MDMA-Assisted Psychotherapy: A Paradigm Shift for Treatment-Resistant PTSD
MDMA-assisted therapy allows trauma survivors to process painful memories without being overwhelmed by the brain's fear response. Recent trials demonstrate that 67% of participants no longer meet PTSD criteria after just three sessions, a result far exceeding current UK standard care.
# MDMA-Assisted Psychotherapy: A Paradigm Shift for Treatment-Resistant PTSD
Overview
The landscape of modern psychiatry is currently undergoing a seismic shift, one that promises to dismantle decades of stagnant, symptom-management protocols. At the heart of this revolution lies a compound long misunderstood and politically maligned: 3,4-methylenedioxymethamphetamine, or MDMA. For those suffering from Post-Traumatic Stress Disorder (PTSD)—specifically the "treatment-resistant" variety that defies standard Selective Serotonin Reuptake Inhibitors (SSRIs)—the current medical model has failed. We are witnessing a crisis of efficacy where the standard of care in the UK leaves thousands of veterans, survivors of domestic abuse, and victims of systemic violence in a state of permanent neurological hyper-vigilance.
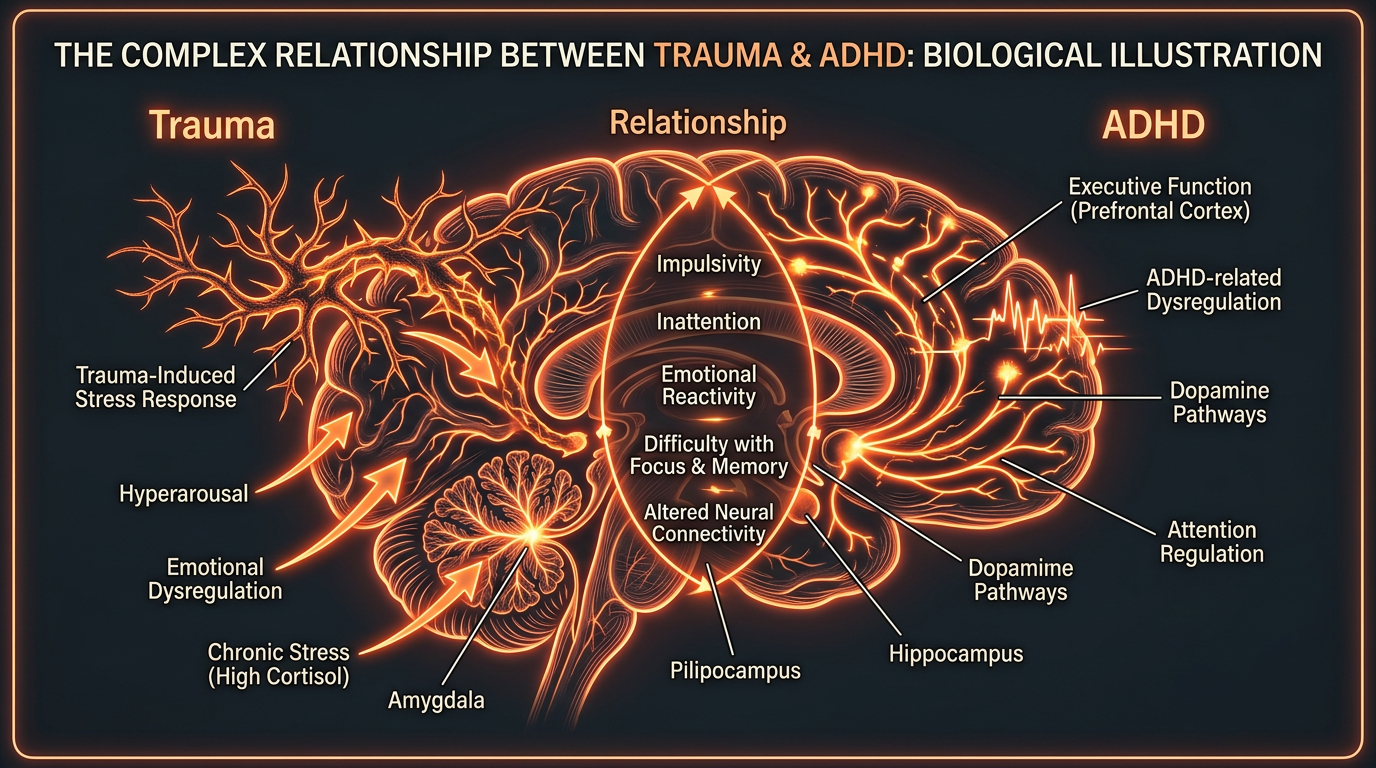
PTSD is not merely a psychological condition; it is a profound biological "freezing" of the nervous system. The brain becomes trapped in a loop of sympathetic dominance, where the amygdala (the fear centre) remains chronically overactive, while the prefrontal cortex (the rational centre) is effectively sidelined. MDMA-assisted psychotherapy offers a unique biological "key" to this lock. Unlike traditional pharmaceuticals that must be taken daily to suppress symptoms, MDMA is administered in a controlled, clinical setting just three times, integrated with intensive psychotherapy.
Recent Phase 3 clinical trials have revealed a staggering truth: 67% of participants who received MDMA-assisted therapy no longer met the diagnostic criteria for PTSD after just three sessions. In comparison, only 32% of the placebo group (who received therapy alone) saw similar results.
This is not a marginal improvement; it is a statistical anomaly in the history of psychiatric medicine. This article will expose the cellular mechanisms, the neurobiological pathways, and the environmental factors that have, until now, kept this life-saving treatment in the shadows of the UK’s regulatory framework.
##
##
The Biology — How It Works
To understand why MDMA is so effective, one must first understand the biological architecture of trauma. When an individual experiences a traumatic event, the brain’s Hypothalamic-Pituitary-Adrenal (HPA) axis is flooded. In a healthy response, the threat passes, and the parasympathetic nervous system restores homeostasis. In PTSD, this restoration never occurs. The brain remains in a state of "high alert," characterised by an inability to distinguish between a past memory and a present threat.
The Amygdala-Prefrontal Cortex Disconnect
In the traumatised brain, the amygdala is hyper-responsive. Any sensory input—a loud noise, a specific scent, or a tone of voice—can trigger a full-scale "fight or flight" response. Simultaneously, the ventromedial prefrontal cortex (vmPFC), which should act as a brake on the amygdala, is inhibited. This creates a state where the patient is emotionally overwhelmed when trying to process their trauma in therapy, leading to "flooding" or "dissociation."
The Window of Tolerance
MDMA functions as a pharmacological bridge. It creates a temporary "window of tolerance" by simultaneously:
- —Decreasing Amygdala Activity: Reducing the fear response and the physiological stress associated with traumatic recall.
- —Increasing Prefrontal Cortex Activity: Enhancing the patient’s ability to process and re-evaluate memories without being hijacked by terror.
- —Enhancing Hippocampal Function: Allowing the brain to correctly "file" the traumatic memory as a past event, rather than an ongoing threat.
By altering this neuro-circuitry, MDMA allows the survivor to revisit the core of their trauma with a sense of safety and self-compassion that is biologically impossible in their standard state.
##
##
Mechanisms at the Cellular Level
The profound psychological shifts induced by MDMA are driven by a complex "chemical cocktail" that targets multiple neurotransmitter systems and hormonal pathways. Unlike classical psychedelics like LSD or Psilocybin, which primarily target the 5-HT2A receptor, MDMA acts as a potent monoamine releaser.
The Monoamine Release: Serotonin, Dopamine, and Norepinephrine
MDMA enters the presynaptic neuron through transport proteins, specifically the Serotonin Transporter (SERT), Dopamine Transporter (DAT), and Norepinephrine Transporter (NET). Once inside, it inhibits the Vesicular Monoamine Transporter 2 (VMAT2), which normally packages neurotransmitters into vesicles. This causes a massive "efflux" or reversal of the transport proteins, flooding the synaptic cleft with:
- —Serotonin: Inducing feelings of euphoria, well-being, and empathy.
- —Dopamine: Enhancing focus and reinforcing the therapeutic process.
- —Norepinephrine: Providing the energy and arousal needed to engage with difficult material without lapsing into dissociation.
The Oxytocin "Pro-Social" Surge
Perhaps the most critical biological component for therapy is the release of Oxytocin. MDMA stimulates the hypothalamus to release large quantities of this "bonding hormone" into the bloodstream and brain.
Oxytocin release during MDMA sessions is significantly higher than that seen in natural social bonding. This surge is responsible for the deep sense of trust between the patient and the therapist, effectively dissolving the "paranoia" and "defensiveness" that often sabotage traditional trauma therapy.
BDNF and Neuroplasticity
MDMA increases the expression of Brain-Derived Neurotrophic Factor (BDNF). This protein is essential for neuroplasticity—the brain's ability to form new neural connections. In the context of PTSD, this means the brain can literally "rewire" itself, creating new pathways that bypass the old, calcified "fear tracks." This is why the benefits of MDMA-assisted therapy persist long after the drug has left the system; it facilitates a structural change in the brain's architecture.
##
##
Environmental Threats and Biological Disruptors
While the potential for MDMA-assisted therapy is revolutionary, the biological efficacy of such treatments is often hampered by modern environmental disruptors. At INNERSTANDING, we recognize that the brain does not exist in a vacuum. The UK’s current environmental landscape—saturated with industrial toxins and synthetic chemicals—can create a state of "neuro-inflammation" that prevents the brain from responding optimally to therapeutic interventions.
Neuro-inflammation and the Blood-Brain Barrier
The success of MDMA therapy relies on a healthy, plastic brain. However, chronic exposure to Glyphosate (the most widely used herbicide in the UK) and other organophosphates can degrade the Blood-Brain Barrier (BBB). When the BBB is compromised, systemic inflammation enters the central nervous system, activating microglia—the brain's resident immune cells.
- —Microglial Activation: When microglia are chronically "on," they release pro-inflammatory cytokines like IL-6 and TNF-alpha, which interfere with serotonin synthesis and BDNF production.
- —Oxidative Stress: Industrial pollutants and heavy metals (like aluminium and lead) found in urban air and tap water increase the "oxidative load" on neurons. This makes the brain less resilient and more prone to the "comedown" effects often associated with MDMA, as the mitochondria are already struggling to produce ATP.
Endocrine Disruptors and Hormonal Balance
The role of Oxytocin and Prolactin in MDMA therapy is paramount. However, the prevalence of Phthalates and Bisphenol A (BPA) in consumer products acts as "endocrine disruptors." These chemicals can mimic or block natural hormones, potentially desensitising the receptors that MDMA targets. If a patient’s hormonal baseline is dysregulated by environmental xenoestrogens, the "bonding" and "empathy" effects of MDMA may be significantly blunted.
##
##
The Cascade: From Exposure to Disease
The progression from a traumatic event to "Treatment-Resistant PTSD" is a biological cascade of failure. It is not just a "bad memory"; it is a systemic collapse of the body’s ability to regulate stress.
Stage 1: The Initial Insult
A traumatic event triggers a massive release of Glutamate and Cortisol. In a resilient system, the Hippocampus provides context, and the Parasympathetic Nervous System (via the Vagus nerve) eventually dampens the response.
Stage 2: The Failure of Extinction Learning
In PTSD, "extinction learning"—the process by which the brain learns that a previous threat is no longer present—fails to occur. This is often due to a deficiency in the Endocannabinoid System. Specifically, low levels of the endocannabinoid Anandamide (often called the "bliss molecule") are linked to the inability to "forget" or move past traumatic triggers.
Stage 3: The Allostatic Load
As the trauma remains "live" in the nervous system, the Allostatic Load (the cumulative wear and tear on the body) increases. This leads to:
- —HPA Axis Dysregulation: Resulting in chronic fatigue or "adrenal burnout."
- —Epigenetic Changes: Trauma can actually alter the expression of genes (such as the FKBP5 gene), making the individual more susceptible to stress for the rest of their life, and even passing this susceptibility to their offspring.
- —Cardiovascular Strain: Chronic sympathetic dominance leads to increased heart rate variability (HRV) issues and hypertension.
MDMA-assisted therapy intervenes at the epigenetic and neurological level, "resetting" the HPA axis and allowing for the extinction learning that was previously blocked.
##
##
What the Mainstream Narrative Omits
The delay in adopting MDMA as a legal therapeutic tool is one of the greatest medical travesties of the 21st century. The mainstream narrative often focuses on the "risks of abuse" or "neurotoxicity," yet these concerns are frequently based on flawed or debunked science.
The Myth of "Brain Holes"
In the late 1990s and early 2000s, a narrative was pushed—often supported by biased government-funded studies—that MDMA caused "holes in the brain" or permanent serotonin depletion. Much of this research was later retracted or found to have used vastly higher doses than those used in clinical settings, or in some cases, used the wrong drug entirely (methamphetamine instead of MDMA).
The Profit Motive vs. The Cure
Current psychiatric standard care relies on the "Pill-a-Day" model. SSRIs like Sertraline or Fluoxetine are designed for chronic use, often for years or decades. This is highly profitable for the global pharmaceutical industry. MDMA-assisted therapy, conversely, is an "Event-Based" model.
- —It requires only 2 or 3 doses.
- —It aims for a "cure" rather than "maintenance."
- —It requires intensive human-to-human interaction (therapy), which cannot be scaled or "automated" like a prescription.
The mainstream narrative omits the fact that the regulatory hurdles placed in front of MDMA are as much about protecting the market share of traditional antidepressants as they are about "public safety."
##
##
The UK Context
In the United Kingdom, the situation for PTSD sufferers is particularly dire. The NHS is currently overwhelmed, with waiting lists for basic Cognitive Behavioural Therapy (CBT) stretching into months or years. For veterans of conflicts in Afghanistan, Iraq, and Northern Ireland, the "gold standard" of CBT or EMDR (Eye Movement Desensitisation and Reprocessing) frequently fails, leaving a population of "treatment-resistant" individuals at high risk for suicide and homelessness.
Regulatory Stagnation: The MHRA and NICE
The Medicines and Healthcare products Regulatory Agency (MHRA) and the National Institute for Health and Care Excellence (NICE) hold the keys to MDMA’s legal status. While the US FDA granted MDMA "Breakthrough Therapy" status years ago, the UK has been slower to move.
According to data from the Office for National Statistics (ONS), the rate of suicide among veterans is a growing concern. The refusal to fast-track a treatment with a 67% success rate is not just a regulatory oversight; it is a public health failure of the highest order.
The Cost-Benefit Reality
Critics often point to the high cost of MDMA-assisted therapy, which involves two therapists present for several 8-hour sessions. However, when one calculates the long-term cost of a PTSD patient to the UK economy—including PIP (Personal Independence Payment) benefits, NHS emergency room visits, lost tax revenue, and the social cost to families—the MDMA model is vastly more cost-effective. A "cure" in three sessions is infinitely cheaper than forty years of disability payments and daily medication.
##
##
Protective Measures and Recovery Protocols
For MDMA-assisted therapy to be safe and effective, the biological terrain of the patient must be prepared and repaired. At INNERSTANDING, we advocate for a rigorous nutritional and environmental protocol to support the "neuro-metabolic" demands of the treatment.
Pre-Session Preparation
The release of monoamines is a metabolically expensive process. To ensure the brain has the necessary building blocks, we recommend:
- —Magnesium Glycinate: To prevent jaw clenching (bruxism) and support over 300 enzymatic reactions in the brain.
- —Omega-3 Fatty Acids (EPA/DHA): To reduce neuro-inflammation and improve the fluidity of neuronal membranes, making receptors more responsive.
- —Antioxidant Loading: Using Alpha-Lipoic Acid (ALA) and Acetyl-L-Carnitine (ALCAR) to protect the mitochondria from any potential oxidative stress during the period of increased neurotransmitter activity.
The Post-Session "Integration" Window
The 48 to 72 hours following an MDMA session are critical for "structural" neuroplasticity.
- —5-HTP Supplementation: Taken 24 hours *after* the session (never before) to help the brain replenish its serotonin stores.
- —Sleep Hygiene: Prioritising deep, restorative sleep to allow the Glymphatic System to clear out metabolic waste and facilitate the "consolidation" of new, healthy neural pathways.
- —Avoiding Circadian Disruptors: Limiting exposure to artificial blue light and EMFs, which can disrupt the natural production of Melatonin, a powerful neuro-protective antioxidant.
Gut-Brain Axis Support
Since 90% of the body’s serotonin is produced in the gut, any protocol must address the microbiome. Eliminating ultra-processed foods and pesticides (which act as antibiotics to beneficial gut flora) ensures that the "raw materials" for neurotransmitter synthesis are available for the brain's recovery.
##
##
Summary: Key Takeaways
The evidence is clear, and the biological mechanisms are understood. MDMA-assisted psychotherapy represents the most significant breakthrough in the treatment of trauma in the history of the NHS.
- —The 67% Solution: In Phase 3 trials, two-thirds of participants were cured of PTSD. This eclipses any existing pharmaceutical intervention.
- —Biological Reset: MDMA doesn't just "numb" the pain; it down-regulates the amygdala and up-regulates the prefrontal cortex, allowing the brain to process and "file" trauma.
- —Oxytocin as a Catalyst: The massive release of Oxytocin creates the "therapeutic alliance" necessary for deep psychological healing.
- —Environmental Awareness: For this treatment to succeed, we must address the "toxic soup" of the UK’s environmental landscape, which drives the neuro-inflammation that underlies treatment resistance.
- —Economic Logic: Transitioning from a "pill-a-day" model to an "event-based" cure is not only more humane; it is the only way to alleviate the long-term financial burden on the NHS.
The shift is coming. The question is no longer whether MDMA-assisted therapy works, but how much longer the UK’s regulatory bodies will allow trauma survivors to suffer in silence while a proven biological cure remains just out of reach. It is time to move beyond the "management" of trauma and into the era of genuine neurological liberation.
This article is provided for informational and educational purposes only. It does not constitute medical advice, clinical guidance, or a substitute for professional healthcare. Information reflects cited research at time of publication. Always consult a qualified healthcare professional before acting on any health information.
RESEARCH FOUNDATIONS
Biological Credibility Archive
Citations provided for educational reference. Verify via PubMed or institutional databases.
Medical Disclaimer
The information in this article is for educational purposes only and does not constitute medical advice, diagnosis, or treatment. Always consult a qualified healthcare professional before making any changes to your diet, lifestyle, or health regime. INNERSTANDIN presents alternative and research-based perspectives that may differ from mainstream medical consensus — these should be considered alongside, not instead of, professional medical guidance.
Read Full DisclaimerReady to learn more?
Continue your journey through our classified biological research.
DISCUSSION ROOM
Members of THE COLLECTIVE discussing "MDMA-Assisted Psychotherapy: A Paradigm Shift for Treatment-Resistant PTSD"
SILENT CHANNEL
Be the first to discuss this article. Your insight could help others understand these biological concepts deeper.
RABBIT HOLE
Follow the biological thread deeper