnesoid X receptor to coordinate the homeostatic regulation of lipid and glucose metabolism.
The endocrine axis involving FGF15/19 is triggered by bile acids in the intestine to suppress hepatic bile acid synthesis and modulate lipid levels.
Bile acid synthesis through the classical pathway is the primary mechanism for cholesterol catabolism in the liver.
The gut microbiota regulates bile acid composition which in turn influences systemic lipid profiles and energy homeostasis through various receptors.
Bile acids facilitate the emulsification and absorption of dietary lipids while acting as metabolic sensors that maintain whole-body lipid balance.
Citations provided for educational reference. Verify via PubMed or institutional databases.
Medical Disclaimer
The information in this article is for educational purposes only and does not constitute medical advice, diagnosis, or treatment. Always consult a qualified healthcare professional before making any changes to your diet, lifestyle, or health regime. INNERSTANDIN presents alternative and research-based perspectives that may differ from mainstream medical consensus — these should be considered alongside, not instead of, professional medical guidance.
Read Full DisclaimerReady to learn more?
Continue your journey through our classified biological research.
DISCUSSION ROOM
Members of THE COLLECTIVE discussing "The Role of Bile Acids in Lipid Homeostasis"
SILENT CHANNEL
Be the first to discuss this article. Your insight could help others understand these biological concepts deeper.
THE ARSENAL
Based on Cholesterol & Lipid Science — products curated by our research team for educational relevance and biological support.
Glytamins Suppositories – Specialist Suppository Formula

C60 Charcoal – Supports Healthy Digestion and Detoxification.

Glutathione Builder – Advanced Amino Acid Formula
INNERSTANDING may earn a commission on purchases made through these links. All products are selected based on rigorous educational relevance to our biological research.
RABBIT HOLE
Follow the biological thread deeper