Thyroid Dysfunction and Thinning: The Metabolic Foundation of Hair Density
Both hypo- and hyperthyroidism significantly alter the rate of hair growth and the duration of the anagen phase. We detail the necessary tests to ensure your thyroid is supporting your follicles.
Overview
In the hierarchy of human survival, hair is an evolutionary luxury. When the body faces physiological stress, nutrient scarcity, or metabolic dysfunction, it systematically reallocates resources away from non-essential peripheral tissues to protect the vital organs—the heart, brain, and liver. At the centre of this resource allocation sits the thyroid gland, a small, butterfly-shaped organ in the neck that acts as the body’s metabolic thermostat.
Thyroid dysfunction is not merely a "hormonal imbalance"; it is a systemic failure of energy production that manifests visibly through the health and density of the hair. For many in the UK, thinning hair, a receding hairline, or a loss of the outer third of the eyebrows are the first outward signals of a metabolic engine that is stalling. Yet, the mainstream medical approach frequently ignores these early warning signs, relying on archaic testing parameters that fail to capture the nuances of thyroid health.
At INNERSTANDING, we recognise that hair density is a profound bio-indicator. To understand why hair thins, we must look beyond the scalp and into the cellular furnace of the thyroid. This article explores the intricate relationship between thyroid hormones and the hair follicle, exposing the metabolic foundations of hair growth and detailing the environmental and systemic hurdles that prevent millions of Britons from achieving optimal follicular health.
UK FACT: It is estimated that 1 in 20 people in the United Kingdom live with a thyroid condition, though many remain undiagnosed. Women are six times more likely than men to develop thyroid problems, often experiencing significant hair thinning as their primary symptom.
The Biology — How It Works

Lugol’s Iodine – Hormonal Issues, Menopause, Immune System, Brain Fog, Memory, Thyroid, Dry Skin
A high-potency 12% Lugol’s Iodine solution designed to support thyroid health, metabolic energy, and cognitive clarity. This traditional aqueous blend provides both iodine and potassium iodide to ensure your body has the essential elements needed for hormonal balance and healthy skin.
Vetting Notes
Pending
The hair follicle is one of the most metabolically active structures in the human body. To produce a single strand of hair, the follicle must engage in rapid cellular proliferation, a process that requires a constant and abundant supply of Adenosine Triphosphate (ATP)—the body’s energy currency. This energy production is governed almost entirely by thyroid hormones.
The HPT Axis and Hormone Production
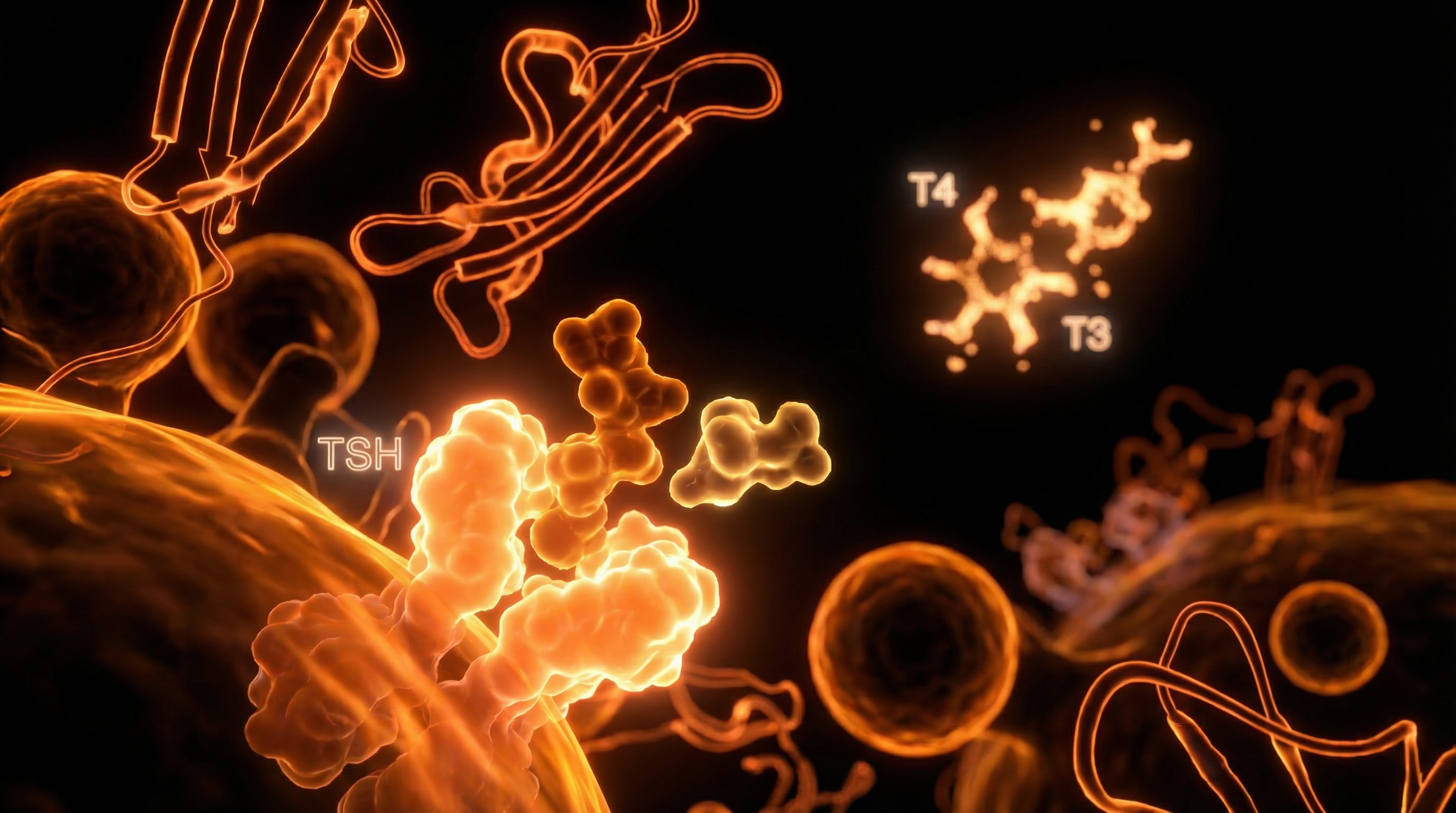
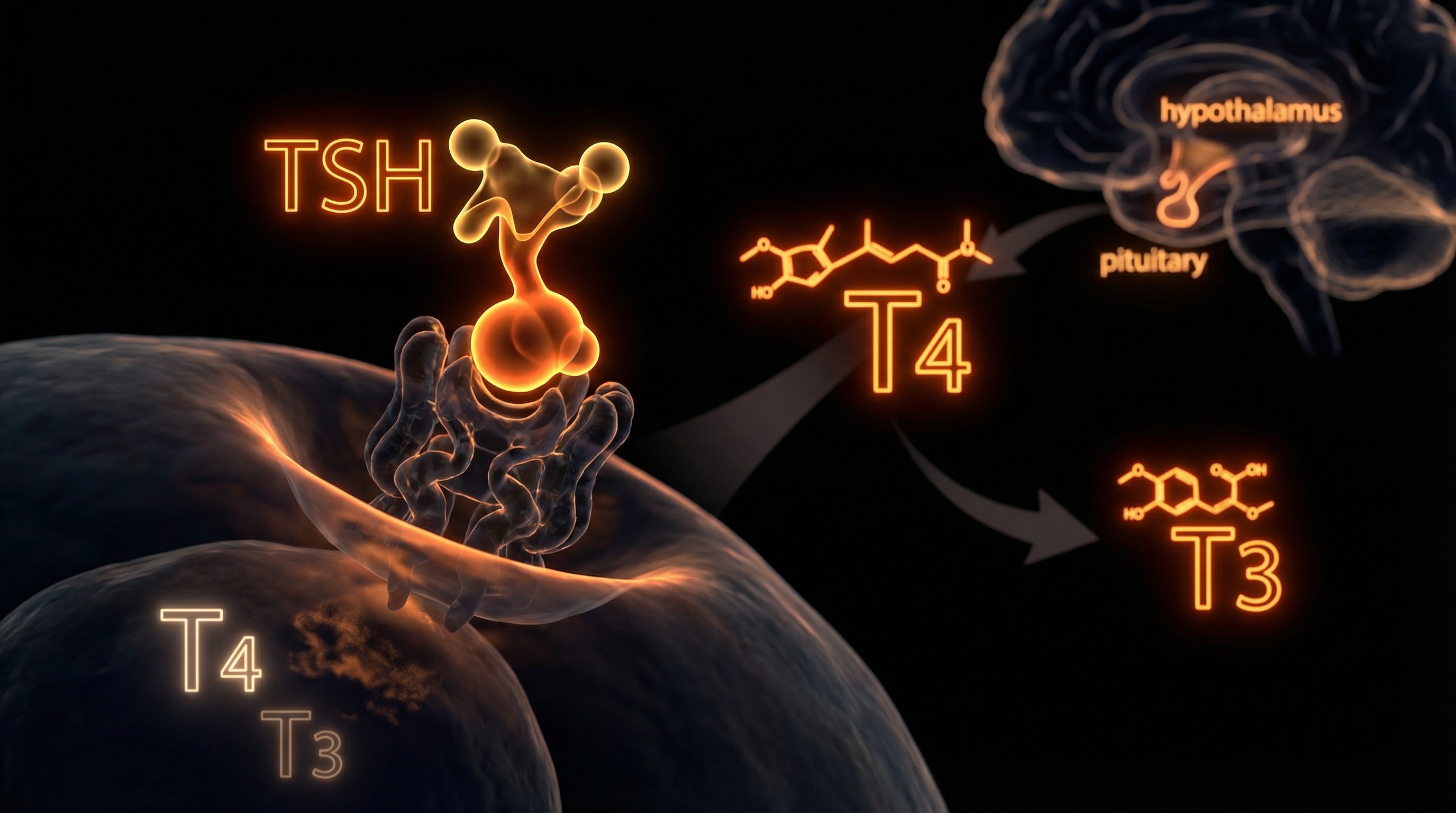
The process begins in the brain. The hypothalamus releases Thyrotropin-Releasing Hormone (TRH), which signals the pituitary gland to secrete Thyroid-Stimulating Hormone (TSH). TSH then prompts the thyroid gland to produce two primary hormones: Thyroxine (T4) and Triiodothyronine (T3).
- —T4 (Thyroxine): Produced in larger quantities, T4 is largely a "pro-hormone." It is relatively inactive and must be converted into T3 to be used by the cells.
- —T3 (Triiodothyronine): This is the biologically active form. Every cell in the body, including those within the hair follicle, has receptors for T3.
The conversion of T4 to T3 primarily occurs in the liver, kidneys, and peripheral tissues, including the skin. If this conversion is impaired—due to stress, nutrient deficiencies, or liver toxicity—the hair follicles will starve for energy, regardless of how much T4 is circulating in the blood.
The Hair Growth Cycle
To understand the impact of the thyroid, one must understand the three stages of the hair cycle:
- —Anagen (Growth Phase): This phase lasts 2 to 7 years. Cells in the root of the hair divide rapidly.
- —Catagen (Transition Phase): A short period where the hair follicle shrinks and detaches from the dermal papilla.
- —Telogen (Resting Phase): The hair is dormant for about 3 months before eventually falling out to be replaced by new anagen growth.
Thyroid hormones are essential for initiating and maintaining the anagen phase. When T3 levels are optimal, the duration of the anagen phase is maximised, leading to long, thick hair. When T3 levels drop (Hypothyroidism) or fluctuate wildly (Hyperthyroidism), the body prematurely triggers the telogen phase. This results in "Telogen Effluvium"—a condition where a large percentage of hairs enter the shedding phase simultaneously.
Mechanisms at the Cellular Level
The influence of thyroid hormones on the hair follicle is direct and profound. Scientific literature has confirmed that human hair follicles are direct targets of thyroid hormones. Both T3 and T4 modulate the function of the Dermal Papilla Cells (DPCs) and the Outer Root Sheath (ORS) keratinocytes.
Mitochondrial Respiration and ATP
The "Metabolic Foundation" mentioned in our title refers to mitochondrial function. T3 enters the mitochondria of the hair follicle cells and stimulates the expression of genes involved in energy production. Without sufficient T3, the mitochondria become sluggish. In the context of the follicle, this means the matrix cells cannot divide at the rate required to sustain hair shaft production. The result is a thinner hair diameter (miniaturisation) and a weakened hair shaft that is prone to breakage.
Keratin Synthesis
Hair is primarily composed of keratin, a fibrous structural protein. Thyroid hormones regulate the synthesis of keratinocytes. In a hypothyroid state, the production of these proteins slows down, leading to hair that feels dry, brittle, and "straw-like." Furthermore, thyroid hormones influence the production of sebum—the natural oil that protects the hair. Low thyroid function leads to reduced sebum, causing the scalp to become dry and the hair to lose its lustre.
Pigmentation and Melanin
The thyroid also influences the melanocytes within the hair follicle. Chronic thyroid dysfunction is often linked to premature greying. When the metabolic rate drops, the oxidative stress within the follicle increases, damaging the melanocytes and halting the production of pigment.
UK FACT: Research suggests that nearly 15% of the UK population may possess elevated thyroid antibodies (TPOAb), indicating a subclinical autoimmune response that can disrupt hair follicle biology long before TSH levels fall out of the "standard" range.
Environmental Threats and Biological Disruptors
In the modern British environment, our thyroids are under constant assault. The decline in hair density across the population is not merely genetic; it is a response to an increasingly "thyro-toxic" world.
The Halogen Competition
The thyroid requires Iodine to produce T4 and T3. However, iodine belongs to a group of elements called halogens, which also include Fluoride, Chlorine, and Bromine. Because these elements are chemically similar, they compete for the same receptors in the thyroid gland.
- —Fluoride: Widely present in the UK's municipal water supply in certain regions (such as the West Midlands and North East), fluoride is a known goitrogen that displaces iodine, effectively "shutting down" hormone production.
- —Bromine: Often used as a flame retardant in British furniture and as a dough conditioner in commercial bread (though less common in the UK than the US, it is still present in various processed foods).
Endocrine Disrupting Chemicals (EDCs)
The UK’s reliance on processed foods and plastic packaging exposes the population to Bisphenol A (BPA) and Phthalates. These chemicals mimic oestrogen and can interfere with the transport of thyroid hormones in the blood. When oestrogen levels are "dominantly" high—a common issue in the UK due to environmental exposure and sedentary lifestyles—the liver produces more Thyroid Binding Globulin (TBG). This protein "mops up" free thyroid hormones, making them unavailable to the hair follicles.
Heavy Metal Accumulation
Mercury (from dental amalgams and certain fish) and Aluminium (from deodorants and cookware) interfere with the enzymes (deiodinases) responsible for converting T4 into the active T3. For the UK resident, the cumulative "toxic load" often explains why hair thinning persists despite a "clean" diet.
The Cascade: From Exposure to Disease
The journey from a healthy head of hair to diffuse thinning is rarely a sudden event; it is a slow metabolic cascade.
- —The Stress Trigger: It begins with chronic stress—physical, emotional, or environmental. This elevates cortisol.
- —Conversion Blockage: High cortisol inhibits the 5'-deiodinase enzyme. Instead of converting T4 into active T3, the body begins producing Reverse T3 (rT3).
- —Metabolic Hibernation: rT3 is a metabolic "brake." It blocks the T3 receptors on the hair follicles, telling the body to conserve energy.
- —Follicular Shutdown: The hair follicles receive the signal that "winter is coming." They exit the anagen phase and enter telogen.
- —Diffuse Thinning: Within 3-6 months of this metabolic shift, the individual notices significant shedding. This is often accompanied by cold hands and feet, fatigue, and weight gain—the classic hypothyroid profile.
This cascade is particularly dangerous because it often occurs within the "normal" ranges of mainstream blood tests. A patient may have "normal" TSH but very high Reverse T3, meaning their hair is effectively in a state of starvation while their doctor tells them they are healthy.
UK FACT: Thyroid medications are among the most prescribed drugs in the UK. In 2020/21, there were over 32 million prescriptions for Levothyroxine (T4) in England alone, yet many patients continue to report ongoing symptoms like hair loss, indicating that T4-only monotherapy is failing to address the cellular metabolic need.
What the Mainstream Narrative Omits
The mainstream medical approach to thyroid health in the UK is, in our view, fundamentally flawed and decades behind current biological understanding.
The TSH Fallacy
The NHS standard for thyroid screening is the TSH test. The theory is that if TSH is high, the thyroid is low. However, TSH is a *pituitary* hormone, not a thyroid hormone. It is a lagging indicator. By the time TSH rises above the "normal" limit (often 4.0 or 5.0 mIU/L in the UK), the individual may have been suffering from cellular hypothyroidism and hair loss for years.
The "Normal" vs "Optimal" Trap
The "normal" range for thyroid markers is based on a statistical average of the population. Given that a significant portion of the UK population is metabolically unwell, being "average" is not the same as being "optimal."
- —Mainstream "Normal" TSH: 0.5 – 4.5 mIU/L
- —INNERSTANDING "Optimal" TSH: 0.5 – 2.0 mIU/L
Furthermore, the mainstream narrative almost entirely omits Free T3 testing. Since T3 is the only hormone the hair follicle can actually use, failing to test it is like checking the fuel in a car's tank but ignoring whether the engine can actually burn it.
The Overlook of Autoimmunity
Approximately 90% of hypothyroidism in developed nations like the UK is actually Hashimoto’s Thyroiditis, an autoimmune condition. The mainstream narrative treats Hashimoto’s the same as simple iodine deficiency—by giving T4. They ignore the immune system's attack on the thyroid, which creates systemic inflammation that further damages the hair follicles.
UK FACT: Iodine deficiency is re-emerging as a significant public health issue in the UK, particularly among women of childbearing age. The UK is now ranked among the top ten iodine-deficient nations in the developed world, directly impacting the nation's metabolic health and hair density.
The UK Context
The UK presents a unique set of challenges for thyroid and hair health. Our geography, agricultural practices, and healthcare structure create a "perfect storm" for metabolic dysfunction.
Soil Depletion and Selenium
The UK’s soil is notoriously low in Selenium, a vital mineral required for the conversion of T4 to T3 and for protecting the thyroid from oxidative damage. Without selenium, the deiodinase enzymes cannot function. While Brazil nuts are a famous source, the selenium content in food consumed in the UK has declined steadily over the last 50 years.
The Postcode Lottery of Care
Access to comprehensive thyroid testing in the UK is a "postcode lottery." Many GPs are restricted by local Integrated Care Board (ICB) guidelines that prevent them from ordering Free T3 or Antibody tests unless TSH is significantly abnormal. This leaves patients in a state of "subclinical" limbo—losing their hair and their vitality while being told their results are "satisfactory."
The Vitamin D Connection
Living in the UK means most residents are Vitamin D deficient for at least six months of the year. Vitamin D is not just a vitamin; it is a pro-hormone that modulates the immune system and supports thyroid hormone receptor sensitivity. Low Vitamin D is a known trigger for both hair loss and autoimmune thyroiditis.
Protective Measures and Recovery Protocols
Recovering your hair density requires a "Metabolic First" approach. You cannot "supplement" your way out of a thyroid problem with biotin alone; you must address the foundation.
Step 1: Comprehensive Testing
Demand a full thyroid panel. If your GP will not provide it, seek private functional testing. You need to know:
- —TSH: To see the pituitary's signal.
- —Free T4: To see what the thyroid is producing.
- —Free T3: To see what is available for your hair follicles.
- —Reverse T3: To see if stress is "braking" your metabolism.
- —TPO and TG Antibodies: To rule out Hashimoto's.
Step 2: Nutrient Optimisation
- —Iodine: Ensure adequate intake through sea vegetables or high-quality supplementation, but *only* after checking antibodies, as iodine can flare Hashimoto's.
- —Selenium: 200mcg per day to support T4 to T3 conversion.
- —Zinc: Essential for TSH production and for the structural integrity of the hair shaft.
- —Iron (Ferritin): Hair follicles require high levels of stored iron (ferritin) to stay in the anagen phase. Aim for a ferritin level of at least 70-100 ng/mL—much higher than the NHS "minimum" of 15-30.
Step 3: Environmental Detoxification
- —Filter your water: Use a filter that specifically removes fluoride and chlorine.
- —Clean Beauty: Switch to "green" personal care products to reduce exposure to phthalates and parabens that disrupt the thyroid.
- —Ditch the Non-Stick: Replace PFAS-laden non-stick pans with stainless steel or cast iron to prevent "forever chemicals" from interfering with hormone receptors.
Step 4: Circadian Rhythm and Stress
The thyroid is deeply tied to the light-dark cycle. Morning sunlight exposure helps regulate the HPT axis. Conversely, chronic blue light exposure at night elevates cortisol, which, as we have established, halts the production of active T3.
UK FACT: A study of UK dermatology patients found that nearly 60% of those presenting with diffuse hair loss had sub-optimal ferritin (iron store) levels below 50 ng/mL, coupled with "borderline" thyroid markers.
Summary: Key Takeaways
The density of your hair is a reflection of your internal metabolic state. To treat thinning hair as a superficial problem is to ignore the urgent message your body is sending you.
- —The Thyroid is the Master: T3 is the "spark plug" of the hair follicle; without it, the anagen (growth) phase cannot be sustained.
- —Mainstream Testing is Incomplete: A "normal" TSH does not mean your hair follicles are receiving the hormones they need. Always insist on Free T3 and Reverse T3.
- —The UK Environment is Challenging: Fluoridated water, selenium-poor soil, and Vitamin D deficiency create a significant metabolic burden for the British public.
- —Nutrients Matter: Hair density requires high levels of ferritin, selenium, zinc, and iodine.
- —Hair Loss is a Signal: Thinning is often the first sign of subclinical hypothyroidism. By addressing the metabolic foundation early, you can prevent the progression into full-scale disease.
At INNERSTANDING, we believe that true health education involves looking beneath the surface. Your hair is not just an aesthetic feature—it is a metabolic output. By supporting the thyroid, reducing environmental toxicity, and demanding comprehensive biological data, you can restore the metabolic foundation required for a lifetime of hair density and vitality.
*
"References & Technical Notes for the Researcher:"
- —*Inhibition of 5'-deiodinase by cortisol (The "Stress-Hair" link).*
- —*Follicular T3 receptor expression (The direct cellular mechanism).*
- —*The "Reference Range" controversy in British Endocrinology.*
- —*Halogen displacement theory (Fluoride vs. Iodine).*
- —*NHS Prescription data (Levothyroxine trends 2010-2023).*
This article is provided for informational and educational purposes only. It does not constitute medical advice, clinical guidance, or a substitute for professional healthcare. Information reflects cited research at time of publication. Always consult a qualified healthcare professional before acting on any health information.
RESEARCH FOUNDATIONS
Biological Credibility Archive
Thyroid hormones T3 and T4 have been shown to significantly prolong the anagen phase of the human hair cycle by stimulating keratinocyte proliferation and suppressing apoptosis.
Thyroid hormone signaling is essential for the metabolic activation of hair follicle stem cells, facilitating the transition from quiescent telogen to active growth.
Disruption of the thyroid hormone receptor pathway alters mitochondrial respiration in the hair follicle, resulting in impaired hair fiber production and reduced density.
Hypothyroidism causes diffuse hair loss and thinning by slowing the metabolic rate of matrix cells and increasing the ratio of telogen to anagen follicles.
Triiodothyronine stimulates the synthesis of glycosaminoglycans in the dermal papilla, which is crucial for maintaining the structural integrity and density of the hair shaft.
Citations provided for educational reference. Verify via PubMed or institutional databases.
Medical Disclaimer
The information in this article is for educational purposes only and does not constitute medical advice, diagnosis, or treatment. Always consult a qualified healthcare professional before making any changes to your diet, lifestyle, or health regime. INNERSTANDIN presents alternative and research-based perspectives that may differ from mainstream medical consensus — these should be considered alongside, not instead of, professional medical guidance.
Read Full DisclaimerReady to learn more?
Continue your journey through our classified biological research.
DISCUSSION ROOM
Members of THE COLLECTIVE discussing "Thyroid Dysfunction and Thinning: The Metabolic Foundation of Hair Density"
SILENT CHANNEL
Be the first to discuss this article. Your insight could help others understand these biological concepts deeper.
THE ARSENAL
Based on Hair Health & Follicle Biology — products curated by our research team for educational relevance and biological support.

Magnesium Blend – The Most Important Mineral
Rejuvenation Pack – Essential Vitamins and Minerals for Health Restoration

Magnesium L-Threonate
INNERSTANDING may earn a commission on purchases made through these links. All products are selected based on rigorous educational relevance to our biological research.
RABBIT HOLE
Follow the biological thread deeper