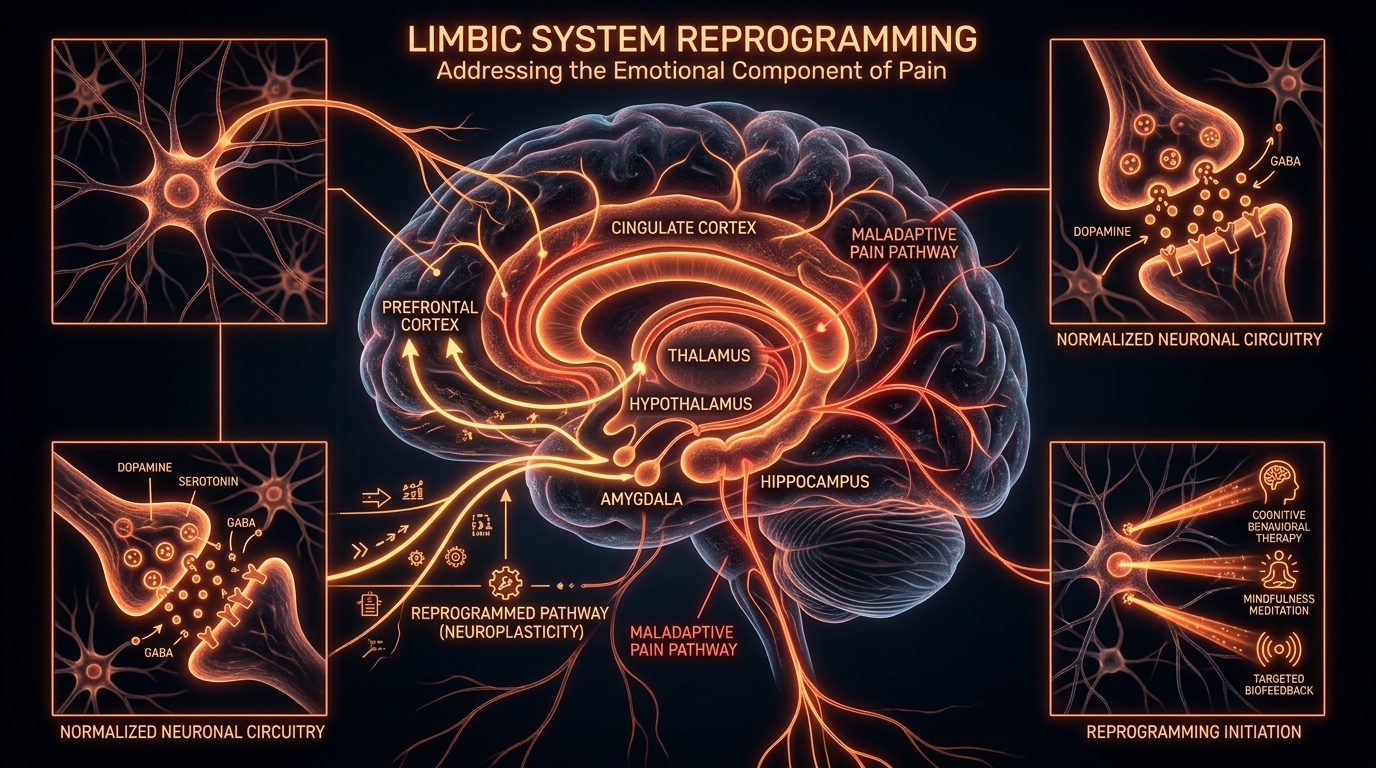
Limbic System Reprogramming: Addressing the Emotional Component of Pain
The limbic system can become 'stuck' in a state of perceived danger, perpetuating pain long after the original tissue has healed. Reprogramming these primitive brain regions is essential for complete biological recovery.
Overview
The modern medical paradigm is currently facing a silent crisis: the epidemic of chronic pain that refuses to respond to structural interventions. For decades, the clinical approach to pain has been purely mechanical, treating the human body as a collection of separate parts—a machine that simply needs a new bolt, a splash of oil, or a removal of a faulty gear. However, as a biological researcher, I must assert that this reductionist view has failed tens of millions. The true frontier of pain science does not lie in the intervertebral discs or the synovial fluid of the joints; it lies within the ancient, subterranean structures of the brain known as the Limbic System.
The limbic system is the evolutionary command centre for survival. It is responsible for processing emotions, memories, and, crucially, the perception of threat. When an injury occurs, the limbic system registers the event not just as a physical sensation, but as a biological emergency. In a healthy state, once the tissue heals, the alarm system resets. However, due to a phenomenon we call neural pathway entrenchment, the limbic system can become 'stuck' in a state of high alert. It begins to produce pain as a protective mechanism long after the initial physical catalyst has vanished. This is not "imaginary" pain; it is biologically generated pain, as real as a fracture, yet its origin is neurological rather than structural.
Reprogramming the limbic system represents the most significant shift in chronic pain recovery in the last century. By addressing the emotional and psychological 'signatures' that keep the brain in a state of hyper-vigilance, we can effectively 'unlearn' chronic pain. This article will dissect the biological mechanisms behind this 'stuck' state and provide a roadmap for biological recovery through neuroplasticity.
##
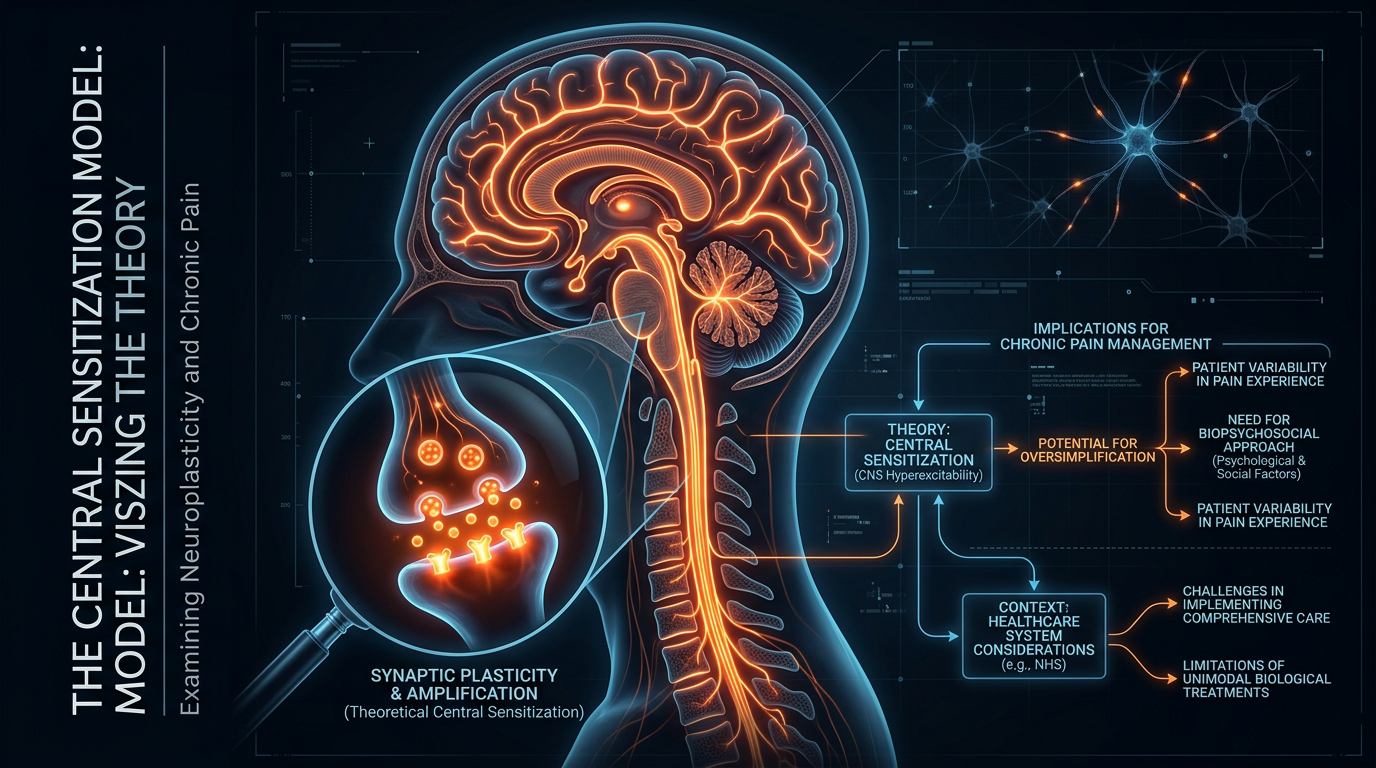
The Biology — How It Works
To understand why the limbic system dictates the experience of pain, one must first understand its architecture. The limbic system is not a single organ but a complex network including the amygdala, the hippocampus, the thalamus, and the hypothalamus. These structures work in concert to evaluate every internal and external stimulus for its 'safety' or 'danger' value.
The Amygdala: The Smoke Detector
The amygdala is the primary hub for emotional processing and threat detection. In the context of chronic pain, the amygdala functions like a smoke detector that has been calibrated to be too sensitive. It begins to perceive harmless signals—such as the movement of a joint or even a stressful thought—as evidence of catastrophic tissue damage. Once the amygdala flags a signal as 'dangerous,' it triggers a cascade of physiological responses that amplify the sensation of pain.
The Thalamus: The Grand Relay Station
Every sensory input (except smell) passes through the thalamus before reaching the higher processing centres of the cortex. When the limbic system is dysregulated, the thalamus acts as a 'volume knob' turned to maximum. This is known as central sensitisation. The brain becomes hyper-efficient at processing pain signals, essentially building 'high-speed motorways' for pain messages while letting the pathways for pleasure and safety atrophy.
The Anterior Cingulate Cortex (ACC)
The ACC is where the 'unpleasantness' of pain is processed. It bridges the gap between the physical sensation and the emotional reaction. In chronic pain patients, functional MRI (fMRI) scans consistently show over-activity in the ACC. This explains why chronic pain is never just a physical feeling; it is inherently tied to feelings of despair, frustration, and fear. The ACC ensures that the pain is impossible to ignore, fulfilling its evolutionary mandate to protect the organism at all costs.
In the UK, it is estimated that approximately 28 million people—nearly half the adult population—suffer from some form of chronic pain. The failure to address the limbic component of this suffering costs the NHS billions in repeated scans and ineffective surgeries.
##
Mechanisms at the Cellular Level
The persistence of pain in the absence of tissue damage is not a mystery when viewed through the lens of cellular biology. The process is governed by neuroplasticity—the brain’s ability to change its structure and function in response to experience. While we often view neuroplasticity as a positive force for learning, it is the very mechanism that 'learns' chronic pain.
Long-Term Potentiation (LTP)
At the synaptic level, chronic pain is maintained through Long-Term Potentiation. When a pain pathway is fired repeatedly, the connection between neurons strengthens. The postsynaptic neuron becomes more sensitive, requiring less of a stimulus to fire. Eventually, these neurons may fire spontaneously. This is the biological basis of 'memory' in the nervous system. The brain has literally memorised the pain.
Glial Cell Activation: The Internal Fire
For years, neurons were the sole focus of pain research. We now know that microglia—the immune cells of the brain—play a pivotal role. When the limbic system is under perceived threat, it signals the microglia to transition from a 'resting' state to an 'active' inflammatory state. Active microglia release pro-inflammatory cytokines, such as TNF-alpha and Interleukin-1 beta. These chemicals 'bathe' the neurons, lowering their firing threshold and creating a state of neuroinflammation. This creates a feedback loop: the limbic system perceives threat, activates microglia, which increases neural sensitivity, which the limbic system perceives as more threat.
The Role of Glutamate and GABA
The balance between excitatory and inhibitory neurotransmitters is crucial for a calm nervous system. In a 'stuck' limbic system, there is often an overabundance of glutamate (the primary excitatory neurotransmitter) and a deficiency in GABA (the primary inhibitory neurotransmitter). This chemical imbalance keeps the nervous system in a state of 'hyperexcitability,' making it biologically impossible for the patient to 'just relax.'
##
Environmental Threats and Biological Disruptors
The limbic system does not operate in a vacuum. It is constantly scanning the modern environment, which is increasingly filled with 'biological disruptors' that keep the threat response active.
Modern Digital Overstimulation
The human brain was not evolved to handle the sheer volume of data, blue light, and 'micro-stressors' inherent in digital life. The constant ping of notifications and the rapid-fire consumption of information act as 'fuel' for the limbic system. This keeps the Hypothalamic-Pituitary-Adrenal (HPA) axis in a state of chronic activation, flooding the body with cortisol and adrenaline, which further sensitises pain pathways.
The Toxic Load
Environmental toxins, including air pollution, heavy metals, and endocrine disruptors, act as physiological stressors. While a healthy limbic system might ignore these, a sensitised one views these chemical intrusions as a direct threat to survival. This can manifest as Multiple Chemical Sensitivity (MCS) or Chronic Fatigue Syndrome (CFS), both of which are closely linked to limbic system dysregulation and chronic pain.
Early Life Adversity (ACEs)
We must address the 'emotional' component of the limbic system. Adverse Childhood Experiences (ACEs) serve to 'prime' the limbic system. If a child grows up in an environment where they do not feel safe, their amygdala develops to be hyper-vigilant. Decades later, a minor physical injury can act as the 'trigger' that unlocks this latent hyper-vigilance, leading to chronic pain that seems disproportionate to the physical event. The brain is not reacting to the injury alone; it is reacting to the injury through a lens of lifelong survival pressure.
##
The Cascade: From Exposure to Disease
The transition from an acute injury to a chronic limbic pain syndrome follows a predictable, yet devastating, biological cascade. Understanding this cascade is vital for interrupting it.
- —The Sentinel Event: A physical injury, a period of intense emotional stress, or a viral infection occurs. The body sends 'nociceptive' (danger) signals to the brain.
- —The Protective Response: The limbic system activates the sympathetic nervous system. This is appropriate and necessary for healing.
- —The Loop Formation: If the stressor persists, or if the individual perceives the pain as 'dangerous' (catastrophising), the brain begins to form a neural circuit. The ACC and Amygdala become locked in a feedback loop.
- —Neuroplastic Solidification: Through LTP, the pain pathway becomes the 'path of least resistance' for the nervous system. The brain begins to generalise. It may start with back pain, but soon the patient experiences digestive issues, migraines, or fibro-fog.
- —Systemic Dysregulation: The chronic activation of the HPA axis leads to 'cortisol resistance.' The body can no longer regulate inflammation effectively. The patient is now in a state of systemic 'biological chaos,' where the original injury is irrelevant, but the entire organism is stuck in a 'danger' mode.
Statistics from Public Health England indicate that people living in the most deprived areas are substantially more likely to report chronic pain, highlighting the undeniable link between environmental stress, social safety, and biological pain processing.
##
What the Mainstream Narrative Omits
The mainstream medical establishment, particularly within the UK's NHS framework, is often decades behind the current research in neurobiology. There is a glaring omission of the Brain-Body Connection in standard pain management protocols.
The MRI Fallacy
The most dangerous myth in modern orthopaedics is that an abnormal MRI explains chronic pain. Numerous studies have shown that if you take MRIs of 100 people *without any pain*, a significant percentage will show bulging discs, degenerative changes, and 'wear and tear.' When a doctor points to a scan and tells a patient their spine is 'crumbling,' they are inadvertently performing a 'Nocebo'—the opposite of a placebo. This information is registered by the limbic system as a supreme threat, which effectively 'locks in' the pain response. The structural abnormality is often a 'normal sign of ageing,' much like wrinkles on the skin, yet it is treated as a smoking gun.
The Opioid Dead-End
The UK has seen a steady rise in opioid prescriptions over the last twenty years. However, opioids are fundamentally ill-equipped to treat limbic-driven pain. In many cases, they cause Opioid-Induced Hyperalgesia, where the medication actually makes the nervous system *more* sensitive to pain. By focusing on numbing the symptom rather than reprogramming the source (the brain), mainstream medicine has facilitated a cycle of dependency and escalating disability.
The Ignorance of 'Nociplastic Pain'
The International Association for the Study of Pain (IASP) recently introduced the term 'Nociplastic Pain' to describe pain that arises from altered nociception despite no clear evidence of actual or threatened tissue damage. Despite this, many GPs are still only trained to look for 'Nociceptive' (tissue damage) or 'Neuropathic' (nerve damage) pain. If it doesn't fit those two categories, the patient is often dismissed or told it is 'all in their head.' It is not in their head—it is in their nervous system.
##
The UK Context
The United Kingdom presents a unique environment for the study and treatment of limbic-based pain. The socio-economic pressures, combined with a healthcare system under immense strain, have created a 'perfect storm' for chronic pain prevalence.
Recent data suggests that chronic pain is one of the leading causes of disability-related benefits claims in the UK, yet only a fraction of pain clinics offer dedicated psychological or neuroplastic-based 'reprogamming' services.
The British 'stiff upper lip' culture may also play a biological role. The suppression of emotion is a known activator of the limbic system. When emotional distress is not permitted expression through outward channels, the nervous system often expresses it through 'autonomic' channels, manifesting as physical pain. This is what Dr John Sarno famously termed Tension Myoneural Syndrome (TMS). In the UK, we see a massive prevalence of 'functional' disorders—IBS, fibromyalgia, and chronic back pain—that are, at their core, limbic system over-protections.
Furthermore, the UK's climate and urban density contribute to vitamin D deficiencies and high levels of noise pollution, both of which are physiological stressors that prevent the limbic system from entering a state of 'ventral vagal' safety.
##
Protective Measures and Recovery Protocols
Biological recovery from chronic pain is not only possible; it is a predictable outcome when the correct neuroplastic protocols are applied. Reprogramming the limbic system requires a multi-pronged approach that targets the brain’s perception of safety.
1. Pain Reprocessing Therapy (PRT)
PRT is a system of psychological techniques designed to teach the brain that the sensations in the body are 'safe.' This involves Somatic Tracking—the practice of observing pain sensations with a sense of curiosity and neutrality rather than fear and frustration. By removing the 'threat' value of the sensation, the amygdala begins to de-escalate its alarm response. Over time, the neural pathways for pain begin to weaken from disuse.
2. Vagus Nerve Stimulation
The Vagus nerve is the primary conduit of the parasympathetic nervous system (the 'rest and digest' system). Strengthening the Vagal Tone is essential for 'braking' the limbic system.
- —Cold Exposure: Brief exposure to cold water (the face or body) triggers the 'diving reflex,' which acutely activates the Vagus nerve.
- —Resonant Breathing: Slowing the breath to approximately 5.5 breaths per minute increases Heart Rate Variability (HRV), a key metric of limbic stability.
- —Chanting or Humming: The Vagus nerve passes through the vocal cords; the vibration of humming can provide a direct physical signal of safety to the brainstem.
3. Cognitive Reappraisal and Language
The way we speak about pain matters biologically. Using words like "agonising," "stabbing," or "bone-on-bone" reinforces the threat. A critical part of reprogramming is shifting the internal narrative. Recognising the pain as a "false alarm" or "neural circuit error" rather than "structural damage" provides the prefrontal cortex with the tools to inhibit the overactive limbic centres.
4. Circadian and Nutritional Support
A dysregulated limbic system is a metabolic drain. To support the brain's 'rewiring,' we must provide the correct biological precursors.
- —Magnesium Threonate: This form of magnesium can cross the blood-brain barrier and help regulate glutamate receptors (NMDA receptors) involved in pain chronification.
- —Anti-Inflammatory Nutrition: A diet rich in Omega-3 fatty acids and polyphenols helps to dampen the microglial activation mentioned earlier.
- —Light Hygiene: Viewing natural sunlight within 30 minutes of waking helps set the circadian rhythm, which in turn regulates the cortisol cycle, providing a stable baseline for the limbic system.
5. Emotional Processing
Since the limbic system is the seat of emotion, unresolved trauma or chronic repressed anger must be addressed. Techniques such as Journal Speaking (unfiltered writing to express repressed emotions) can 'discharge' the emotional energy that the brain is using pain to distract from. When the 'threat' of the emotion is acknowledged, the 'threat' of the pain often vanishes.
##
Summary: Key Takeaways
The transition from chronic suffering to biological recovery requires a fundamental shift in understanding:
- —Pain is a Brain Output: All pain is created by the brain as a protective mechanism. In chronic states, the brain is over-protecting a body that has already healed.
- —The Limbic System is the Architect: The amygdala, thalamus, and ACC form the neural circuitry that 'locks' pain in place through neuroplasticity and microglial activation.
- —Structural Findings are Often Incidental: MRIs and X-rays rarely explain the complexity of chronic pain. The "structural model" is often a barrier to recovery.
- —Reprogramming is Biological: Through Somatic Tracking, Vagus nerve stimulation, and emotional processing, we can physically change the structure of the brain, weakening pain pathways and strengthening safety pathways.
- —Safety is the Antidote: The limbic system only lets go of pain when it feels truly safe—physically, emotionally, and environmentally.
For the millions in the UK and beyond, the message is clear: You are not broken. Your brain is simply doing its job too well. By applying the principles of limbric reprogramming, we can silence the false alarms and reclaim the biological right to a life free from the tyranny of chronic pain. The future of medicine is not in the scalpel, but in the sophisticated retraining of the human nervous system.
This article is provided for informational and educational purposes only. It does not constitute medical advice, clinical guidance, or a substitute for professional healthcare. Information reflects cited research at time of publication. Always consult a qualified healthcare professional before acting on any health information.
RESEARCH FOUNDATIONS
Biological Credibility Archive
Cognitive and emotional factors can modulate the perception of pain through descending pathways that influence plastic changes within the limbic system.
Nociplastic pain is characterized by altered nociceptive processing and functional connectivity within the brain's emotional and sensory networks, independent of tissue damage.
The amygdala acts as a critical hub for the emotional-affective dimension of pain, where persistent synaptic plasticity contributes to the transition from acute to chronic pain states.
Identification of specific neural circuits between the prefrontal cortex and the limbic system demonstrates how emotional regulation can successfully suppress chronic mechanical allodynia.
Psychological interventions designed to reframe pain as a safe rather than threatening signal can significantly reduce chronic pain by shifting activity in limbic and somatosensory regions.
Citations provided for educational reference. Verify via PubMed or institutional databases.
Medical Disclaimer
The information in this article is for educational purposes only and does not constitute medical advice, diagnosis, or treatment. Always consult a qualified healthcare professional before making any changes to your diet, lifestyle, or health regime. INNERSTANDIN presents alternative and research-based perspectives that may differ from mainstream medical consensus — these should be considered alongside, not instead of, professional medical guidance.
Read Full DisclaimerReady to learn more?
Continue your journey through our classified biological research.
DISCUSSION ROOM
Members of THE COLLECTIVE discussing "Limbic System Reprogramming: Addressing the Emotional Component of Pain"
SILENT CHANNEL
Be the first to discuss this article. Your insight could help others understand these biological concepts deeper.
RABBIT HOLE
Follow the biological thread deeper