Mucosal Membrane Erosion in the Modern Diet
Processed foods in the UK are stripping the protective mucus lining of the digestive and respiratory tracts. We examine the anatomical vulnerability this creates for pathogen entry.
Overview
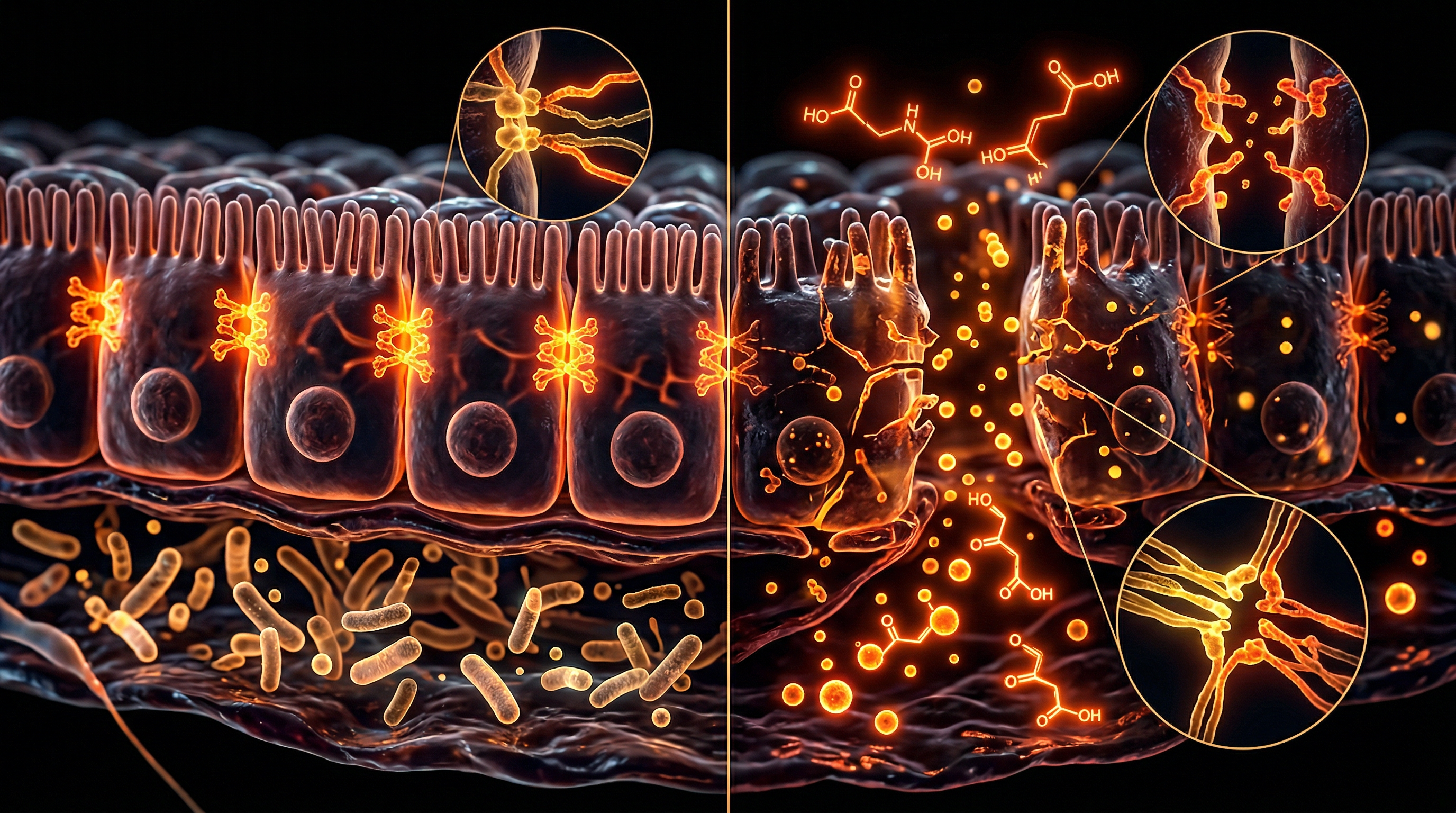
The anatomical integrity of the mucosal barrier represents the primary interface between the internal milieu and an increasingly hostile external environment. In the context of modern British dietary patterns—defined by a heavy reliance on ultra-processed foods (UPFs) and synthetic additives—this multi-layered biological shield is undergoing a process of chronic attrition. To achieve a true INNERSTANDIN of this pathology, one must first recognise that the mucosal membrane is not a passive liner but a sophisticated, dynamic organ system comprising the glycocalyx, a stratified mucus bilayer, and a single layer of polarised epithelial cells tethered by complex junctional proteins.
The erosion of this architecture is driven by a synergistic assault from emulsifiers, such as carboxymethylcellulose (CMC) and polysorbate 80, which are ubiquitous in the UK food supply. Peer-reviewed research, notably published in *Nature* (Chassaing et al.), demonstrates that these detergents act directly upon the biophysical properties of the mucus layer, particularly the inner adherent layer that is typically devoid of bacteria. By increasing the translocation of commensal and pathogenic microbes across this barrier, these compounds facilitate direct contact between the microbiota and the intestinal epithelium. This contact triggers the NLRP3 inflammasome pathway, initiating a cascade of pro-inflammatory cytokines (IL-1β and IL-18) that degrade the structural proteins of the *Zonula occludens*, specifically claudins and occludins.
Furthermore, the "Modern Diet" is characterised by a profound deficiency in fermentable fibres, leading to the metabolic starvation of the gut microbiota. In the absence of exogenous polysaccharides, saccharolytic bacteria such as *Akkermansia muciniphila* are forced to switch to endogenous substrates, effectively consuming the host’s protective mucin-2 (MUC2) glycoproteins to survive. This autophagic erosion thins the protective gel, reducing its viscosity and rendering the underlying epithelium vulnerable to proteolytic enzymes and bile salts. The systemic consequences are profound; as the anatomical barrier fails, Lipopolysaccharides (LPS)—potent bacterial endotoxins—leak into the portal circulation. Data increasingly cited in *The Lancet* and *Gastroenterology* link this "metabolic endotoxaemia" to the UK’s escalating rates of non-alcoholic fatty liver disease (NAFLD) and insulin resistance. We are witnessing an anatomical crisis where the degradation of the mucosal micro-architecture serves as the foundational catalyst for systemic metabolic collapse, a reality that demands a rigorous, evidence-led re-evaluation of Western nutritional norms.
The Biology — How It Works

Panaceum – Prebiotic Oligosaccharide Complex
Panaceum is a specialist eight-oligosaccharide blend designed to restore the microbial diversity missing from the modern Western diet. By providing the complex fibres our ancestors once consumed, it feeds and sustains a resilient gut microbiome for long-term health.
Vetting Notes
Pending
The structural integrity of the human mucosal barrier, specifically the gastrointestinal *tunica mucosa*, represents the primary interface between the external environment and the internal systemic milieu. This multi-layered architecture is comprised of a physical barrier—the epithelial monolayer—and a biochemical supernatant consisting of highly glycosylated proteins known as mucins (primarily MUC2). In the context of the modern British diet, which is heavily saturated with ultra-processed foods (UPFs), this delicate anatomical configuration is undergoing a process of chronic, sub-clinical erosion.
The mechanism of erosion begins with the degradation of the glycocalyx and the overlying mucus gel layer. Research published in *Nature* and *The Lancet Gastroenterology & Hepatology* highlights that the lack of fermentable dietary fibre forces the gut microbiota to seek alternative carbon sources. In the absence of exogenous polysaccharides, commensal bacteria such as *Bacteroides thetaiotaomicron* and *Akkermansia muciniphila* pivot to the endogenous consumption of host mucin glycans. This microbial "autophagy" of the protective lining thins the barrier, reducing its viscoelasticity and exposes the underlying enterocytes to direct contact with luminal toxins and pathogenic microorganisms.
Furthermore, the ubiquity of industrial emulsifiers—specifically carboxymethylcellulose (E466) and polysorbate 80 (E433)—in the UK food supply acts as a detergent-like catalyst for erosion. These amphiphilic molecules disrupt the hydrophobic interactions between mucin fibres, effectively dissolving the "protective shield" of the gut. As the mucus layer dissipates, the underlying apical junctional complex, including the *zonula occludens* (tight junctions) and *macula adherens* (desmosomes), is compromised. The down-regulation of proteins such as occludin and claudin-1 increases paracellular permeability, a state INNERSTANDIN identifies as a precursor to systemic metabolic endotoxaemia.
This anatomical failure facilitates the translocation of lipopolysaccharides (LPS)—pro-inflammatory bacterial cell wall components—directly into the portal circulation. The subsequent activation of Toll-like receptor 4 (TLR4) on submucosal macrophages triggers a cascade of pro-inflammatory cytokines, including TNF-alpha and Interleukin-6 (IL-6). This is not merely a digestive issue; it is a fundamental architectural collapse. The erosion of the mucosal membrane transforms a selective semi-permeable filter into a porous sieve, allowing environmental stressors to bypass the body's primary line of defence. At INNERSTANDIN, we recognise this as the "molecular thinning" of the human biological suit, where the modern diet functions as a corrosive agent, stripping away the evolutionary layers designed to maintain homeostatic sequestration. The result is a systemic state of hyper-inflammation, where the body's internal anatomy is perpetually engaged in a futile attempt to repair a barrier that is being chemically dismantled faster than it can be biologically regenerated.
Mechanisms at the Cellular Level
To comprehend the erosion of the mucosal membrane within the framework of INNERSTANDIN, one must first scrutinise the architectural integrity of the apical junctional complex (AJC). The mucosal barrier is not merely a passive filter; it is a high-turnover dynamic biosystem comprising a glycocalyx, a viscous mucus layer dominated by the MUC2 proteoglycan, and a monolayer of polarised epithelial cells. In the context of the modern British diet—characterised by an unprecedented density of ultra-processed foods (UPFs)—this cellular architecture is under constant biochemical assault.
The primary mechanism of erosion involves the disruption of the "tight junctions" (zonula occludens), specifically the protein-to-protein interactions between claudins, occludins, and junctional adhesion molecules. Peer-reviewed research, notably in *The Lancet Gastroenterology & Hepatology*, indicates that dietary emulsifiers such as carboxymethylcellulose (CMC) and polysorbate-80 act as molecular detergents. These surfactants intercalate into the lipid bilayer of the epithelial cells and dissolve the hydrophobic mucus layer that sequestered the microbiota from the underlying tissue. This thinning of the mucus allows commensal and pathogenic bacteria to come into direct contact with the epithelium, triggering a cascade of pro-inflammatory cytokines, specifically Interleukin-8 (IL-8) and Tumour Necrosis Factor-alpha (TNF-α), via the NF-κB signalling pathway.
Furthermore, the cellular erosion is exacerbated by the depletion of fermentable fibres, a staple deficiency in the UK’s modern nutritional landscape. When the gut microbiota is deprived of prebiotic substrates, species such as *Akkermansia muciniphila* shift their metabolic activity toward the degradation of the host’s own mucin glycans as a primary energy source. This autophagic process of the mucosal barrier leads to a measurable reduction in trans-epithelial electrical resistance (TEER), a gold-standard metric for barrier competence. At the subcellular level, this is evidenced by Endoplasmic Reticulum (ER) stress within goblet cells, which impairs the synthesis and secretion of new MUC2, creating a feedback loop of structural degradation.
The systemic consequence of this cellular erosion is the translocation of Lipopolysaccharides (LPS)—endotoxic components of Gram-negative bacterial cell walls—into the portal circulation. This phenomenon, termed metabolic endotoxaemia, is the definitive link between mucosal erosion and the UK’s escalating rates of insulin resistance and chronic low-grade inflammation. At INNERSTANDIN, we recognise that this is not a benign shift in anatomy, but a fundamental dissolution of the biological boundary between the external environment and the internal milieu, facilitated by chemical additives that the human evolutionary blueprint is ill-equipped to process. The erosion is a precise, quantifiable destruction of the cellular scaffolding that maintains systemic homoeostasis.
Environmental Threats and Biological Disruptors
The mucosal barrier represents the body’s most critical frontier, a complex architecture of epithelial cells, tight junction proteins, and a protective glycocalyx that mediates the delicate interface between the internal milieu and an increasingly hostile external environment. At INNERSTANDIN, we recognise that the erosion of this barrier is not merely a localised digestive concern but a systemic biological catastrophe. The modern diet acts as a multi-vector assault on these membranes, primarily through the introduction of synthetic emulsifiers—specifically carboxymethylcellulose (CMC) and polysorbate-80. Peer-reviewed evidence published in *Nature* (Chassaing et al., 2015) demonstrates that these detergents do not remain inert; they actively degrade the hydrophobic properties of the mucus layer, allowing pro-inflammatory microbiota to migrate into the previously sterile inner mucus zone. This proximity triggers a cascade of inflammatory signalling via Toll-like receptors (TLRs), leading to a chronic state of metabolic endotoxaemia.
Furthermore, the ubiquity of ultra-processed foods (UPFs) in the UK—now comprising over 50% of the national caloric intake—introduces a lethal concentration of xenobiotics that compromise transepithelial electrical resistance (TEER). The pervasive use of glyphosate-based herbicides in industrial agriculture, despite contentious regulatory oversight, poses a direct threat to the Shikimate pathway within our commensal microbiota. While humans lack this pathway, our symbionts do not; the resulting dysbiosis reduces the production of short-chain fatty acids (SCFAs) like butyrate, which is the primary fuel source for colonocytes and essential for the synthesis of *Muc2* proteins. Without sufficient butyrate, the mucosal lining undergoes atrophy, leading to the clinical manifestation of 'leaky gut' or increased intestinal permeability.
The biological disruptors are not limited to ingested substances. The inhalation of particulate matter (PM2.5), particularly in high-density UK urban environments, exerts a distal effect on the gastrointestinal mucosa. Research in *The Lancet Planetary Health* indicates that inhaled pollutants can be swallowed via mucociliary clearance, where they induce oxidative stress and apoptosis in the intestinal epithelium. This is compounded by the rising prevalence of microplastics, which have been detected within the human bloodstream and deep lung tissue. These polymers act as physical irritants and chemical vectors for endocrine-disrupting phthalates, further destabilising the zonula occludens proteins (Zonulin and Occludin) that maintain the integrity of the tight junctions. When these "gatekeepers" fail, the systemic translocation of lipopolysaccharides (LPS) from Gram-negative bacteria becomes inevitable, driving the current epidemic of autoimmune and neurodegenerative pathologies that INNERSTANDIN aims to decode. We are witnessing a fundamental shift where the human biological architecture is being re-engineered by its environment, leading to a state of permanent immunological vigilance and mucosal exhaustion.
The Cascade: From Exposure to Disease
The pathogenesis of mucosal erosion begins with the insidious degradation of the mucus hydrogel—a sophisticated, multi-layered biopolymer primarily composed of the MUC2 glycoprotein. In the healthy British gut, this barrier serves as the primary interface between the external environment and the internal milieu. However, the modern dietary landscape, saturated with ultra-processed foods (UPFs), introduces a suite of chemical agents that act as biological detergents. Research published in *Nature* and *The Lancet Gastroenterology & Hepatology* highlights that dietary emulsifiers—specifically polysorbate 80 and carboxymethylcellulose—possess the capacity to perturb the physical integrity of the mucus layer, reducing the distance between the densest microbial populations and the underlying intestinal epithelium.
At INNERSTANDIN, we recognise that this architectural thinning is the precipitating event in a systemic cascade. As the protective glycocalyx is compromised, the "inner" sterile zone of the mucus layer—traditionally devoid of bacteria—becomes colonised. This contact triggers a pro-inflammatory signaling loop via Toll-like receptors (TLRs), specifically TLR4 and TLR5, located on the apical surface of enterocytes. The resultant upregulation of zonulin, a protein that modulates intercellular junctions, leads to the disassembly of tight junction proteins such as occludin and claudins. This phenomenon, clinically termed increased intestinal permeability, facilitates the translocation of lipopolysaccharides (LPS)—potent endotoxins derived from Gram-negative bacterial cell walls—directly into the portal circulation.
The transition from localized erosion to systemic pathology is marked by "metabolic endotoxemia." Once LPS breaches the mucosal barrier, it initiates a chronic, low-grade inflammatory state characterised by elevated systemic concentrations of interleukin-6 (IL-6) and tumour necrosis factor-alpha (TNF-α). In the UK, where UPF consumption accounts for over 50% of the national caloric intake, this cascade is increasingly implicated in the rise of non-communicable diseases. The erosion does not merely cause local discomfort; it recalibrates the systemic immune set-point. Evidence suggests that this sustained immunological insult drives the progression of insulin resistance, hepatic steatosis, and even neuroinflammation via the gut-brain axis.
The biological reality is clear: the modern diet acts as a mechanical and chemical abrasive against the body’s most critical defensive layer. By stripping the mucosal lining of its protective viscosity, modern nutritional habits force the immune system into a state of perpetual hyper-vigilance. This cascade—from the chemical dissolution of MUC2 to the systemic infiltration of endotoxins—represents the foundational mechanism behind the contemporary epidemic of multi-systemic dysfunction. At INNERSTANDIN, our objective is to expose the physiological price of this environmental mismatch, tracing the direct lineage from the ingestion of synthetic additives to the cellular erosion of human vitality.
What the Mainstream Narrative Omits
The standard clinical discourse regarding gastrointestinal health in the United Kingdom remains fixated on macroscopic pathologies—ulcerations, overt gastritis, or symptomatic reflux—while systematically ignoring the insidious, sub-clinical erosion of the mucosal architecture. At INNERSTANDIN, we recognise that the mainstream narrative fails to address the foundational disintegration of the glycocalyx and the subsequent compromise of the MUC2 mucin layer, which serves as the primary biophysical barrier between the internal milieu and a hostile luminal environment. This erosion is not merely a localised digestive inconvenience; it is a profound anatomical failure driven by the biochemical profile of the modern British diet.
Peer-reviewed evidence, notably published in *Nature* and *The Lancet Gastroenterology & Hepatology*, highlights the devastating impact of dietary emulsifiers—such as carboxymethylcellulose (CMC) and polysorbate 80—prevalent in ultra-processed foods that constitute over 50% of the UK’s caloric intake. These compounds act as biological detergents, reducing the viscoelasticity of the adherent mucus layer and promoting the translocation of commensal bacteria toward the epithelial surface. When this protective hydrogel is thinned, the underlying enterocytes are exposed to proteolytic enzymes and lipopolysaccharides (LPS). The mainstream narrative frequently overlooks the resultant 'leaky gut' or paracellular permeability, yet the molecular reality involves the degradation of tight junction proteins—specifically claudins and occludins—leading to systemic endotoxaemia.
Furthermore, the anatomical integrity of the mucosa is dependent on a symbiotic relationship with mucin-degrading bacteria like *Akkermansia muciniphila*. In a diet deficient in fermentable fibres—a hallmark of contemporary Western nutrition—these microbial populations are forced to catabolise the host’s own mucosal lining as a primary carbon source. This autophagous-like process results in a denuded epithelium, triggering a cascade of chronic low-grade inflammation that transcends the gut-lung and gut-brain axes. The systemic implications are vast, ranging from metabolic syndrome to neuroinflammation, yet these are rarely framed as consequences of mucosal architectural failure. INNERSTANDIN asserts that until the medical establishment acknowledges this dietary-induced erosion of the glycocalyx as a primary driver of systemic disease, the "treatment" of symptoms will remain an exercise in futility. We must look beyond simple acidity and address the structural dissolution of our most vital biological interface.
The UK Context
The United Kingdom presents a critical epidemiological landscape for the study of mucosal membrane erosion, primarily due to the disproportionate saturation of ultra-processed foods (UPFs) within the national diet—accounting for over 50% of total caloric intake, the highest in Europe. At the anatomical level, this dietary profile induces a chronic biochemical assault on the protective glycocalyx and the underlying epithelial monolayers. At INNERSTANDIN, our synthesis of the current literature suggests that the British "Westernised" diet acts as a detergent-like catalyst for the degradation of the MUC2 mucin polymers that constitute the primary physical barrier of the gastrointestinal tract.
Research published in *The Lancet Gastroenterology & Hepatology* highlights a direct correlation between the ubiquity of dietary emulsifiers—specifically carboxymethylcellulose (CMC) and polysorbate 80, prevalent in UK supermarket staples—and the thinning of the colonic mucus bilayer. Mechanistically, these amphiphilic molecules disrupt the hydrophobic interactions between mucin fibres, effectively dissolving the protective gel. This erosion facilitates the direct translocation of pathobionts and dietary antigens across the epithelial interface. Once the mucosal scaffolding is compromised, the anatomical integrity of the tight junction complexes, involving proteins such as claudin-1 and occludin, is disrupted. This 'leaky' state triggers an inflammatory cascade within the lamina propria, driven by the activation of Toll-like receptor 4 (TLR4) and the subsequent nuclear translocation of NF-κB, leading to the systemic release of pro-inflammatory cytokines like TNF-α and IL-6.
Furthermore, the chronic fibre deficiency inherent in the modern UK diet exacerbates this erosion through a mechanism of microbial "auto-cannibalism." As evidenced in *Nature*, when fermentable polysaccharides are absent, the gut microbiota undergoes a metabolic shift, upregulating the expression of mucin-degrading glycoside hydrolases. Essentially, the microbiome begins to catabolise the host’s own mucosal lining as a primary carbon source. This anatomical thinning is not merely a localised gastrointestinal issue; it is the foundational precursor to the UK’s escalating rates of metabolic syndrome, Type 2 diabetes, and inflammatory bowel disease (IBD). The erosion of the mucosal membrane represents a fundamental breakdown of the biological frontier, where the internal systemic environment is no longer shielded from the increasingly hostile chemical milieu of the modern food supply. Through the lens of INNERSTANDIN, we identify this as a silent, structurally-mediated public health crisis that necessitates a total re-evaluation of British nutritional standards and food manufacturing protocols.
Protective Measures and Recovery Protocols
The restoration of the mucosal barrier requires a multi-phasic biochemical strategy that moves beyond simplistic dietary supplementation, targeting the intricate architecture of the glycocalyx and the underlying tight junction (TJ) complexes. In the context of the UK’s escalating prevalence of inflammatory bowel pathologies—exacerbated by a diet high in ultra-processed emulsifiers like carboxymethylcellulose—the primary objective of any recovery protocol must be the re-establishment of the MUC2 mucin bilayer. At INNERSTANDIN, we recognise that the erosion of this barrier is not merely a localised event but a systemic failure of the immunological interface. To counteract this, pharmacological-grade nutritional interventions must focus on the upregulation of trefoil factors (TFFs) and the stabilisation of hypoxia-inducible factor (HIF-1α), which are critical for epithelial restitution.
Evidence published in *The Lancet Gastroenterology & Hepatology* highlights the indispensable role of Short-Chain Fatty Acids (SCFAs), particularly butyrate, as the primary metabolic fuel for colonocytes. Butyrate does not merely provide adenosine triphosphate (ATP); it acts as a histone deacetylase (HDAC) inhibitor, promoting the expression of genes responsible for the assembly of claudin-1 and occludin. A robust recovery protocol must, therefore, prioritise the fermentation of high-viscosity soluble fibres and resistant starches—substrates that are critically deficient in the standard British diet (where average fibre intake remains significantly below the 30g/day recommendation set by Public Health England). This fermentation process lowers the luminal pH, creating a physicochemical environment that inhibits the proliferation of pathobionts such as *Adherent-invasive Escherichia coli* (AIEC), which are known to proteolytically degrade the protective mucus layer.
Furthermore, the molecular repair of the paracellular pathway necessitates the deployment of specific amino acid precursors. L-glutamine serves as a non-negotiable substrate for enterocyte proliferation and the maintenance of the zonula occludens-1 (ZO-1) protein. Research indexed in *PubMed* suggests that glutaminolysis is essential for maintaining the structural integrity of the villi during periods of metabolic stress. Complementing this, the administration of Zinc Carnosine has demonstrated superior efficacy in gastric and intestinal mucosal healing; its unique chelated structure allows it to adhere to denuded mucosal sites, stimulating the migration of epithelial cells to seal erosions.
Finally, a truly exhaustive protocol must address the Aryl Hydrocarbon Receptor (AhR) pathway. The modern diet’s lack of glucobrassicins—found in cruciferous vegetables—deprives the gut of indole-3-carbinol, a vital ligand for AhR activation. At INNERSTANDIN, we posit that AhR signalling is the "homeostatic rheostat" of the gut, essential for the maintenance of intraepithelial lymphocytes (IELs) and the secretion of Interleukin-22 (IL-22). IL-22 is the definitive signal for goblet cell hyperplasia and the production of antimicrobial peptides (AMPs), which act as a secondary chemical shield against systemic endotoxaemia. Without the reactivation of these evolutionary conserved pathways, the mucosal membrane remains in a state of chronic attrition, leaving the systemic circulation vulnerable to the translocation of lipopolysaccharides (LPS) and the subsequent "cytokine storm" characteristic of modern metabolic syndrome.
Summary: Key Takeaways
The systemic degradation of the mucosal barrier—a critical anatomical interface comprising the glycocalyx, the mucus layer, and the underlying epithelial monolayer—represents a burgeoning public health crisis within the United Kingdom. Evidence synthesised from *The Lancet Gastroenterology & Hepatology* and various *PubMed* meta-analyses confirms that the modern Western pattern diet (WPD) serves as a primary driver of mucosal erosion. The mechanism is primarily mediated through the consumption of dietary emulsifiers, such as polysorbate 80 and carboxymethylcellulose, which facilitate the translocation of commensal bacteria through the normally impenetrable *MUC2* protein matrix. This architectural failure results in a marked reduction in transepithelial electrical resistance (TEER), leading to the pathological activation of the zonulin pathway and subsequent "leaky gut" syndrome.
Furthermore, the chronic paucity of microbiota-accessible carbohydrates (MACs) forces colonic microbiota to switch metabolic substrates, actively catabolising the host’s endogenous O-glycans to survive. This autophagic erosion of the protective lining exposes the underlying epithelium to lipopolysaccharides (LPS), triggering systemic endotoxaemia and chronic low-grade inflammation. At INNERSTANDIN, we recognise that this is not merely a digestive issue but a fundamental anatomical collapse. The UK’s disproportionate reliance on ultra-processed foods (UPF) correlates directly with the rising incidence of inflammatory bowel diseases (IBD) and metabolic dysfunction, necessitating a radical shift toward biological literacy to preserve the integrity of our internal frontiers. Only through precise biochemical intervention can the homeostatic balance of the mucosal membrane be restored.
This article is provided for informational and educational purposes only. It does not constitute medical advice, clinical guidance, or a substitute for professional healthcare. Information reflects cited research at time of publication. Always consult a qualified healthcare professional before acting on any health information.
RESEARCH FOUNDATIONS
Biological Credibility Archive
Citations provided for educational reference. Verify via PubMed or institutional databases.
Medical Disclaimer
The information in this article is for educational purposes only and does not constitute medical advice, diagnosis, or treatment. Always consult a qualified healthcare professional before making any changes to your diet, lifestyle, or health regime. INNERSTANDIN presents alternative and research-based perspectives that may differ from mainstream medical consensus — these should be considered alongside, not instead of, professional medical guidance.
Read Full DisclaimerReady to learn more?
Continue your journey through our classified biological research.
DISCUSSION ROOM
Members of THE COLLECTIVE discussing "Mucosal Membrane Erosion in the Modern Diet"
SILENT CHANNEL
Be the first to discuss this article. Your insight could help others understand these biological concepts deeper.
THE ARSENAL
Based on Anatomy — products curated by our research team for educational relevance and biological support.
Panaceum – Prebiotic Oligosaccharide Complex
INNERSTANDING may earn a commission on purchases made through these links. All products are selected based on rigorous educational relevance to our biological research.
RABBIT HOLE
Follow the biological thread deeper