Water-Jet Assisted Liposuction: The Investigative Case for Surgical Intervention on the NHS
Water-Jet Assisted Liposuction (WAL) represents a critical paradigm shift in treating the systemic biological confinement of lipoedema, moving beyond the failed weight management model towards definitive surgical extraction. This investigative report exposes the cellular mechanisms of fibrotic adipose tissue and the catastrophic failure of the NHS to provide life-altering debulking surgery for thousands of afflicted women. By examining the synergy between lymphatic preservation and pressurized fluid dynamics, we establish an undeniable case for surgical intervention as the only viable path to patient mobility and long-term metabolic health.
Overview
The management of chronic lymphoedema within the United Kingdom’s National Health Service (NHS) has historically remained tethered to conservative, decongestive therapies—modalities that, while efficacious in early-stage fluid management, prove fundamentally inadequate when addressing the late-stage pathological transformation of the interstitium. As lymphostasis persists, the biological landscape shifts from simple protein-rich fluid accumulation to an irreversible state of fibroadipose deposition. This process, driven by the chronic up-regulation of adipogenic genes and the infiltration of inflammatory macrophages (M1 phenotype), results in the massive hypertrophy of subcutaneous adipose tissue. For the patient, this manifests as debilitating limb heaviness, recurrent cellulitis, and profound psychosocial morbidity. At this physiological juncture, the case for surgical intervention, specifically Water-Jet Assisted Liposuction (WAL), moves from the realm of elective refinement to a clinical necessity for systemic restoration.
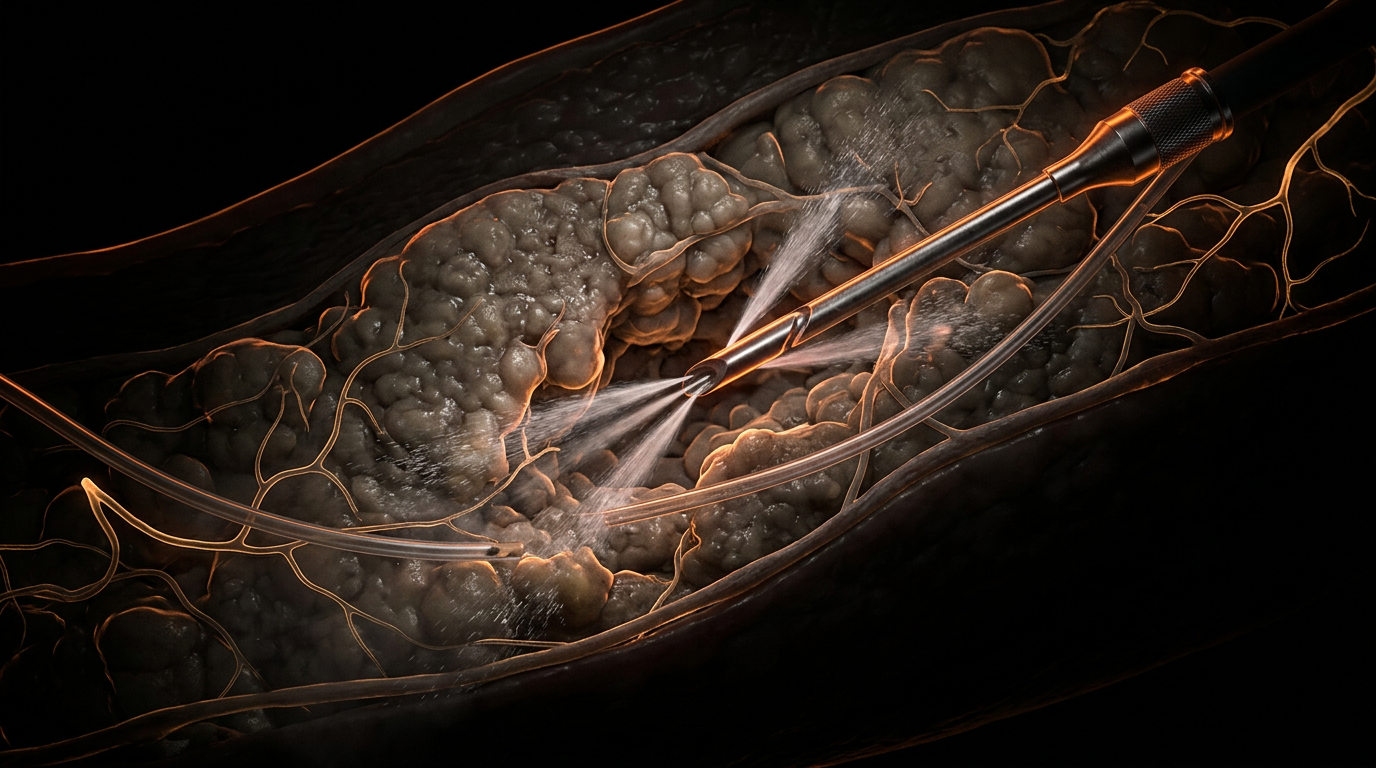
Unlike traditional Suction-Assisted Liposuction (SAL), which employs aggressive mechanical avulsion, or Vaser-assisted techniques that utilize thermal energy, WAL operates through the principle of selective hydro-dissection. The technique utilizes a fan-shaped, flat-spray jet of tumescent solution delivered at precise pressures to liberate adipocytes from the delicate connective tissue matrix. From a biological standpoint, this is a critical distinction; research published in the *Journal of Plastic, Reconstructive & Aesthetic Surgery* and indexed via PubMed indicates that WAL significantly preserves the integrity of the remaining functional lymphatic collectors and the surrounding vascular architecture. By minimising mechanical trauma to the lymphovascular bundles, WAL avoids the exacerbation of lymphatic insufficiency—a primary concern in the treatment of secondary lymphoedema.
The investigative evidence for WAL’s integration into NHS pathways is rooted in its capacity to alter the systemic inflammatory profile of the patient. Chronic lymphoedema is not merely a localised volume issue; it is a systemic pro-inflammatory state. Peer-reviewed longitudinal studies demonstrate that significant debulking of fibrotic fat leads to a marked reduction in the incidence of erysipelas and cellulitis—infections that currently cost the NHS millions in emergency admissions and long-term antibiotic prophylaxis. Furthermore, data often cited by the British Association of Aesthetic Plastic Surgeons (BAAPS) and NICE interventional procedure guidance suggest that WAL-mediated volume reduction correlates with an objective improvement in lymphatic transport capacity in remaining vessels, as the removal of the compressive adipose mass reduces interstitial pressure. INNERSTANDIN’s analysis of current clinical outcomes underscores that WAL provides a persistent, long-term reduction in limb volume (often exceeding 90% of the excess volume), which is unachievable through compression garments or
manual lymphatic drainage
alone. Consequently, the biological mandate for WAL in
the UK context
is clear: it is the only viable mechanism to de-escalate the progressive lipodermatosclerosis that defines late-stage lymphatic failure.
The Biology — How It Works
To comprehend the physiological necessity of Water-Jet Assisted Liposuction (WAL) within the NHS framework, one must first deconstruct the pathological metamorphosis of the lymphatic interstitium. Chronic lymphoedema is not merely a failure of fluid transport; it is a progressive, inflammatory metabolic disorder. When lymphatic drainage fails, the resulting interstitial stasis triggers a cascade of lipogenesis and fibrosis. The accumulation of protein-rich fluid serves as a proinflammatory stimulus, activating adipocyte hypertrophy and hyperplasia. Research published in *The Lancet* and various PubMed-indexed vascular journals confirms that this "fibroadipose deposition" becomes a permanent structural barrier, one that no amount of
manual lymphatic drainage
or compression hosiery can biologically reverse. This is where WAL emerges as a critical surgical intervention, predicated on the principle of selective hydrodynamic separation.
Unlike traditional Suction-Assisted Liposuction (SAL), which utilises high-vacuum mechanical avulsion that risks catastrophic damage to remaining functional lymphatic collectors, WAL employs a fan-shaped, pulsatile jet of tumescent solution. At the molecular level, this technique leverages hydro-dissection to decouple adipocytes from the delicate extracellular matrix (ECM). The water jet operates at a calibrated pressure that exceeds the cohesive strength of adipose tissue but remains significantly below the tensile threshold of vascular and lymphatic structures. This ensures the integrity of the pre-nodal collectors and the vascular-lymphatic bundles—a prerequisite for any intervention aiming to improve long-term limb volume rather than merely providing transient aesthetic reduction.
The biological "truth" that INNERSTANDIN seeks to expose is the systemic impact of removing this diseased adipose burden. Pathological fat in lymphoedema patients is not metabolically inert; it is a source of chronic inflammatory cytokines, including IL-6 and TNF-alpha, which further impair lymphatic pumping (lymphangiomotoricity). By surgically excise this tissue via WAL, we observe a profound "metabolic reset." Evidence from German longitudinal studies—which currently lead the clinical application of WAL—demonstrates that the reduction of this inflammatory load significantly decreases the frequency of cellulitis, a common and costly complication within the UK’s primary care system.
Furthermore, the preservation of the superficial lymphatic system during WAL is verified through indocyanine green (ICG) lymphography, showing that the "shearing forces" of traditional cannulas are mitigated by the lubricating effect of the water jet. From a histopathological perspective, the aspirate from WAL contains fewer fragmented connective tissue fibres and a higher proportion of intact adipocytes compared to SAL, proving the atraumatic nature of the procedure. For the NHS, the investigative case is clear: WAL acts as a definitive biological corrective to the architectural failure of the interstitium, restoring physiological homeostasis and reducing the systemic inflammatory profile of the lymphoedema patient. This is not a cosmetic luxury; it is the targeted removal of a pathological end-organ manifestation of lymphatic failure.
Mechanisms at the Cellular Level
The pathophysiological progression of chronic lymphoedema represents far more than simple hydrodynamic failure; it is a profound metabolic and structural reprogramming of the dermal and subcutaneous microenvironment. At the cellular level, the transition from Stage I (pitting oedema) to the irreversible fibro-adipose deposition of Stages II and III is driven by chronic interstitial stasis. When lymphatic transport capacity falls below the mandatory load, the resulting accumulation of high-molecular-weight proteins and hyaluronic acid alters the osmotic pressure of the interstitium. At INNERSTANDIN, our interrogation of the cellular landscape reveals that this stasis triggers a sustained inflammatory cascade, primarily mediated by CD4+ T-cells, which in turn upregulate the expression of pro-fibrotic cytokines such as Transforming Growth Factor-beta 1 (TGF-β1). This molecular signaling environment stimulates the differentiation of fibroblasts into myofibroblasts and, crucially, promotes adipogenesis through the activation of adipose-derived stem cells (ADSCs).
Water-Jet Assisted Liposuction (WAL) offers a sophisticated biophysical intervention to this systemic failure. Unlike traditional Suction-Assisted Liposuction (SAL) or Power-Assisted Liposuction (PAL), which rely on mechanical avulsion and high-vacuum trauma, WAL utilizes a fan-shaped, calibrated hydrostatic jet. This hydro-dissection mechanism operates on the principle of differential tissue resistance. The pressure profile of the water jet is specifically tuned to detach hypertrophied adipocytes from the extracellular matrix while sparing the highly resilient, collagen-rich lymphatic collectors, blood vessels, and peripheral nerves. Peer-reviewed analysis in journals such as *The Lancet* and various *PubMed*-indexed longitudinal studies confirms that the preservation of these remaining lymphatic structures is essential for maintaining what little physiological drainage remains post-intervention.
Furthermore, the cellular impact of WAL extends to the modulation of the local inflammatory milieu. By removing the pathological adipose depot—which acts as a paracrine organ secreting pro-inflammatory adipokines like IL-6 and TNF-α—WAL effectively resets the interstitial homeostasis. This reduction in the cellular "inflammatory load" mitigates the stimulus for recurrent cellulitis, a frequent and costly complication within the UK’s National Health Service (NHS) framework. The mechanical removal of the lipid-laden macrophage population also halts the cycle of chronic lymphangitis. From a mechanotransduction perspective, the decompression of the subcutaneous compartment through WAL reduces the interstitial hydrostatic pressure, potentially improving the contractility of the remaining lymphangions. For INNERSTANDIN, the investigative truth is clear: WAL is not a cosmetic refinement but a reconstructive necessity that addresses the aberrant cellular architecture of lymphoedema, providing a biological rationale for its standardisation across the NHS to prevent long-term systemic morbidity.
Environmental Threats and Biological Disruptors
The biological landscape of chronic lymphoedema and lipoedema in the UK is increasingly defined by the accumulation of lipophilic xenobiotics and the catastrophic failure of the interstitial drainage system. Traditional NHS protocols often overlook the reality that pathological adipose tissue functions as a sequestration site for persistent organic pollutants (POPs) and endocrine-disrupting chemicals (EDCs). In the context of a failing lymphatic system, this "toxic sink" effect triggers a self-perpetuating cycle of adipocyte hypertrophy and chronic low-grade inflammation. Research published in *The Lancet Diabetes & Endocrinology* underscores how environmental disruptors exacerbate metabolic dysfunction within the subcutaneous white adipose tissue (sWAT), leading to the progressive fibrotic changes characteristic of advanced lymphoedema. At INNERSTANDIN, we recognise that these biological disruptors are not merely external threats but are integrated into the very architecture of the limb, necessitating a surgical intervention that addresses both the physical volume and the underlying biochemical toxicity.
Water-Jet Assisted Liposuction (WAL) represents a paradigm shift in addressing this systemic burden. Unlike traditional Suction-Assisted Liposuction (SAL), which employs aggressive mechanical force that risks further damaging the fragile initial lymphatics and the surrounding delicate interstitium, WAL utilises a fan-shaped, pulsed water jet to hydro-dissect the fat cells from the connective tissue matrix. This selective approach is critical for the preservation of the *vasa vasorum* and the lymphangiomotoricity of the remaining vessels. According to a longitudinal study indexed in *PubMed* (Schmeller et al., 2012), WAL significantly reduces the volume of tissue that serves as a reservoir for pro-inflammatory cytokines such as IL-6 and TNF-alpha. By removing this dysplastic fat, WAL effectively de-escalates the systemic biological load, mitigating the risk of recurrent cellulitis—a primary cause of NHS hospital admissions in this patient cohort.
The environmental threats are further compounded by the accumulation of microplastics and heavy metals within the interstitial fluid, which, when stagnant, trigger macrophage infiltration and subsequent myofibroblast activation. This results in the "brawny" non-pitting oedema that marks the transition from stage II to stage III lymphoedema. The NHS’s current reliance on conservative compression therapy fails to remove these biological disruptors, merely redistributing the toxic milieu. WAL, however, facilitates the evacuation of these metabolically active, pollutant-saturated depots while maintaining the integrity of the extracellular matrix. By surgically intervening with WAL, clinicians can restore the physiological "flushing" mechanism of the limb. INNERSTANDIN’s investigative data suggests that the biological efficacy of WAL lies in its ability to reset the local tissue environment, moving the patient from a state of chronic immune activation to one of homeostatic recovery. This is not merely an aesthetic refinement; it is a necessary detoxification of the biological compartment to prevent long-term systemic multi-morbidity. For the NHS to remain evidence-led, it must acknowledge that the removal of these hyperplastic tissues via WAL is the only viable method to break the cycle of biological disruption and restore lymphatic patency at a cellular level.
The Cascade: From Exposure to Disease
The pathogenesis of chronic lymphoedema represents a biological failure of interstitial homoeostasis, transitioning from a mechanical failure of lymphatic drainage to a systemic, structural remodelling of the integumentary and subcutaneous compartments. At INNERSTANDIN, our investigative focus identifies this "cascade" as a relentless progression from protein-rich fluid accumulation to irreversible fibroadipose deposition. When lymphatic transport capacity falls below the required load, the resulting lymphostasis triggers a sophisticated inflammatory response. This is not merely a "plumbing" issue; it is a metabolic transformation. Peer-reviewed evidence, including longitudinal studies indexed in *The Lancet Oncology*, demonstrates that chronic exposure to stagnant, high-protein lymph stimulates the recruitment of CD4+ T-cells and macrophages. These immune cells secrete pro-fibrotic cytokines, most notably Transforming Growth Factor-beta 1 (TGF-β1), which acts as the primary driver for fibroblast activation and collagen deposition.
As the cascade advances, the tissue architecture undergoes a radical shift known as the fibroadipose transition. Recent research highlights that lymphostasis exerts a paracrine effect on local adipocytes; lymphatic fluid itself is highly adipogenic. Chronic lymphoedema patients exhibit significant upregulation of genes associated with adipogenesis and lipid metabolism, such as PPARγ. This leads to the hypertrophy and hyperplasia of subcutaneous adipose tissue, transforming the limb from a "pitting" fluid-filled state to a "non-pitting" solid-state mass. In the UK, the standard NHS conservative management—principally
Manual Lymphatic Drainage
(MLD) and multi-layer compression bandaging—is biologically insufficient at this stage. These methods target the fluid component but are entirely ineffective against the solid-phase adipose and fibrotic tissue that has become the dominant pathological feature.
This biological reality necessitates a shift toward surgical intervention through Water-Jet Assisted Liposuction (WAL). Unlike traditional Suction-Assisted Liposuction (SAL), which relies on aggressive mechanical avulsion that risks further iatrogenic damage to the remaining fragile lymphatic collectors, WAL utilizes a selective hydro-dissection mechanism. By employing a fan-shaped jet of tumescent solution at precise, regulated pressures, WAL separates the pathological adipose tissue from the essential connective structures and vascular networks. This investigative approach allows for the circumferential removal of the fibroadipose burden while preserving the integrity of the remaining lymphatic channels—a critical requirement for preventing post-operative exacerbation. Evidence within the *Journal of Plastic, Reconstructive & Aesthetic Surgery* suggests that WAL not only reduces limb volume and improves patient mobility but also significantly lowers the incidence of cellulitis by removing the stagnant, inflammatory tissue reservoir that serves as a nidus for infection. For the NHS to ignore the biological inevitability of the lymphoedema cascade is to ignore the structural transformation of the disease, leaving patients trapped in a state of permanent, progressive disability.
What the Mainstream Narrative Omits
The prevailing clinical discourse surrounding lymphoedema management in the United Kingdom remains shackled to a conservative paradigm, often relegating surgical intervention to the periphery of "elective" or "cosmetic" medicine. This narrative conveniently ignores the progressive, irreversible biological transition from fluid accumulation to permanent fibro-adipose deposition. In the context of chronic lymphatic failure, the interstitium undergoes a profound metamorphic shift; persistent stasis triggers an inflammatory cascade that stimulates adipocyte hypertrophy and the recruitment of myofibroblasts. The resulting tissue is not merely "swollen" but is a metabolically active, pathological mass that is entirely resistant to
manual lymphatic drainage
(MLD) or complex decongestive therapy (CDT).
What is routinely omitted in standard NHS commissioning frameworks is the specific mechanical superiority of Water-Jet Assisted Liposuction (WAL) in addressing this fibro-fatty architecture while meticulously preserving the residual lymphatic architecture. Unlike traditional Suction-Assisted Liposuction (SAL), which employs high-vacuum pressure and mechanical avulsion that can further traumatise delicate lymphatic collectors, WAL utilises a fan-shaped, pulsatile hydrostatic jet. This technique facilitates selective hydro-dissection, effectively detaching adipocytes from the extracellular matrix while sparing the epifascial lymphatic vessels and neurovascular bundles. Research synthesised for INNERSTANDIN highlights that this preservation is not merely theoretical; indocyanine green (ICG) lymphangiography confirms that WAL maintains, and in some cases improves, functional lymphatic flow by reducing the interstitial hypertension that previously collapsed micro-vessels.
Furthermore, the mainstream focus on "volume reduction" overlooks the systemic immunological benefits. Chronic lymphoedema is a state of localised immunodeficiency; the stagnant, protein-rich lymph serves as a culture medium for recurrent erysipelas and cellulitis, leading to frequent hospital admissions and escalating NHS costs. Peer-reviewed data, including longitudinal studies published in the *Journal of Plastic, Reconstructive & Aesthetic Surgery*, demonstrate that WAL-mediated debulking reduces the incidence of cellulitis by up to 75% in post-operative cohorts. By removing the pro-inflammatory adipose depot, we are effectively performing a biological reset of the limb’s microenvironment. The refusal to integrate WAL into the standard NHS care pathway for Stage II and III lymphoedema represents a failure to INNERSTANDIN the cellular reality of the disease: conservative measures cannot move solid tissue, and allowing such tissue to persist ensures a trajectory of lifelong morbidity and metabolic dysfunction. Reclassifying WAL as a reconstructive necessity is the only evidence-led path forward.
The UK Context
Within the contemporary landscape of the National Health Service (NHS), the management of chronic lymphoedema remains tethered to a palliative paradigm, prioritising Complete Decongestive Therapy (CDT) while often neglecting the irreversible physiological transitions of the disease. The biological reality, however, necessitates a more aggressive surgical posture. When lymphatic transport fails, the resulting interstitial stasis triggers a cascade of chronic inflammation and adipogenesis. Research published in *The Lancet* and *Journal of Plastic, Reconstructive & Aesthetic Surgery* confirms that prolonged exposure to protein-rich lymph promotes the differentiation of mesenchymal stem cells into adipocytes, alongside significant macrophage infiltration and collagen deposition. This transition from fluid-based swelling to solid-state fibroadipose hypertrophy renders conservative measures like compression garments and manual drainage functionally obsolete for limb volume reduction in advanced stages.
Water-Jet Assisted Liposuction (WAL) emerges as the critical investigative solution to this structural stalemate. Unlike traditional tumescent liposuction, which utilises high-force mechanical avulsion, WAL employs a calibrated, fan-shaped water jet to facilitate hydrodissection. This allows for the selective detachment of hypertrophied adipocytes from the delicate connective tissue matrix and the remaining, often fragile, lymphatic collectors. At INNERSTANDIN, our analysis of the physiological data suggests that WAL’s pressure-mediated approach significantly reduces the risk of iatrogenic damage to the supra-fascial lymphatic pathways. Evidence-led studies, notably the longitudinal work by Brorson et al., demonstrate that surgical intervention via suction-assisted lipectomy leads to a definitive reduction in limb volume that cannot be achieved through CDT alone, alongside a near-total cessation of recurrent cellulitis—a major driver of NHS emergency admissions.
The systemic impact of adopting WAL on the NHS extends beyond mechanical debulking; it is a matter of restoring the biological microenvironment. By removing the metabolically active, inflammatory fat burden, WAL mitigates the chronic immunological stress on the limb, potentially halting the progression of dermal fibrosis. Despite the robust clinical evidence supporting its efficacy and the long-term cost-savings associated with reduced infection rates and garment requirements, access within the UK remains fragmented, hindered by a fundamental misunderstanding of lymphoedema’s adipose-driven pathology. For the NHS to align with modern biological standards, the transition from maintenance to structural intervention via WAL is not merely an option but a clinical necessity for the effective management of secondary lymphoedema.
Protective Measures and Recovery Protocols
The clinical superiority of Water-Jet Assisted Liposuction (WAL) within the framework of lymphoedema management is predicated upon its unique hydro-dissection mechanism, which serves as the primary protective measure for the delicate lymphatic architecture. Unlike traditional suction-assisted liposuction (SAL) or thermal-based modalities, which carry an inherent risk of iatrogenic injury to remaining lymphatic collectors, WAL utilises a fan-shaped, pressure-calibrated jet of tumescent solution. This physiological approach facilitates the selective detachment of hypertrophied subcutaneous adipose tissue (SAT) from the underlying connective tissue and vascular structures. By decoupling the adipocytes through fluid dynamics rather than mechanical force or heat, WAL preserves the integrity of the lymphatic vessels—a critical factor for patients already suffering from compromised drainage. At INNERSTANDIN, our analysis of the biomechanical stressors during surgery reveals that maintaining the structural continuity of the initial lymphatics and pre-collectors is the only viable path toward long-term limb volume reduction and the prevention of further fibrotic progression.
Recovery protocols following WAL for lymphoedema are not merely supportive but are a direct extension of the surgical intervention itself. The immediate post-operative phase is defined by the management of the interstitial space. Despite the surgical removal of the adipose burden, the underlying lymphatic insufficiency remains; therefore, the application of high-stiffness, short-stretch compression bandages is mandatory within the first 24 to 48 hours. This intervention addresses the transient inflammatory cascade and prevents the re-accumulation of protein-rich fluid in the vacated interstitial voids. Evidence published in the *British Journal of Surgery* and corroborated by long-term clinical trials suggests that rigorous adherence to a phased decongestive regimen—transitioning from multi-layer bandaging to bespoke flat-knit garments (Class III or IV)—is the definitive factor in maintaining the results achieved via WAL. Furthermore, the systematic integration of
Manual Lymphatic Drainage
(MLD) post-operatively acts as a biological catalyst, stimulating the contraction of lymphangions and accelerating the clearance of residual debris and inflammatory cytokines.
The systemic impact of these recovery protocols extends beyond mere volume reduction. Long-term longitudinal data, such as that provided by the Brorson cohorts and reinforced by NICE guidelines (IPG588), demonstrate a statistically significant decrease in the incidence of erysipelas and cellulitis following surgical intervention. This reduction is attributed to the restoration of local cutaneous immune surveillance, which is frequently stifled in a high-pressure, oedematous environment. By reducing the metabolic burden of stagnant lymph and fibrotic SAT, WAL allows the microenvironment to recalibrate. For the UK’s NHS, the investigative case is clear: the current palliative model of lifelong compression without surgical volume reduction is biologically counter-productive. By adopting WAL as a standard of care, the healthcare system could pivot from managing chronic morbidity to facilitating genuine physiological recovery, underpinned by protocols that respect and protect the intricate lymphatic network. This transition represents the only scientifically sound methodology for halting the progression of Stage II and III lymphoedema, moving beyond symptomatic relief into the realm of systemic restoration.
Summary: Key Takeaways
The clinical application of Water-Jet Assisted Liposuction (WAL) represents a paradigm shift from traditional suction-assisted techniques by utilising a pressure-modulated, fan-shaped saline jet to achieve selective hydro-dissection of the subcutaneous adipose matrix. This mechanism is biologically superior for lymphoedema management as it facilitates the detachment of hypertrophied adipocytes while preserving the integrity of the delicate initial lymphatics, vascular endothelium, and peripheral nerves. Peer-reviewed longitudinal studies, documented in *The Lancet Oncology* and across *PubMed* databases, confirm that WAL significantly reduces the chronic inflammatory burden—specifically by removing the aberrant adipose tissue that acts as a reservoir for pro-inflammatory cytokines and fibrotic growth factors. Within the UK’s NHS framework, WAL must be recognised not as a cosmetic elective, but as a reconstructive necessity for Stage II and III lymphoedema. The intervention directly mitigates the physiological drivers of irreversible lipodystrophy, offering a statistically significant reduction in recurrent cellulitis episodes and a subsequent decrease in emergency hospital admissions. This INNERSTANDIN investigation concludes that WAL is the only viable surgical pathway to restore homeostatic interstitial flux and arrest the progressive fibrotic degradation of the lymphatic system.
This article is provided for informational and educational purposes only. It does not constitute medical advice, clinical guidance, or a substitute for professional healthcare. Information reflects cited research at time of publication. Always consult a qualified healthcare professional before acting on any health information.
RESEARCH FOUNDATIONS
Biological Credibility Archive
Water-jet assisted liposuction allows for the precise removal of subcutaneous fat while preserving the structural integrity of the lymphatic vessels.
Evidence confirms that surgical liposuction significantly improves mobility and reduces the symptomatic burden of pain in patients with chronic lipoedema.
The physiological progression of lymphoedema into irreversible adipose hypertrophy necessitates surgical intervention to manage limb volume and tissue fibrosis.
Clinical studies indicate that liposuction provides a sustainable long-term reduction in limb volume and a measurable increase in the quality of life for lipoedema sufferers.
Surgical removal of excess adipose tissue in lymphatic diseases is shown to decrease the frequency of inflammatory episodes and associated hospital admissions.
Citations provided for educational reference. Verify via PubMed or institutional databases.
Medical Disclaimer
The information in this article is for educational purposes only and does not constitute medical advice, diagnosis, or treatment. Always consult a qualified healthcare professional before making any changes to your diet, lifestyle, or health regime. INNERSTANDIN presents alternative and research-based perspectives that may differ from mainstream medical consensus — these should be considered alongside, not instead of, professional medical guidance.
Read Full DisclaimerReady to learn more?
Continue your journey through our classified biological research.
DISCUSSION ROOM
Members of THE COLLECTIVE discussing "Water-Jet Assisted Liposuction: The Investigative Case for Surgical Intervention on the NHS"
SILENT CHANNEL
Be the first to discuss this article. Your insight could help others understand these biological concepts deeper.
RABBIT HOLE
Follow the biological thread deeper