Vitamin D and Cholesterol: The Sterol Connection
Cholesterol is the precursor to Vitamin D, which is often deficient in the UK population. This article examines the biological trade-offs between cholesterol levels and sunlight-mediated hormone synthesis.
Overview
In the modern landscape of clinical medicine, few molecules have been as systematically vilified as cholesterol. For decades, the mainstream narrative has framed this vital sterol as a primary driver of cardiovascular pathology, leading to a global crusade to lower its levels through pharmaceutical intervention. However, this narrow perspective ignores a fundamental biological truth: cholesterol is the structural and functional foundation of human life. Nowhere is this more apparent than in its role as the direct precursor to Vitamin D—or more accurately, the secosteroid hormone Cholecalciferol.
The synthesis of Vitamin D is a magnificent display of biological alchemy, where the skin transforms a specific form of cholesterol into a potent master regulator of the human genome. Yet, in the modern era—particularly within the United Kingdom—this synthesis has been catastrophicly disrupted. We are currently witnessing a dual crisis: a widespread cultural "cholesterol phobia" and a profound epidemic of Vitamin D deficiency.
This article explores the "Sterol Connection," examining how the body prioritises the allocation of cholesterol and why the suppression of this molecule, combined with the lack of adequate ultraviolet radiation in northern latitudes, is driving a systemic collapse in public health. We will deconstruct the biological trade-offs inherent in hormone synthesis and expose why the conventional approach to lipid management may be inadvertently starving the body of its most powerful defensive hormone.
Fact: Vitamin D is not actually a vitamin; it is a secosteroid hormone. Unlike vitamins, which are cofactors for enzymes, Vitamin D acts as a transcription factor, directly influencing the expression of over 200 different genes in the human body.
---
The Biology — How It Works

Energy Blend Supports
Energy Blend is a comprehensive formula designed to fuel your body at a cellular level, promoting sustained physical stamina and mental clarity without synthetic spikes. It targets fundamental metabolic pathways to ensure your nervous system and hormonal activity remain balanced and resilient.
Vetting Notes
Pending
To understand the connection between cholesterol and Vitamin D, we must first look at the molecular architecture of the sterol family. Cholesterol is a waxy, fat-like substance that is essential for cell membrane integrity, bile acid production, and the synthesis of all steroid hormones, including cortisol, oestrogen, and testosterone.
The Precursor: 7-Dehydrocholesterol
The specific bridge between lipids and light is a molecule called 7-Dehydrocholesterol (7-DHC). This molecule is synthesised in the liver from cholesterol and then transported to the skin, specifically the keratinocytes and fibroblasts of the epidermis and dermis.
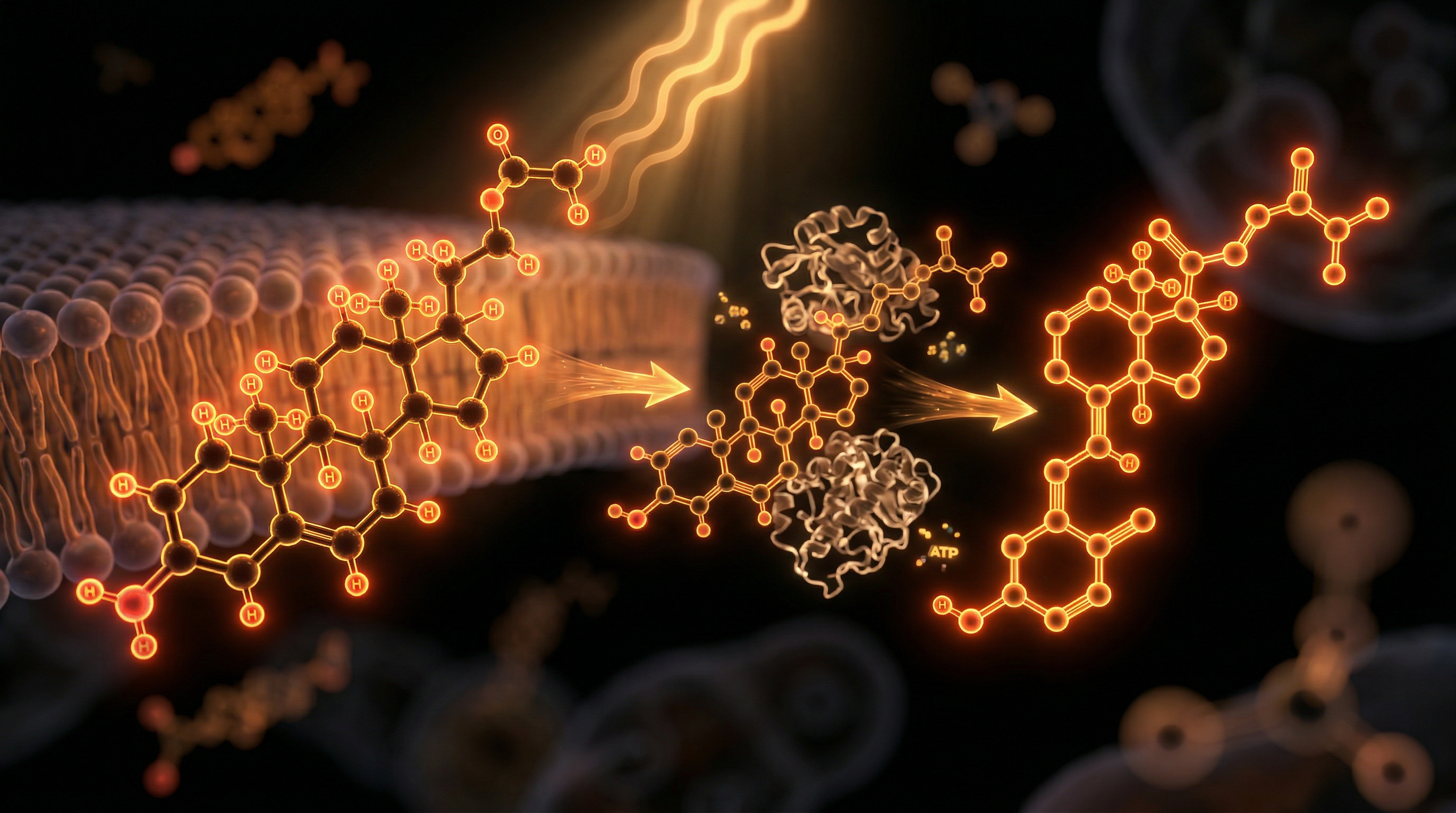
The Photolysis Process
When the skin is exposed to Ultraviolet B (UVB) radiation—specifically in the range of 290 to 315 nanometres—the energy from these photons breaks the "B-ring" of the 7-DHC molecular structure. This process, known as photolysis, converts 7-DHC into Pre-vitamin D3.
- —Thermal Isomerisation: Once Pre-vitamin D3 is formed, it undergoes a rapid, heat-dependent rearrangement (isomerisation) to become Vitamin D3 (Cholecalciferol).
- —Transport: Vitamin D3 is then ejected from the cell membranes into the extracellular space and enters the capillary bed, where it binds to the Vitamin D Binding Protein (VDBP) for transport to the liver.
The Dual Transformation
It is critical to note that Vitamin D3 is biologically inert when it first enters the bloodstream. It must undergo two successive hydroxylation steps to become active:
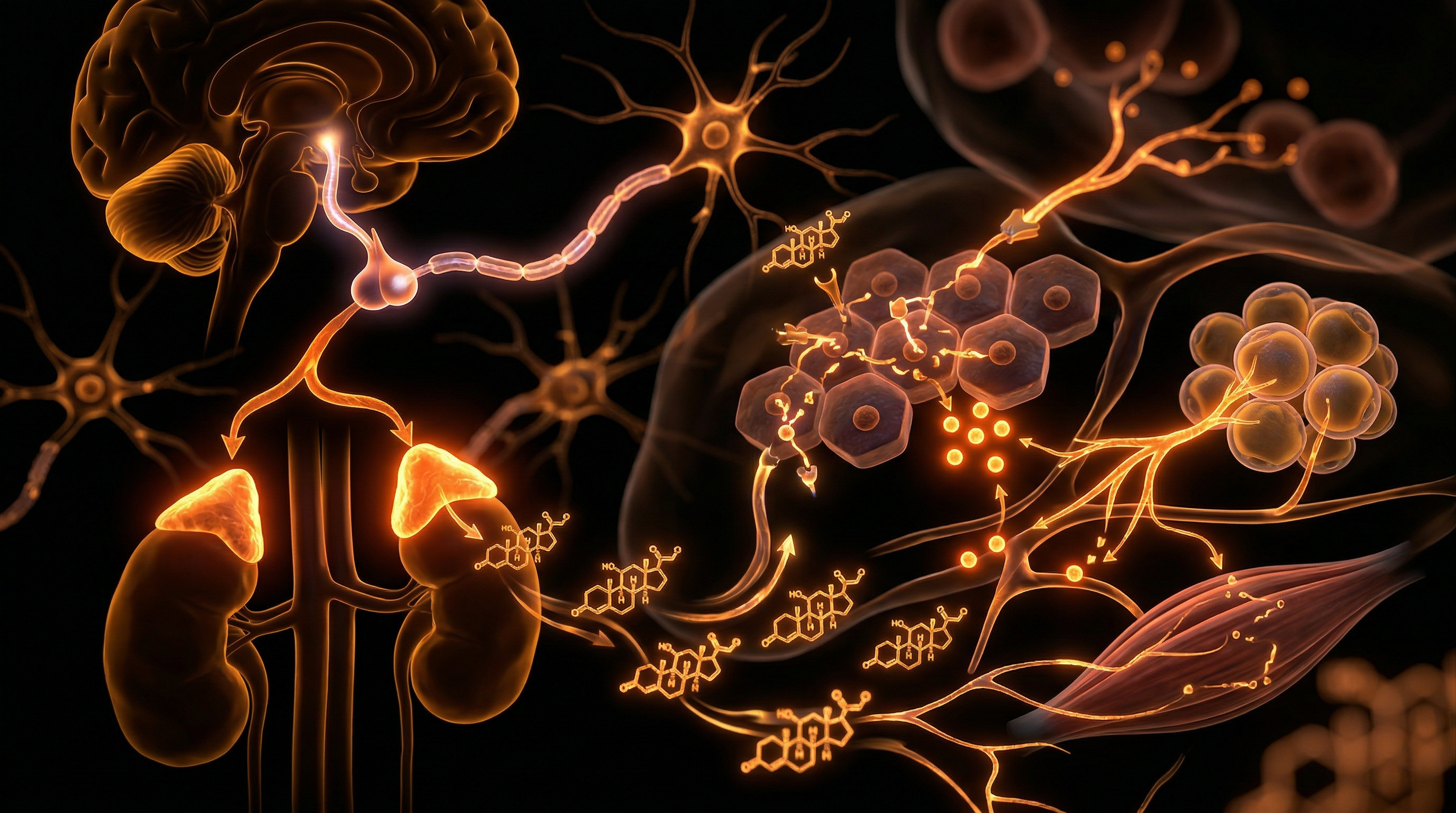
- —In the Liver: The enzyme CYP27A1 (or 25-hydroxylase) converts D3 into 25-hydroxyvitamin D [25(OH)D], also known as Calcifediol. This is the form measured in standard blood tests.
- —In the Kidneys: The enzyme CYP27B1 (1-alpha-hydroxylase) converts Calcifediol into the biologically active form: 1,25-dihydroxyvitamin D [1,25(OH)2D], also known as Calcitriol.
Fact: Without sufficient cholesterol levels in the skin to provide the 7-DHC substrate, the body cannot produce Vitamin D3, regardless of how much sunlight an individual is exposed to.
---
Mechanisms at the Cellular Level
The interplay between cholesterol and Vitamin D goes far deeper than mere synthesis. On a cellular level, these two molecules are part of a feedback loop that regulates metabolic health and immune function.
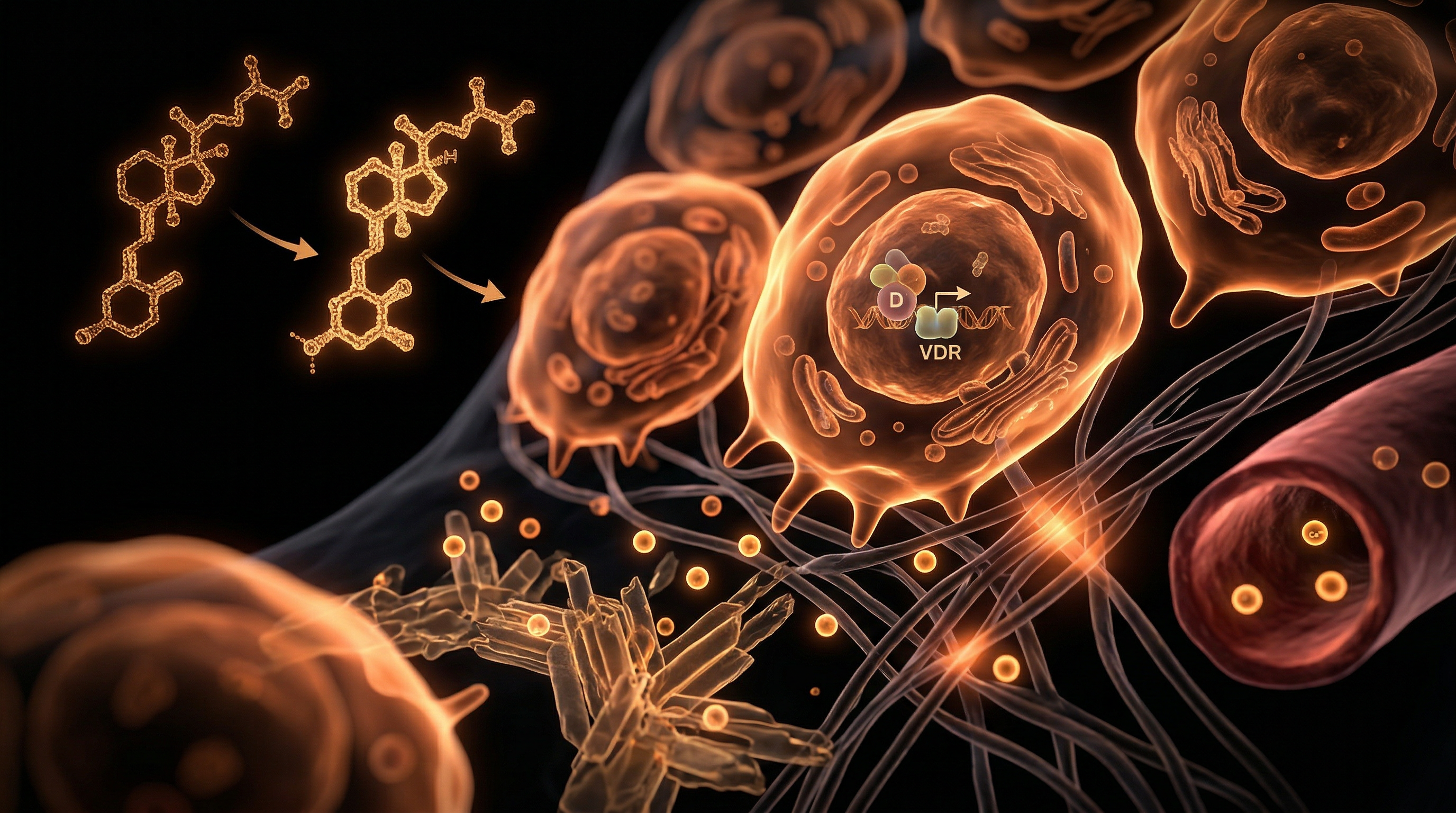
The Role of the VDR (Vitamin D Receptor)
Once Calcitriol is formed, it acts by binding to the Vitamin D Receptor (VDR), which is present in almost every cell in the body. The VDR is a nuclear receptor; when activated, it travels to the cell nucleus, pairs with the Retinoid X Receptor (RXR), and binds to specific DNA sequences known as Vitamin D Response Elements (VDREs).
This binding acts like a master switch, turning genes on or off. These genes control:
- —Calcium Homeostasis: Enhancing the absorption of calcium and phosphorus from the gut.
- —Cell Proliferation: Preventing the uncontrolled growth of cancer cells.
- —Immune Modulation: Optimising the "innate" immune system (macrophages and neutrophils) while calming the "adaptive" immune system to prevent autoimmunity.
Cholesterol as a "Buffer"
Interestingly, the body appears to use cholesterol levels as a compensatory mechanism. When Vitamin D levels are low, the body may upregulate cholesterol production in an attempt to provide more 7-DHC for potential synthesis. This suggests that "high cholesterol" in sun-deprived populations (like the UK) might not be a "disease" of overconsumption, but a biological adaptation to chronic UV starvation.
Enzymatic Competition
The enzymes that metabolise cholesterol (the Cytochrome P450 family) are the same enzymes responsible for the activation and deactivation of Vitamin D.
- —CYP24A1 is the enzyme responsible for breaking down excess Vitamin D.
- —If the body is under toxic stress or burdened by pharmaceutical drugs, these enzymes can become "hijacked," leading to a state where Vitamin D is degraded faster than it can be synthesised or utilised.
---
Environmental Threats and Biological Disruptors
In the modern world, the biological pathway from cholesterol to Vitamin D is under constant assault. We no longer live in the environment in which our physiology evolved, and the "Sterol Connection" is being severed by several key factors.
The Sunscreen Mythos
The most direct threat to Vitamin D synthesis is the pervasive use of high-SPF sunscreens. While marketed as a protective measure against skin cancer, SPF 30 sunscreen blocks approximately 95% to 98% of UVB radiation.
- —Because UVB is the only wavelength capable of cleaving the B-ring of 7-DHC, the use of sunscreen effectively shuts down the endogenous production of Vitamin D.
- —Paradoxically, while blocking UVB, many sunscreens allow UVA (which penetrates deeper and causes more oxidative damage) to pass through, potentially increasing the risk of melanoma while simultaneously inducing Vitamin D deficiency.
Air Pollution and Particulate Matter
In urban UK environments, air pollution acts as a secondary filter. Particulate matter, nitrogen dioxide, and ozone can scatter and absorb UVB photons before they reach ground level. This means that even on a "sunny" day in a city like London or Manchester, the UV Index may remain too low for effective Vitamin D synthesis.
The Blue Light Hazard and Indoor Living
Humanity has moved indoors. We spend 90% of our time under artificial lighting, which is dominated by high-energy visible (HEV) blue light and lacks the full spectrum of the sun.
- —Window Glass: Standard window glass blocks 100% of UVB radiation. You cannot produce Vitamin D by sitting behind a window, even in direct sunlight.
- —Circadian Mismatch: Lack of morning sunlight (Infrared and Red light) makes the skin more susceptible to damage from the midday UV rays, as the skin uses the morning spectrum to "prime" its antioxidant defences.
Biological Disruptors: Glyphosate and Statins
- —Statins: These drugs inhibit HMG-CoA reductase, the rate-limiting enzyme in cholesterol synthesis. By lowering total cholesterol, statins directly reduce the availability of 7-DHC in the skin.
- —Glyphosate: The most widely used herbicide in UK agriculture has been shown to interfere with Cytochrome P450 enzymes. By disrupting these enzymes, glyphosate impairs the liver's ability to hydroxylate Vitamin D into its active form.
Callout: A 2013 study suggested that the "epidemic" of Vitamin D deficiency in the West may be partially linked to the massive increase in glyphosate residue in the food supply, which prevents the liver from processing the "vitamin" correctly.
---
The Cascade: From Exposure to Disease
When the cholesterol-Vitamin D pathway is compromised, the body enters a state of systemic disharmony. This is not just about "weak bones"; it is a total metabolic collapse.
Metabolic Syndrome and Insulin Resistance
Vitamin D is a key regulator of insulin secretion by the pancreas. When levels fall, insulin sensitivity drops. Furthermore, because cholesterol is not being converted into Vitamin D, the liver may become congested with excess lipids, contributing to Non-Alcoholic Fatty Liver Disease (NAFLD).
The Immune System "Firestorm"
Without the modulating effect of Calcitriol, the immune system loses its "regulatory T-cells" (Tregs).
- —Autoimmunity: The body begins to attack itself (Multiple Sclerosis, Rheumatoid Arthritis, Hashimoto’s).
- —Cytokine Storms: In the absence of Vitamin D, the body is prone to hyper-inflammatory responses to viral infections—a phenomenon observed clearly during the COVID-19 pandemic.
Cardiovascular Consequences
The mainstream view is that high cholesterol causes heart disease. However, the reality is more nuanced. Vitamin D inhibits the calcification of arteries.
- —When Vitamin D is low, the body cannot properly manage calcium. Instead of going into the bones, calcium is deposited in the soft tissues and arterial walls.
- —High cholesterol *combined* with low Vitamin D is a recipe for atherosclerosis. If Vitamin D levels were optimal, the body could handle higher levels of circulating cholesterol without the risk of plaque formation.
Mental Health and the "Winter Blues"
Vitamin D regulates the enzyme Tryptophan Hydroxylase 2 (TPH2), which converts the amino acid tryptophan into serotonin in the brain.
- —Low Vitamin D = Low Serotonin.
- —This explains why Seasonal Affective Disorder (SAD) is so prevalent in the UK, where UVB levels are non-existent for six months of the year.
---
What the Mainstream Narrative Omits
The suppression of the "Sterol Connection" is not merely an oversight; it is a byproduct of a medical system that thrives on chronic disease management rather than root-cause resolution.
The RDA Deception
The Recommended Dietary Allowance (RDA) for Vitamin D in the UK is currently set at 400 IU (10mcg) per day. Most independent researchers argue this is catastrophically low.
- —The 400 IU figure was originally calculated to prevent rickets, a severe bone deformity. It was never intended to support optimal immune or hormonal function.
- —Evidence suggests that the human body, when exposed to midday summer sun in a swimsuit, can produce 10,000 to 20,000 IU of Vitamin D in just 20 minutes.
- —Setting the RDA at 400 IU is like trying to fill a swimming pool with a teaspoon.
The Statin Contradiction
If cholesterol is the raw material for Vitamin D, and Vitamin D is protective against heart disease, then lowering cholesterol to "floor" levels via statins may actually *increase* cardiovascular risk by inducing a Vitamin D deficiency.
- —Mainstream guidelines rarely suggest that patients on statins should co-supplement with high-dose Vitamin D.
- —This creates a feedback loop of pharmaceutical dependency: the statin causes low D, which causes muscle pain and insulin resistance, which leads to more prescriptions for painkillers and metformin.
The "D2 vs. D3" Confusion
Many practitioners still prescribe Ergocalciferol (Vitamin D2), which is derived from fungus (yeast or mushrooms).
- —Human biology is designed for Cholecalciferol (Vitamin D3), the animal/sterol form.
- —D2 is less bioavailable, has a shorter half-life, and competes for the same receptors as D3, potentially causing more harm than good. The mainstream narrative often treats them as interchangeable, which they are not.
Important Fact: Research published in the *Journal of Clinical Endocrinology & Metabolism* found that a mathematical error in the original RDA calculations led to a 10-fold underestimation of the amount of Vitamin D needed to maintain healthy blood levels.
---
The UK Context
The United Kingdom presents a unique "perfect storm" for the disruption of the sterol-to-hormone pathway. This is largely due to our geographical position and the prevailing climate.
The Vitamin D Winter
In the UK, the sun’s angle is too low for the majority of the year to provide enough UVB radiation for Vitamin D synthesis.
- —From October to early April, the "Zenith Angle" of the sun ensures that UVB photons are absorbed by the Earth's atmosphere before they reach our skin.
- —Even on a bright, cold day in February, your body will produce zero Vitamin D. You are effectively living off the "stores" accumulated during the summer—stores which most people never build up in the first place.
The Melanin Paradox
The UK is a multi-ethnic society, and this has profound implications for the Sterol Connection.
- —Melanin acts as a natural sunscreen. It evolved in equatorial regions to protect the body from *too much* UV radiation.
- —For individuals with darker skin tones (South Asian, African, or Caribbean heritage) living in the UK, the problem is magnified. They require 3 to 5 times longer sun exposure than someone with fair skin to produce the same amount of Vitamin D.
- —This has led to disproportionately high rates of autoimmune diseases and metabolic issues in these communities within the UK.
The Cultural "Indoor" Shift
The UK’s "pub culture," office-based economy, and notoriously grey weather mean that even during the "Vitamin D Summer" (May to August), many people remain indoors during the crucial hours of 11:00 AM to 3:00 PM when UVB is at its peak.
- —If you are only outdoors during your morning or evening commute, you are receiving UVA (which causes skin ageing) but no UVB (which creates Vitamin D).
---
Protective Measures and Recovery Protocols
Restoring the balance between cholesterol and Vitamin D requires a departure from conventional "sun-avoidance" advice and a return to ancestral wisdom, bolstered by modern testing.
1. Smart Sun Exposure
Stop viewing the sun as a carcinogen and start viewing it as a nutrient.
- —The Shadow Rule: If your shadow is shorter than you are, you can produce Vitamin D. If your shadow is longer than you, you are getting almost no UVB.
- —Micro-dosing: Aim for 10–20 minutes of exposure (without sunscreen) to as much skin as possible during the midday sun.
- —Protect the Face: The skin on the face is thin and prone to ageing; protect it, but expose the torso, back, and limbs, which have a much higher capacity for D3 synthesis.
2. Nutritional Support for the Sterol Pathway
Since cholesterol is the precursor, your diet must provide the building blocks.
- —Healthy Fats: Consume grass-fed butter, tallow, eggs (especially the yolks), and cold-water fatty fish. These provide the lipids necessary for 7-DHC production.
- —Magnesium — The Missing Link: The enzymes that convert Vitamin D into its active form are magnesium-dependent. If you are magnesium deficient (as 70% of the UK population is), even high-dose Vitamin D supplements will not work; they will simply remain in their inactive form.
- —Vitamin K2 (MK-7): Never take Vitamin D without K2. Vitamin D increases calcium absorption, but K2 acts as the "traffic warden" that directs that calcium into the bones and teeth and away from the arteries.
3. Supplementation Strategy
In the UK climate, supplementation is often a necessity, not an option.
- —Target Levels: Aim for blood levels of 25(OH)D between 100 nmol/L and 150 nmol/L. The NHS "sufficient" level of 50 nmol/L is widely considered by specialists to be the bare minimum to prevent bone disease, not the level for optimal health.
- —Dosage: Most adults in the UK require between 4,000 IU and 5,000 IU daily during the winter to maintain optimal levels.
4. Testing and Monitoring
Don't guess—test.
- —Get a Vitamin D 25-OH blood test twice a year: once in September (at your peak) and once in March (at your lowest).
- —Monitor your Lipid Profile alongside your Vitamin D. If your cholesterol is high but your Vitamin D is low, address the deficiency before consenting to statin therapy.
Callout: Modern lifestyle "biohacks" such as Sperti UVB lamps or high-quality red-light therapy can help bridge the gap for those living in the UK, mimicking the evolutionary stimulus of the sun during the dark winter months.
---
Summary: Key Takeaways
The connection between cholesterol and Vitamin D is one of the most critical, yet misunderstood, relationships in human biology. By reframing cholesterol not as a poison, but as the essential raw material for a master hormone, we can begin to see the current public health crisis in a new light.
- —Cholesterol is the precursor: Without the sterol 7-dehydrocholesterol, Vitamin D synthesis is impossible.
- —UVB is the key: Sunlight in the 290–315 nm range is a biological requirement for human health, not an optional luxury.
- —The UK is a high-risk zone: The "Vitamin D Winter" and our indoor lifestyles mean that most UK citizens are "hormonally starved" for most of the year.
- —The Statin Trap: Artificially lowering cholesterol can lead to a cascade of deficiencies that impair the immune system and cardiovascular health.
- —Synergy matters: Vitamin D requires Magnesium, Vitamin K2, and a healthy lipid base to function correctly.
To reclaim our health, we must stop fearing the sun and the molecules that allow us to harness its power. The "Sterol Connection" is a testament to our deep integration with the natural world—a link that we sever at our own peril. It is time to move beyond the simplistic "cholesterol is bad" narrative and embrace a more sophisticated, biologically grounded understanding of how our bodies truly function.
"Innerstand your biology. Reclaim your light."
This article is provided for informational and educational purposes only. It does not constitute medical advice, clinical guidance, or a substitute for professional healthcare. Information reflects cited research at time of publication. Always consult a qualified healthcare professional before acting on any health information.
RESEARCH FOUNDATIONS
Biological Credibility Archive
Citations provided for educational reference. Verify via PubMed or institutional databases.
Medical Disclaimer
The information in this article is for educational purposes only and does not constitute medical advice, diagnosis, or treatment. Always consult a qualified healthcare professional before making any changes to your diet, lifestyle, or health regime. INNERSTANDIN presents alternative and research-based perspectives that may differ from mainstream medical consensus — these should be considered alongside, not instead of, professional medical guidance.
Read Full DisclaimerReady to learn more?
Continue your journey through our classified biological research.
DISCUSSION ROOM
Members of THE COLLECTIVE discussing "Vitamin D and Cholesterol: The Sterol Connection"
SILENT CHANNEL
Be the first to discuss this article. Your insight could help others understand these biological concepts deeper.
THE ARSENAL
Based on Cholesterol & Lipid Science — products curated by our research team for educational relevance and biological support.
Energy Blend Supports

Lugol’s Iodine – Hormonal Issues, Menopause, Immune System, Brain Fog, Memory, Thyroid, Dry Skin
INNERSTANDING may earn a commission on purchases made through these links. All products are selected based on rigorous educational relevance to our biological research.
RABBIT HOLE
Follow the biological thread deeper